
Abstract
Objective:
Hyperhidrosis can cause dehydration and exercise intolerance. There are several case reports of extremely high sweat rates in athletes. We present as case report of a 17-year-old male with the highest sweat rate recorded in the literature (5.8 L/h). Our goal was to determine if glycopyrrolate, an anticholinergic medication with primarily anti-muscarinic effects that is known to decrease sweat production, would reduce the sweat rate of our subject in a controlled exercise setting.
Methods:
Our patient and a control subject were subjected to an exercise protocol consisting of running on a treadmill (5.4–6.7 mile/h at 1° of incline) in a warm climate-controlled chamber after receiving 0, 2, or 4 mg of glycopyrrolate. Core temperature, heart rate, rater of perceived exertion, and sweat rate were monitored in both subjects.
Results:
Glycopyrrolate dose was not significantly correlated with decreased sweat rate and maximal core temperature. However, the clinical effect of reducing the sweat rate was very strong. The improvement of the subject’s sweat rate allowed him to successfully return to sport.
Conclusion:
Our findings suggest that low-dose glycopyrrolate may be a safe and effective method of controlling exertional hyperhidrosis.
Case report
A 17 year-old male (height: 1.803 m; weight: 83.235 kg; body mass index (BMI): 25.59 kg/m2) high school varsity athlete (football, basketball) was referred to an outside endocrinologist by his primary care provider after an approximate 2-year history of worsening episodes of exercise-induced excessive sweating accompanied by abdominal cramps, headaches, dizziness, occasional blurred vision, and paresthesia throughout his entire body during exercise. His sweating episodes were characterized by a heavy increase in sweating approximately 5 min after the onset of athletic activity. A complete general medical and endocrine evaluation was inconclusive. His comprehensive metabolic panel was within normal limits. His physical examination was unrevealing. The patient subsequently presented to our sports medicine clinic for evaluation of heavy sweating during athletic activities.
Subjective hyperhidrosis (HH) is a reasonably common clinical complaint, but frequently patients are found to have a normal sweat rate when tested. The first step in our clinical protocol for most patients who complain of excess sweating is to have them exercise in a hot and humid environment and measure their weight pre- and post-workout to get an estimate of their actual sweat rate. This patient ran for 33 min on a warm and humid afternoon (88°F, humidity 65%, heat index 97.5), did not urinate, and demonstrated a 3.2-kg weight loss which calculated to an estimated sweat rate of 5.8 L/h (69.9 mL/kg/h). Following this period of exertion, he had a normal resting heart rate at 70 beats per minute. His sweat pattern appeared normal with sweat noticeable on his head, chest, back, and all four extremities. Post-exertional labs were obtained within 5 min of exercise completion and demonstrated mild acidosis (CO2: 21; anion gap: 19), hyperphosphatemia (5.9 mg/dL), and hyperglycemia (123 mg/dL), but no other electrolyte or acid-base abnormalities. We discussed with the patient and his family the results including the excessively high rate of sweat loss (69.9 mL/kg/h vs normal rate of 10–20 mL/kg/h). We encouraged aggressive fluid resuscitation with sugar and electrolyte sports during prolonged exercise athletic events and continued abstinence from caffeine. We also discussed with the patient the possibility of using an aluminum hydroxide–based antiperspirant diffusely over his body in an attempt to limit the rate of sweating during athletic competitions.
Given the patient’s athletic participation, we also made a plan with the patient to test how glycopyrrolate therapy might alter his body temperature and sweat rates during strenuous physical activity. We obtained institutional review board (IRB) approval (the project was deemed exempt) and informed verbal consent from the patient’s father and verbal assent from the patient for a research protocol to test the patient’s physiologic response to glycopyrrolate therapy when physically stressed in a hot and humid environment.
The patient and one healthy control subject (healthy: 35-year-old male, senior author, A.R.P.) received three different trials of glycopyrrolate therapy 0 mg (Trial 1), 2 mg (Trial 2), and 4 mg (Trial 3). Each subject waited 2 h after each glycopyrrolate administration and then underwent an exercise protocol consisting of running on a treadmill (5.4–6.7 mile/h at 1° of incline) in a warm climate-controlled chamber (87 F, humidity 57%, heat index 92.5) for 30 min. Core temperature (CorTemp® Ingestible Core Body Temperature Sensor), heart rate (Polar® FT-1 Heart Rate Monitor), rate of perceived exertion (RPE), and sweat rate were monitored. Spearman correlations and partial effect sizes were calculated. Glycopyrrolate dose was non-significantly correlated with decreased sweat rate (r = −0.79, p = 0.06; Figure 1) and maximal core temperature (r = 0.60, p = 0.21; Figure 2). However, the clinical effect of reducing the sweat rate was very strong. The improvement of his sweat rate allowed him to successfully return to sport. The effect size of glycopyrrolate dose on sweat rate was high (partial eta-squared = 0.28), but the effect size of glycopyrrolate on core temperature was low (partial eta-squared = 0.07). The patient with HH decreased his sweat rate from 4.4 L/h (53 mL/kg/h) with 0 mg glycopyrrolate to 2.0 L/h (24 mL/kg/h) and 1.8 L/h (22 mL/kg/h) with 2 and 4 mg of glycopyrrolate, respectively (Figure 1). This is in comparison to the control subject with a sweat rate of 2.0 L/h (26.7 mL/kg/h) with 0 mg of glycopyrrolate to 1.4 L/h (18.7 mL/kg/h) and 0.6 L/h (8.0 mL/kg/h) with 2 and 4 mg of glycopyrrolate, respectively (Figure 1). The patient with HH’s core temperature was unchanged between the trials with 0 and 2 mg of glycopyrrolate (38.19°C and 37.96°C, respectively), but increased to 38.65°C with 4 mg glycopyrrolate (Figure 2). The control subject had a similar maximal core temperature response as he was unchanged with 0 and 2 mg of glycopyrrolate (38.43°C and 38.28°C, respectively), but increased to 39.27°C with 4 mg of glycopyrrolate (Figure 2). Neither subject had a significant change in heart rate with 2 or 4 mg of glycopyrrolate compared to 0 mg of glycopyrrolate (Figure 3).

Subject sweat rate as a function of glycopyrrolate dose. Both subjects showed decreased sweat rates with both 2 and 4 mg of glycopyrrolate.
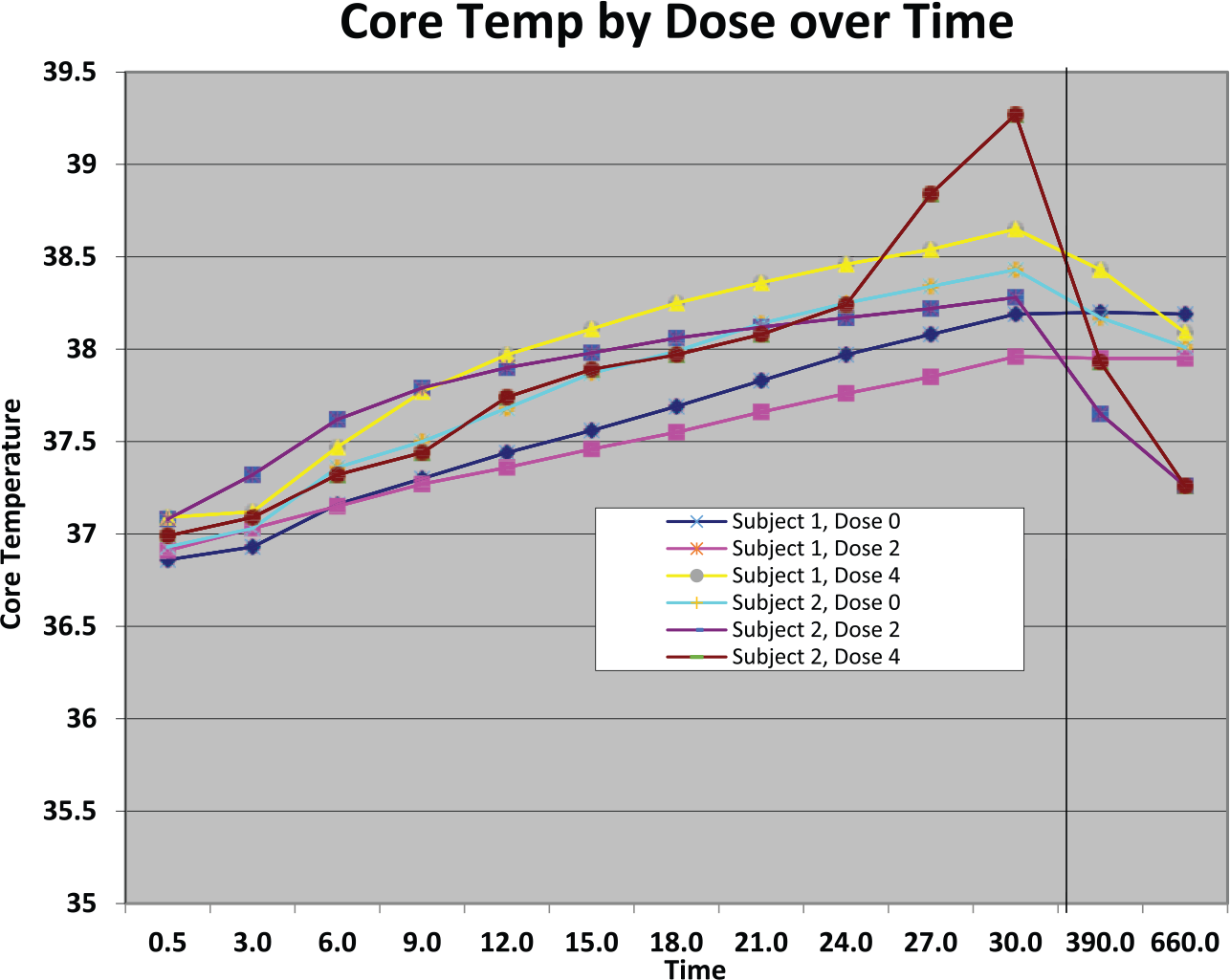
Subject core temperature (°C) on the Y-axis as a function of time and dose of glycopyrrolate. Temperature increased significantly for both subjects with the 4 mg dose of glycopyrrolate and physical exertion.

Subject heart rate (beats per minute) as a function of time (minutes) and dose of glycopyrrolate. Maximum heart rate was not clinically different for each subject when comparing each individual subject across all three glycopyrrolate dosages.
Discussion
Sweat rate and hydration status are important for the exercising athlete and those who are exposed to environments or disease that produce a marked increase in sweat rate. HH, or excessive sweating greater than needed for thermoregulation, has been speculated to exist in 3% of the general population. 1 Hornberger et al. 2 defined diagnostic criteria for primary, focal HH as visible, excessive, focal sweating of at least 6-month duration without apparent cause with at least two of the following also occurring: bilateral and relatively symmetric sweating, frequency of at least one sweating episode per week, impairment of daily activities, age at onset <25 years, positive family history, or cessation of sweating during sleep.
Previous work in the field of exercise physiology has investigated thermoregulation and fluid balance across multiple sports and age groups. Many variables have been shown to influence an athlete’s day-to-day sweat rate including ambient temperature during exercise, exercise intensity, clothing selection, and acclimation to heat.3,4 Factors such as body surface area, body mass, and family history of excessive sweating also contribute to variation of baseline sweat rate between individuals.5–7 Recent studies have quantified sweat rates in adult male athletes across multiple sports, including soccer, football, tennis, and distance running. Mean sweat rates in these trials measured between 1.0 and 2.0 L/h.3,6,8–15 Similarly, adolescent males participating in football, hockey, and soccer were also found to have mean sweat rates in this range.16–19 Professional football players with larger body mass, specifically linemen, were found to have slightly higher sweat rates of 2.11 ± 0.77 L/h. 5 Several case reports of very high sweat rates in athletes exist with the highest sweat rate recorded at 3.9 L/h, in a 19-year-old, 139 kg football lineman. 9
Our case subject, a 17-year-old male high school athlete with excessive sweating that limited his participation and performance in athletic activities, demonstrates the highest sweat rate reported in the literature. His initial sweat rate of 5.8 L/h is nearly twice that of the previous high mark and his rate of 4.4 L/h obtained in a more controlled setting is still much higher than other reports of extreme HH. Although the patient is male, making him more likely to sweat, his negative work-up for neurologic and endocrine abnormalities and his BMI of 25.2 make it unlikely his marked increase in sweat rate was due to other previously proposed causes of excessive sweating with athletic activity. This relative increase in sweat rate compared to previous case reports and case series is most likely accounted for by the patient’s underlying idiopathic HH in conjunction with athletic activity.
Given the extent of our subjects HH and debilitating symptoms, we trialed low-dose glycopyrrolate in an attempt to alleviate his symptoms. Glycopyrrolate is the generic drug name for the molecule glycopyrronium bromide, a synthetically derived anticholinergic with primarily anti-muscarinic effects. It is commonly used clinically to decrease airway secretions and block the anti-muscarinic effects of other drugs. Glycopyrrolate also decreases sweat production and previous reports found that up to 79% of patients have a statistically significant decrease in perspiration following oral administration of glycopyrrolate.7,20,21
Previous literature has concluded that sweat sodium concentration increases linearly as sweat rate increases.22,23 Buono et al. 24 used in vivo testing to demonstrate that the absolute rates of both sodium secretion and reabsorption increase linearly with increases in sweat rate; however, sodium secretion increases faster. Previous work has also reported dehydration (−4.9% ± 0.2% body weight) in competitive cyclists during 2 h of exercise caused hyperthermia (esophageal temperature of 39.3°C) and a phenomenon where cardiac output and blood pressure declined significantly (18% and 5%, respectively), while systemic vascular resistance increased and skin blood vessels vasoconstricted. 25 It has also been shown that dehydration (−4% body weight) and hyperthermia elicit a synergistic effect and, when presenting together, reduce stroke volume by more than double while also increasing systemic vascular resistance by five times compared with either dehydration or hyperthermia alone.26,27 Both the patient and the control subjects in this study demonstrated decreased sweat rates (HH patient: −2.4 L/h; control subject: −0.6 L/h) while also maintaining their core temperature in non-elevated states with low doses of glycopyrrolate (2 mg). The decrease in sweat rates in this study did not reach statistical significance. However, the decrease in sweat rate was large and clinically significant to the patient. That being said, the effects of treatment on a single patient are not generalizable.
This study found no clinical difference in heart rate between the three different levels of glycopyrrolate for either subject (Figure 3). However, cardiac output and blood pressure were not directly monitored. We feel these findings suggest the need for further study and inquiry into the use of low-dose glycopyrrolate to decrease sweat rates while maintaining core body temperature. Additionally, we suggest that it is at least plausible that by decreasing sweat rates, low-dose glycopyrrolate could potentially alter previously cited deleterious downstream physiologic effects of high sweat rates and dehydration.
The HH patient in this study reported no side effects at 0 or 2 mg of glycopyrrolate and mild abdominal pain at 4 mg. It should be noted that the patient gave a history of mild abdominal pain with athletic activity at baseline. The healthy control subject had no symptoms at baseline and at both 2 and 4 mg of glycopyrrolate therapy experienced dry mouth. As previously mentioned, both the patient and the healthy control subject in this study were found to have clinically relevant decreased rates of sweating with low-dose glycopyrrolate while no associated increases in core temperature were observed. At higher doses of glycopyrrolate therapy (4 mg), a further reduction in sweat rate compared to results after 2 mg of glycopyrrolate was noted in both subjects (HH patient: −0.2 L/h; control subject: −0.8 L/h); however, a concomitant rise in core temperature was noted at 4 mg of glycopyrrolate (HH patient: +0.69C; control subject: +0.99C). These findings are consistent with previous work, 28 and we acknowledge that though our work here appears to validate that glycopyrrolate is relatively safe when administered at lower doses, higher doses of glycopyrrolate are problematic clinically as the associated rise in core temperature could be detrimental to the patient. When considering glycopyrrolate as a therapy for exertional HH, we suggest the clinician should consider previous work which has found limited effect of the drug (79%7,20,21), a wide range of drug bioavailability (1%–13%29–31), and the potential to increase the patient’s core body temperature if the drug is inappropriately administered.
Conclusion
For this patient with HH and one additional control subject, a single 2 mg dose of glycopyrrolate 2 h before exercise in a warm environment decreased sweat rate without an increase in maximal core temperature. Our findings support what has been previously reported on the effects, dose–response receptor affinity, and pharmacokinetics of glycopyrrolate. We conclude that low-dose glycopyrrolate may be safe and effective for treating HH in athletes, but further study is needed to establish optimal dosing to maximize sweat reduction while minimizing the side effects associated with glycopyrrolate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series. The work was deemed exempt by the University IRB.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for anonymized patient information to be published in this article.