
Abstract
Objectives:
Despite restrictions, mercury continues to pose a health concern. Mercury has the ability to deposit in most parts of the body and can cause a wide range of unspecific symptoms leading to diagnostic mistakes.
Methods and results:
We report the case of severe mercury vapour poisoning after occupational exposure in a chloralkali plant worker that resulted in life-threatening respiratory failure, pneumomediastinum and quadriparesis.
Conclusions:
Prolonged mechanical ventilation and treatment with penicillamine and spironolactone was used with successful outcome.
Keywords
Introduction
Metallic mercury is liquid at room temperature and easily transforms to vapour. When inhaled, mercury vapour is well absorbed through the lungs and distributes to all tissues. In the bloodstream, most of elemental mercury is oxidized to an ionic form, which binds to sulphur-containing amino acids and interferes with the function of sulfhydryl enzymes leading to disruption of metabolic cellular functions.1–3
According to the Minamata Convention on Mercury established in 2013 and European Community regulations, occupational exposure to mercury should be restricted. 4 This applies particularly to chloralkali plants where metallic mercury was employed in electrodes in the electrolytic production of chlorine and sodium hydroxide. 5 Unfortunately, during the period of transition to mercury-free technology, chemical plant workers could still be exposed to mercury vapour.
Case report
A 31-year-old man, who had been working for 2 months in chloralkali mercury electrolysis plant, developed signs and symptoms of fatigue, dizziness, profuse sweating, tremor of hands and calves, burning and freezing sensations in the feet followed by maculopapular rash on the extremities and body. He was diagnosed and treated by a family doctor, an occupational medicine physician, and hospitalized for 4 days in a regional hospital, where elevated liver transaminases, an enlarged liver and nonsignificant hyponatremia were found (Table 1). The consulting toxicology specialist excluded acute mercury vapour poisoning.
Laboratory data obtained on admittance to the general hospital and the university hospital.

Hgb: haemoglobin; Hct: haematocrit; WBC: white blood cell; PLT: platelet.
After 2 months of the onset of symptoms, he was admitted to the university hospital with dizziness, tremor, ataxia, dysarthria, dysphagia, urinary and stool retention, diminished deep tendon reflexes and hyponatremia (126 mmol/L). His previous medical history was unremarkable, and he denied tobacco, alcohol or illicit drug use. Encephalopathy and polyradiculoneuropathy of unknown aetiology were diagnosed; a urine sample for mercury test was sent to a certified laboratory and extensive neuro-diagnostic tests were performed (Table 2).
Neuro-diagnostic tests performed during the hospital stay.
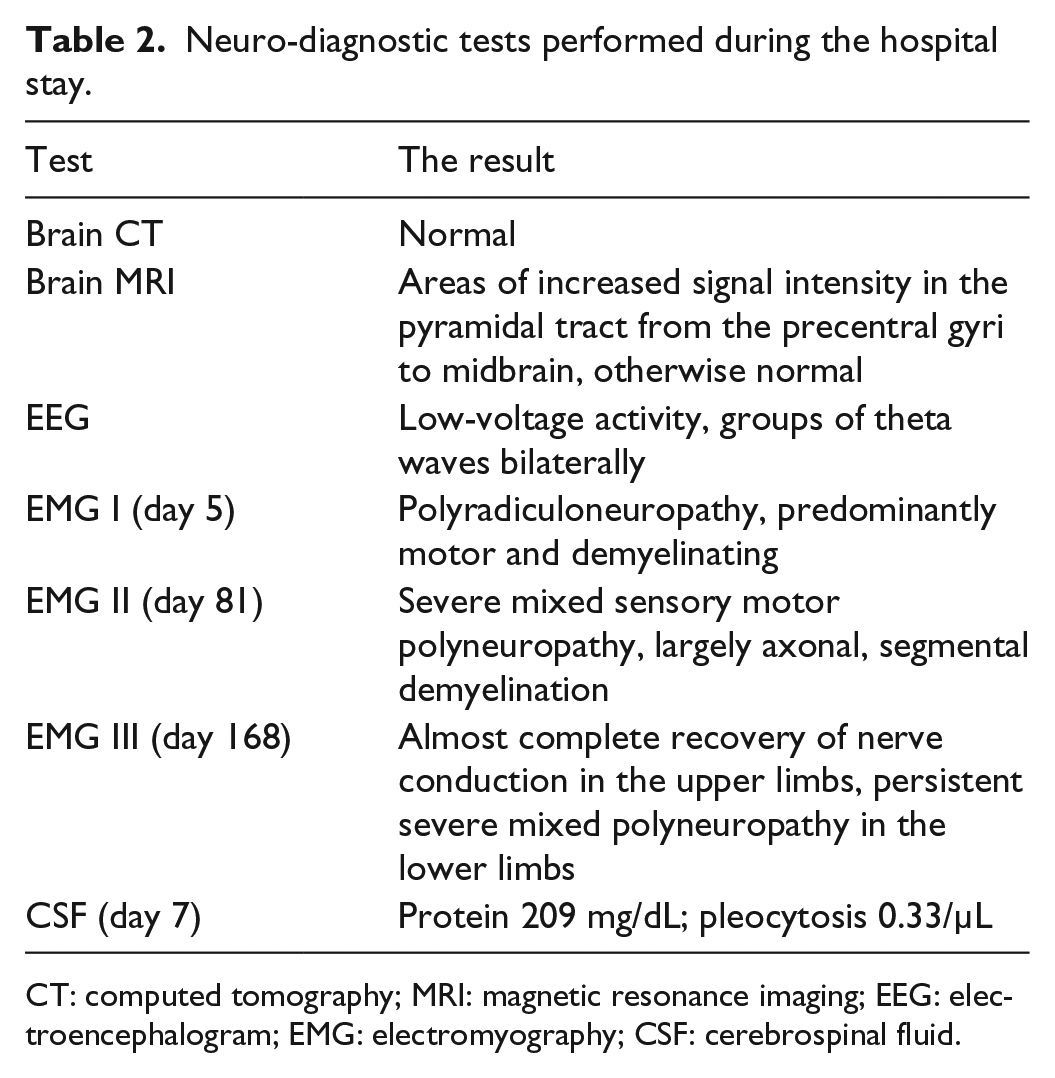
CT: computed tomography; MRI: magnetic resonance imaging; EEG: electroencephalogram; EMG: electromyography; CSF: cerebrospinal fluid.
Due to the progression of symptoms: increased extremity paresthesias with burning sensation of the soles, peripheral facial nerve neuropathy and progressive lower extremity weakness, antiviral, antibiotic and intravenous immunoglobulin treatment was used. On the 28th day of hospitalization, acute respiratory failure developed; the patient was intubated and mechanical ventilation was started. At this time, the result of the urine mercury level test (317.2 µg/L, normal values < 5 µg/L) was received from the laboratory (Table 3) and chelation therapy with penicillamine 250 mg every 6 h was started. The patient was transferred to the intensive care unit (ICU) and treatments with continuous venovenous hemodiafiltration for 9 days and 2,3-dimercaptopropane-1-sulfonate (DMPS) 250 mg intravenously every 12 h for 4 days were added in hope of increasing the rate of mercury elimination.
Urine mercury concentration in the course of treatment (the atomic absorption spectrometry method, reference values <5 µg/L).

On admission to the ICU, crackles of subcutaneous emphysema were palpable on the neck, and pneumomediastinum was detected on the chest X-ray (Figure 1). The finding was confirmed by a computed tomography (CT) scan which showed an 8-mm wide pneumomediastinum, subcutaneous emphysema of the neck together with atelectasis and consolidation in the lower segments of the left lung (Figure 2).

Plain chest X-ray showing linear air lucency on the left border of mediastinum (arrows) and subcutaneous emphysema in the supraclavicular area and the neck.

(a) Axial and (b) coronal CT scans demonstrating pneumomediastinum and subcutaneous emphysema in the neck (arrows).
A subsequent endoscopic examination revealed thick, purulent secretions in the bronchi with no signs of damage to the bronchi or oesophagus. Mechanical ventilation was used for almost 5 months before he was successfully weaned off the ventilator. A control CT scan performed 2 weeks later showed complete resolution of the air from the mediastinum and neck and progression of pneumonia in the left lung. Septic shock developed and multiresistant Acinetobacter baumannii was cultured from tracheal secretions. Limb weakness progressed to almost complete tetraplegia, and flaccid paralysis remained unchanged for the next 3.5 months. Only moderate movements of the head and the shoulder girdle and slight flexion of the fingers of the right hand were preserved. He suffered from persistent diarrhoea, recurrent Pseudomonas urinary tract infections and the formation of multiple urinary calculi. Drenching sweats resulted in profound hypovolemia with an incident of transient loss of consciousness.
After 3 months in the ICU, intravenous spironolactone was added to the penicillamine treatment. After 3 weeks, the tetraplegia began to subside, and soon he was able to move all his extremities and stand by the bedside with the assistance. He was also weaned off the ventilator, and the tracheostomy tube was removed. The electromyography (EMG) showed significant improvement in the function of the peripheral nerves of the arms with persistent severe polyneuropathy in lower extremities. The mercury urine concentration decreased to normal level. Upon return to normal gastrointestinal and urinary functioning, he was discharged home after 196 days of hospitalization.
Discussion
Our patient developed clinical manifestations of sub-acute mercury poisoning after being exposed to liquid mercury when cleaning workplace facilities and an electrolysis bath in the chloralkali plant. The possibility of dangerous exposure is easy to overlook as elemental mercury vapour is odourless, heavier than air and has a tendency to accumulate in poorly ventilated or low-lying areas. 6
Mercury can cause a wide range of unspecific symptoms. Initial symptoms of mercury poisoning may mimic a viral illness 7 and can lead to diagnostic mistakes. 3 Due to the non-specific signs and symptoms presented by our patient, the diagnosis of mercury poisoning was delayed until a high mercury concentration in the urine became apparent. The mercury concentration in the urine (317.2 µg/L) significantly exceeded the maximum accepted level for occupational exposure (<30 µg/L), and values >300 µg/L are usually associated with overt symptoms of poisoning. 2
Initial complaints of our patient were mainly attributed to central and peripheral nervous system toxicity. Our patient had electromyographic signs of mixed sensorimotor polyneuropathy that progressed to severe quadriparesis. A similar case of quadriparesis was described by Chu et al. 8 in a man, after prolonged ingestion of herb drugs containing mercuric sulphate. Their patient remained quadriparetic with only minor improvement after a 2-year follow-up. However, signs of polyneuropathy in our patient subsided after 5 months of treatment, and he returned later to normal activity.
Acute massive exposure to vaporized elemental mercury results in the rapid appearance of pulmonary symptoms, with dyspnoea, cough, chest pain, fever, chills and a metallic taste in the mouth.1,2,9 Diffuse pulmonary infiltrates, acute respiratory distress syndrome (ARDS), pneumonia, fibrosis, chemical pneumonitis, bronchiolitis and pneumothorax often resulting in death has been described.10–13 Prolonged exposure results in signs and symptoms in other organs, notably from the central nervous system and kidneys and also the peripheral nerves, immune system, endocrine system, muscles and skin. 3
The respiratory manifestations in the form of pneumomediastinum, pneumonia and respiratory failure developed in our patient after only several weeks from exposure and were not typical for mercury intoxication. Most cases of pneumothorax and pneumomediastinum in the course of mercury vapour poisoning have been reported in children12,14,15 and very few in adults. 16
Signs of autonomic dysfunction in our patient were manifested by tachycardia, profuse sweating, diarrhoea and abdominal pain. Some of those signs are presumed to be the effect of the inhibition of catecholamine degradation by mercury.7,17
The mainstay of treatment of mercury poisoning is chelation therapy. Penicillamine was used in our patient for almost 6 months. Based on sparse reports suggesting the ability to restore impaired metabolism, 18 spironolactone was added to the penicillamine therapy. Spironolactone administration coincided with the sudden improvement of neurological function that ensued 3 weeks later.
To conclude, we hereby presented a case of mercury vapour poisoning after occupational exposure resulting in prolonged respiratory failure, pneumomediastinum and quadriparesis with excellent outcome. Insidious onset and non-specific clinical manifestations of mercury poisoning can lead to diagnostic mistakes. Physicians should be aware of mercury vapour poisoning especially after occupational exposure.
Footnotes
Acknowledgements
The authors are pleased to acknowledge the Department of Radiology for provision and interpretation of diagnostic imaging results.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for the publication of this case report.