
Abstract
Hypogammaglobulinemia is a known side-effect of rituximab use. It is typically asymptomatic and transient, although certain factors, such as maintenance dosing and concomitant glucocorticoid use can lead to symptomatic or prolonged hypogammaglobulinemia. Patients with symptomatic hypogammaglobulinemia leading to recurrent infections may be treated with intravenous immunoglobulin therapy. Herein, we report a case of a 49-year-old male on maintenance rituximab without prior respiratory symptoms with new onset recurrent pneumonia after COVID-19 pneumonia and treatment with glucocorticoids.
Introduction
Rituximab is a monoclonal antibody that targets the CD20 receptor found on the surface of circulating peripheral B-cells and is commonly used in lymphoproliferative disorders and autoimmune diseases. 1 Although immunoglobulin levels should theoretically be unaffected since CD20 receptors are not found on mature plasma cells, many patients develop a self-limiting hypogammaglobulinemia most likely secondary to depletion of pre-plasma B-cells. 2 Because of this effect, rituximab use has been associated with a reduced response to vaccines, reactivation of viral infections, and an increased susceptibility to bacterial infections. 3 This hypogammaglobulinemia is usually transient; however, some patients demonstrate persistent hypogammaglobulinemia, defined as decreased immunoglobulins for >6 months following discontinuation of rituximab. 1 This complication is seen in 39%–42.2% of patients on rituximab and is typically asymptomatic. 1 Symptomatic hypogammaglobulinemia is defined as two or more non-neutropenic infections within 6 months of rituximab treatment that requires immunoglobulin replacement therapy. 1 It is most common in patients undergoing autologous hematopoietic stem cell transplants (16.7% of patients), most likely due to the higher level of immune suppression and longer period of immune reconstitution in these patients. 1 Risk is also increased with the concomitant use of glucocorticoids and an increased number of doses of rituximab.1,4 In a study by Parmentier et al., 5 they also found that those with low baseline IgG levels had a higher risk of hypogammaglobulinemia during treatment with rituximab and persistence after discontinuation.
The most common infections due to hypogammaglobulinemia include sinopulmonary infections, upper respiratory infections, and pneumonia. 4 Less common infections include soft tissue infections and viral infections with HSV, VZV, and CMV. 3 Given the increased risk of recurrent infections, measurement of immunoglobulin levels has been recommended prior to and during rituximab therapy to identify patients who may benefit from IVIG therapy. 2 With the COVID-19 pandemic, some studies have been performed to see how patients with hypogammaglobulinemia are affected. In a study consisting of 17 patients with hypogammaglobulinemia, they found patients experienced prolonged COVID-19 symptoms with a median symptom course of 56 days and positive RNAemia measured by polymerase chain reaction (PCR) during this time. 6
Case report
The patient is a 49-year-old male with a past medical history of mantle cell lymphoma treated with autologous stem cell transplant in 2017 and maintenance rituximab until July 2020. He was initially hospitalized for 2 days with COVID-19 pneumonia in November 2020. He had no prior history of pneumonia while on rituximab therapy. From November 2020 to March 2021, he was hospitalized four times for recurrent shortness of breath and fever, for which he was diagnosed with recurrent pneumonia based on his clinical symptoms and pulmonary infiltrates on chest imaging. The patient had an extensive infectious disease workup throughout this time, which was negative, including for recurrent COVID-19 infection. During each case, he was treated with antibiotics and steroids with improvement in symptoms, but his respiratory symptoms returned within a few days upon discontinuing steroids and antibiotics. The patient also reported daily fevers, chills, night sweats, decreased appetite, and a 35-pound weight loss over the past 4 months.
The patient presented to our facility in March 2021 with recurrent shortness of breath and fever of 102°F. A chest x-ray revealed multifocal pulmonary opacities concerning for cryptogenic organizing pneumonia or interstitial pneumonia (Figure 1). He also underwent computed tomography (CT) angiography which showed patchy bilateral lung infiltrates and interstitial thickening concerning for pneumonia with pulmonary edema (Figure 2). Infectious disease workup was negative, including gram stain, respiratory culture, fungal culture, AFB smear and culture, blastomycosis, histoplasmosis, pneumocystis, legionella, and aspergillus. The patient also underwent a bronchoscopy, bronchoalveolar lavage, and lung biopsy, which showed chronic inflammation but was negative for wall cultures and malignancy. Laboratories were significant for hypogammaglobulinemia: IgG 260 mg/dL, IgA 19 mg/dL, and IgM 7 mg/dL. The patient had several risk factors for hypogammaglobulinemia, including a history of immune suppression for hematopoietic stem cell transplant in 2017, maintenance rituximab until July 2020, and multiple short courses of glucocorticoids. The patient was managed with broad-spectrum antibiotics, a reduction in steroid dose, and administration of intravenous immunoglobulins (IVIG).

Anterior-posterior semi-erect chest X-ray showing multifocal pulmonary opacities (arrows).
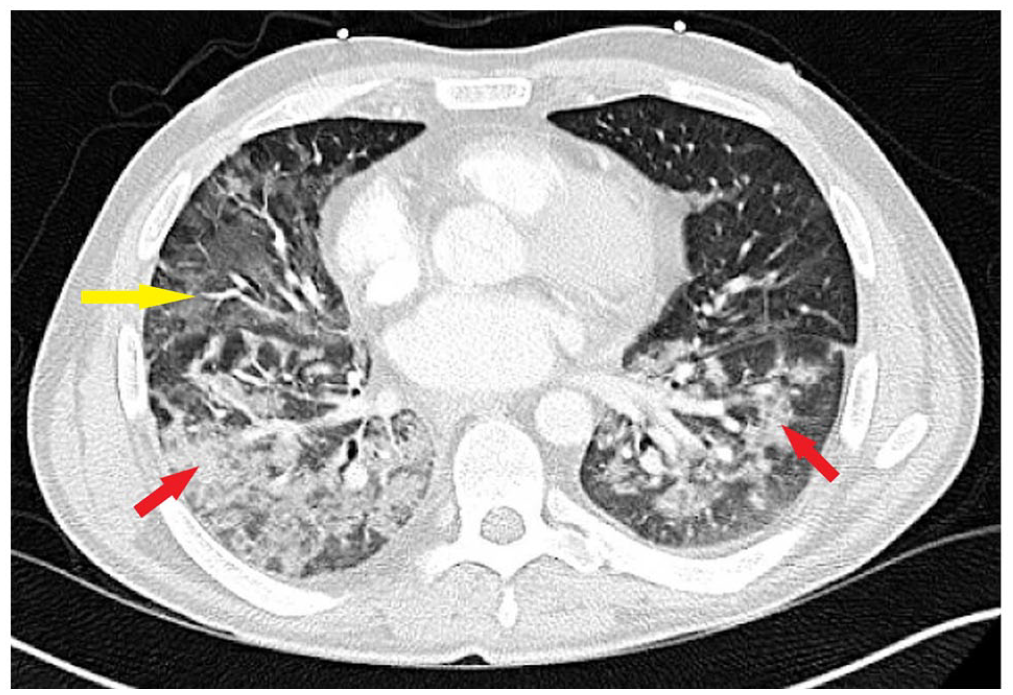
Axial computed tomography angiography showing patchy bilateral ground glass opacifications (red arrows) and focal lung infiltrates (yellow arrow).
At his 1-month follow-up visit, the patient reported marked improvements in his symptoms. He stated he has continued to have some occasional cough and sinus drainage but denied any continued fevers, chills, or night sweats. He also reported improvement in shortness of breath with exertion.
Discussion
Hypogammaglobulinemia is a known adverse effect of rituximab use, which can be exacerbated by glucocorticoid use. Rituximab is particularly prone to causing hypogammaglobulinemia in patients receiving maintenance doses, as seen in our patient. In a study by Casulo et al., 4 they found that hypogammaglobulinemia developed in 54.2% of patients who received maintenance rituximab compared to 32.8% who received rituximab as immunotherapy or chemoimmunotherapy alone. In this study, they also report a significant reduction in the recurrence of infections with the administration of intravenous immunoglobulin (IVIG), the mainstay of therapy. 4
Herein, we report a case of hypogammaglobulinemia in a patient with a history of maintenance rituximab leading to multiple episodes of pneumonia following COVID-19 infection. This is a unique case as the patient had been on maintenance rituximab for 3 years without any infections requiring hospitalization and then became symptomatic following COVID-19 pneumonia. Following his COVID-19 infection in November 2020, he was hospitalized four times and found to have hypogammaglobulinemia. Baseline immunoglobulin levels were not previously evaluated due to his lack of respiratory symptoms. During each hospitalization, the patient was treated with glucocorticoids, a known trigger of symptomatic hypogammaglobulinemia. 7 Glucocorticoids are thought to induce hypogammaglobulinemia by increasing apoptosis of plasma cells and increasing immunoglobulin catabolism; however, this side effect is typically seen in long-term steroid use in doses of 15 mg/day for 1 year. 8 It is also worth noting the patient had negative COVID-19 antibody and PCR testing during his rehospitalizations. In a study by Hueso et al., 6 they found patients with hypogammaglobulinemia had persistent COVID-19 symptoms, but the patients in this study had positive COVID-19 PCR, which was not seen in our patient. Given the recurrent nature of the pneumonia, we query the possibility of altered immunity from COVID-19 infection.
Conclusion
Rituximab is a monoclonal antibody commonly used for autoimmune diseases and lymphoproliferative disorders that targets peripheral B-cells. Hypogammaglobulinemia is a known adverse effect of rituximab use that may lead to recurrent infections. In patients with symptomatic hypogammaglobulinemia or risk factors for hypogammaglobulinemia, such as long-term use, high dosage, concomitant glucocorticoid use, or low baseline immunoglobulin levels, intravenous immunoglobulin use should be considered prior to and during rituximab use. Further investigation is warranted to determine if there is a correlation between hypogammaglobulinemia and persistent respiratory symptoms following COVID-19 infection.
Footnotes
Author’s contribution
C.O. conceptualized and drafted the manuscript with the support of R.E. and S.C. Patient records and images were reviewed by R.E. and S.C. All authors contributed to conceptual refinement and critical manuscript review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.