
Abstract
Anti-N-methyl-D-aspartate receptor encephalitis is a life-threatening medical emergency that can be clinically misperceived as Hashimoto’s encephalopathy. We present a case of anti-N-methyl-D-aspartate receptor encephalitis in an otherwise healthy young female with subclinical hypothyroidism without an associated ovarian teratoma. She was first misdiagnosed as Hashimoto’s encephalopathy due to delirium and behavioral changes, seizures, psychosis, and increased amount of thyroid peroxidase and thyroglobulin antibodies in serum. Final diagnosis was established by third week following presentation with the detection of anti-N-methyl-D-aspartate receptor antibodies in her cerebrospinal fluid. After treatment with intravenous immunoglobulin, methylprednisolone, and amisulpride, she recovered significantly with minimal sequelae at 3-week follow-up.
Keywords
Introduction
Anti-N-methyl-D-aspartate receptor (anti-NMDAR) encephalitis is now considered the most common cause of autoimmune encephalitis after acute demyelinating encephalitis and 80% of patients are women. 1 The autoimmune process was first described in 2007 when Dalmau et al. 2 portrayed the existence of autoantibodies to NR1-NR2 heteromers in 11 women with ovarian teratoma together with neuropsychiatric symptoms. Since then, more than 1000 cases have been reported and the exact incidence of anti-NMDAR encephalitis is unknown. 3
Lately, several cases have highlighted the coexistence of anti-thyroid antibodies with anti-NMDAR antibodies in non-paraneoplastic anti-NMDAR encephalitis. 4 A PubMed search for “((Anti-N-methyl-d-aspartate) OR NMDA) AND thyroid” (on 13 March 2020) identified 69 items addressing this issue, including 14 case reports. Out of these, 10 are positive for thyroid autoantibodies including one case report in 2016 highlighting subclinical hypothyroidism in an elderly lady presenting with cognitive dysfunction in context of overlap syndrome (anti-NMDAR encephalitis with positive thyroid autoantibodies). 5 Here, we present the first documented case, to the best of our knowledge, of a middle age female with subclinical hypothyroidism who presented with autoimmune anti-NMDAR encephalitis associated with positive anti-thyroid peroxidase (TPO) antibodies. We also suggest that amisulpride may work to attenuate the psychiatric symptoms secondary to anti-NMDAR encephalitis.
Case report
The patient was a 35-year-old female without previous psychiatric or medical history. She was brought to the Emergency Department (ED) by her family with a 3-week history of diffuse body malaise and weakness associated with dizziness, shortness of breath, chills, and headache. The patient refused routine blood investigations and left ED against medical advice. Two days later, she was brought back by ambulance after sudden onset of disorganized speech and hallucinatory behavior. Initial laboratory studies showed leukocytosis with neutrophilia. Comprehensive metabolic panel, brain computed tomography (CT) scan, urine toxicology screen, and blood alcohol level were unremarkable. The case was referred to the Consultation and Liaison (CL) Psychiatry service for schizophrenia spectrum mental illness but in view of a recent travel history to Turkey and Oman, agitation, urinary incontinence, and delirium, CL consulted neurology and medical teams. The medical team recommended involuntary admission and patient was followed jointly by medicine, neurology, and psychiatry. The following day she was started on intravenous acyclovir after lumbar puncture (LP) revealed lymphocytosis (Table 1). She rapidly deteriorated and became more disorganized and reported persecutory delusions (e.g. “people are coming to get me and harm me”) associated with both auditory and visual hallucinations (e.g. hears noises and voices of strangers). Nursing staff has observed her whispering and spitting, together with altered level of consciousness.
CSF findings.

CSF: cerebrospinal fluid; GFAP: glial fibrillary acidic protein; IFA: immunofluorescence assay; NMDAR: N-methyl-D-aspartate receptor; VDRL: venereal disease research laboratory.
She was started on intravenous ceftriaxone (in addition to acyclovir) after magnetic resonance imaging (MRI) head showed superior fronto-parietal sulci fluid-attenuated inversion recovery (FLAIR) hyperintensity and mild abnormal contrast enhancement which were suggestive of meningitis (Figure 1). Over the course of the ensuing week, she became increasingly delirious (mixed hyperactive and hypoactive) and started to develop seizure-like activity (twitching of face and abnormal movements of tongue and lips) associated with autonomic instability. Medical intensive care unit (ICU) was onboard for any eventuality. Owing to her declining condition, intravenous immunoglobulin (IVIG) and methylprednisolone were initiated on an empiric basis for anti-NMDAR encephalitis (IVIG was delayed by 2 days as family initially refused). She was also placed on levetiracetam for seizure control. Pan-MRI to assess for any malignancy and remaining blood work were negative except mildly elevated thyroid-stimulating hormone, normal free T4, high anti-TPO, and high anti-thyroglobulin (TG) antibody (Table 2). Her provisional diagnosis was Hashimoto’s encephalopathy (HE) in view of acute onset of altered mental status and elevated anti-thyroid antibodies, in the absence of a central nervous system infection, tumor, or stroke. Endocrinology team started her on levothyroxine. Meanwhile, she has a second LP for autoimmune and infectious screening. Encephalopathy autoimmune cerebrospinal fluid (CSF) evaluation was sent abroad as it not available locally. Given her repeated bouts of agitation and administration of antipsychotic agents, a creatinine phosphokinase and myoglobin levels were ordered, which were slightly elevated at 324 U/L and 131 ng/mL. When evaluated by CL service, the patient was noted to exhibit catatonic features such as echolalia, waxy flexibility, and catalepsy. She was also very psychotic (she believed that the devil is spying on her through cameras, that her neighbors are going to harm her) and agitated, in addition to abnormal perceptual disturbances such as tactile hallucinations. Olanzapine was prescribed for psychotic symptoms and lorazepam for catatonia and agitation.
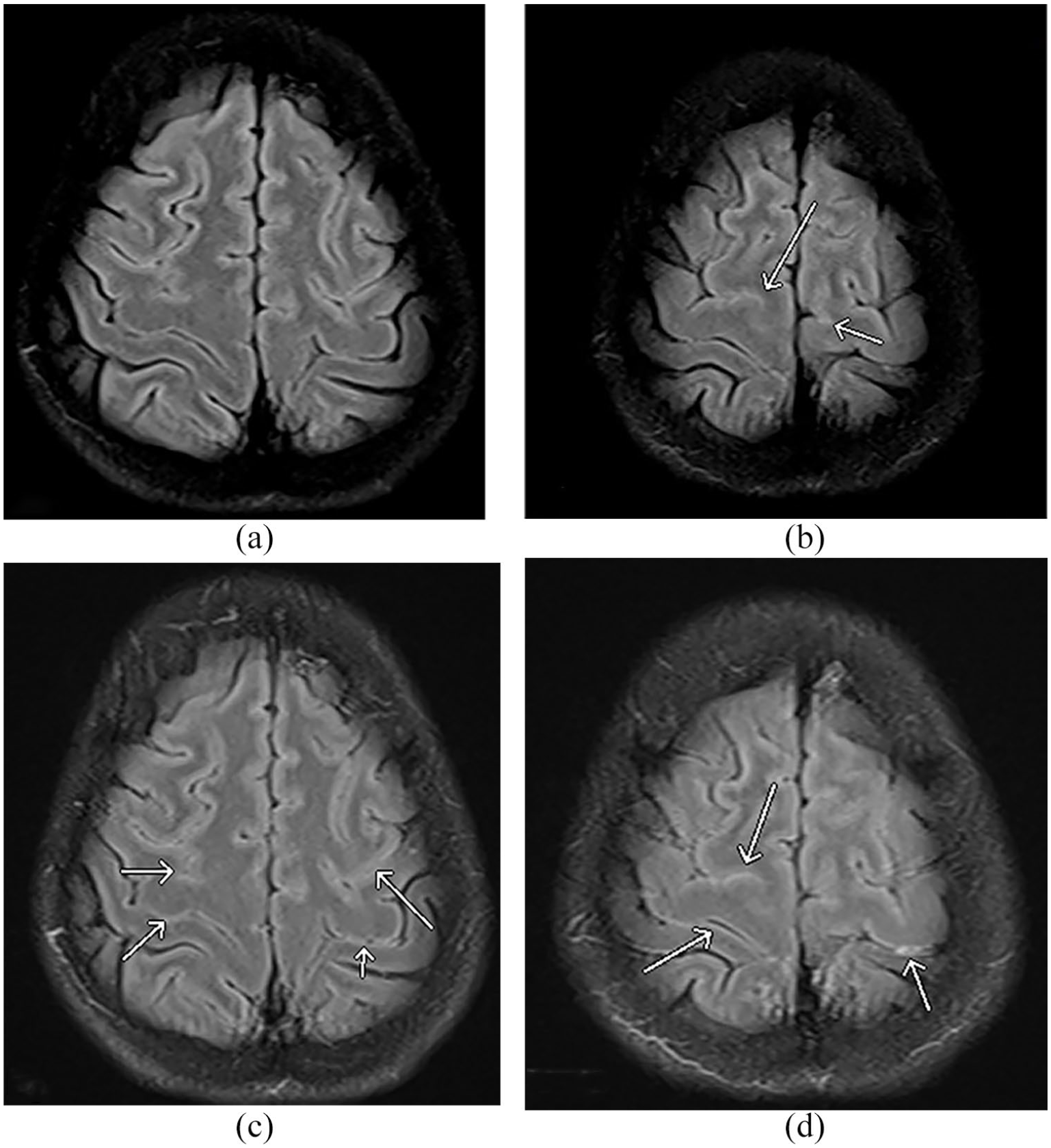
Magnetic resonance imaging (MRI) of brain with axial fluid-attenuated inversion recovery (FLAIR) sequence (a, b) non-contrast images and (c, d) post-contrast. (a, b) Subtle hyperintense superior convexity fronto-parietal sulci. (c, d) Mild abnormal contrast enhancement of the same superior convexity fronto-parietal sulci suggestive of meningitis.
Neuroimaging and other investigations.

CT: computed tomography; MRI: magnetic resonance imaging; US: ultrasound; EEG: electroencephalogram; FDG: fluorodeoxyglucose; FLAIR: fluid-attenuated inversion recovery; XR: X-ray.
By the third week, she has shown minimal improvement after a course of antibiotics, 5-day course of IVIG and methylprednisolone, levothyroxine, and antipsychotics. Medical team ordered whole body fluorodeoxyglucose positron emission tomography/CT (FDG PET/CT) Table 2 to further evaluate a possible paraneoplastic encephalitis. Results showed no FDG avid pathology except relatively increased FDG uptake in the right superior fronto-parietal brain, the same area which showed mild abnormal findings on previous MRI. Neurology changed levetiracetam to valproate as they suggested that levetiracetam could exacerbate agitation. A few days later, CSF anti-NMDAR antibodies returned with a positive result, confirming the diagnosis. Neurology did not proceed with rituximab which is the second-line therapy for anti-NMDAR encephalitis because of deranged liver function tests. Accordingly, CL team changed olanzapine to amisulpride which is a renally excreted antipsychotic with no hepatic metabolism. In a matter of days, she improved significantly in terms of clearer sensorium with better focused attention and much lesser bouts of agitation and psychosis. Her psychotic symptoms and hallucinations drastically resolved. She was able to communicate and was independent in her activities of daily living (ADL). Her family agreed to discharge to home with 24-h supervision, and she returned home approximately 42 days after her initial presentation. At her outpatient medicine follow-up, 7 days after her discharge, her liver function test (LFT) was back to normal and was described as “stable but with bloating symptoms and heart burn.” One week later at outpatient neurology clinic, she was described as “markedly improved, alert and fully oriented, communicating appropriately, drives her car independently, no evidence of seizure.” Family members reported bouts of anger and irritability. Her gastrointestinal symptoms were explained by prednisolone which was tapered to 20 mg daily and levetiracetam was discontinued as no evidence of seizure since discharge. Patient was offered an appointment in the neurology outpatient clinic after 2 weeks to aim at discontinuing prednisolone. Figure 2 illustrates the patient’s timeline of events in chronologic detail.

Timeline of events.
Discussion
Our patient was initially referred to Psychiatry CL team for her marked disorganized behavior which could be easily mistaken for symptoms of schizophrenia. Clinical symptoms of anti-NMDAR encephalitis may mimic schizophrenia and psychotic spectrum disorders; hence, it is so frequent for these patients to be initially seen and evaluated as new-onset psychosis. 1 In our case, schizophrenia was ruled out as she did not have prodromal symptoms such as avolition or social withdrawal, in addition to negative family history of mental illness and presence of insight into her unusual thoughts. In light of her recent travel history and acute deterioration, substance-induced psychosis was also considered; however, her symptoms worsened even in the absence of substance use which makes this differential diagnosis very much least likely. The differential diagnosis also includes other viral encephalitides, other autoimmune causes, and toxic/metabolic disorders. 6
Thyroiditis, including Graves’ disease and Hashimoto’s thyroiditis, has recently come to light as a potential etiology of autoimmune encephalitis. The presence of thyroid autoantibodies in non-paraneoplastic anti-NMDAR encephalitis was first described in 2010. 7 Among the 10 case reports positive for thyroid autoantibodies from our literature search, five cases depicted a clinical picture of hyperthyroidism. The only case illustrating subclinical hypothyroidism and elevated thyroid autoantibodies (anti-TPO >3000 U/mL and anti-TG 92 U/mL) is that of a 70-year-old woman presenting with confusion, cognitive dysfunction, mood changes, and goiter. 5 She was initially diagnosed with HE which is comparable to our case as HE can present with neurocognitive changes, seizures, and psychiatric symptoms. 4 However, due to lack of response to corticosteroid, another possible cause of the encephalopathy was considered and tests for antibodies to the NMDAR were found positive. The main difference in our case was the age group and the symptomatology. Our patient was a healthy middle age female with prodromal viral-like illness for 2 weeks presenting to hospital after she developed psychotic symptoms and disorganized thought process and behavior. As the disease progressed, her presentation began to differ from that of typical psychosis with the onset of autonomic dysfunction, seizures, and movement disorders. Within the same period of time, she developed catatonia with multiple episodes of agitation. In hindsight, she showed typical clinical presentation of anti-NMDAR encephalitis as seen in 70% of patients.6,8
Nonetheless, it is worthwhile to mention that one autoimmune disease (AD) increases the chance of an additional AD. 9 Although ADs may co-develop in one patient, it is not a frequent phenomenon. In a recent study on coexistence of autoimmune encephalitis and other systemic ADs, the authors found that out of 307 anti-NMDAR encephalitis cases, 16 patients had concomitant ADs, including 11 with positive anti-thyroid antibodies. In addition, they also report concomitant ADs such as systemic lupus erythematosus, chronic urticaria, and anaphylactoid purpura. 10
In our literature review, we found two cases which were misdiagnosed for HE which consequently led to the delay in the final diagnosis of anti-NMDAR encephalitis by 6 months to 4 years in an 18-year-old female and 14-year-old girl, respectively.11,12 We minimized delays in both assessment and treatment by repeating LP on day 7 to test the CSF for anti-NMDAR antibodies because it is more sensitive than serum antibodies (100 versus 85.6% sensitivity). 13
After screening for teratoma or germ cell tumors, she was started on concurrent IVIG (0.4 g/kg per day for 5 days) and methylprednisolone (1 g per day for 5 days) instead of plasma exchange as a recent study seems to favor the former. 14 However, the patient’s psychiatric symptoms were not alleviated after immunotherapy, thyroxine, and various psychotropics such as haloperidol, lorazepam, and olanzapine. Furthermore, she developed drug-induced hepatitis (ALT 1455 U/L, AST 139 U/L, Alk Phos 110 U/L, and normal bilirubin) and the Medical Team suspected either valproate or olanzapine as the causing agent. Deranged LFTs also precluded the initiation of second-line therapy such as rituximab. Even though hepatotoxicity is an infrequent complication of second-generation antipsychotic, she was shifted to amisulpride 200 mg tablet daily as there are case reports that highlight the worsening of psychiatric symptoms with olanzapine.15,16 Present-day, there is no established antipsychotic treatment strategy for anti-NMDAR encephalitis with psychiatric symptoms. We suggest that amisulpride may work in context of subclinical hypothyroidism if the psychiatric symptoms could not be controlled after immunotherapy and thyroid replacement.
Conclusion
Anti-NMDAR encephalitis is a threatening, potentially lethal condition that is often initially confused with HE, schizophrenia spectrum mental illness, or substance-induced psychosis. While the topic of this article is not too novel, even so, as a relatively newly understood entity this case report contributes to the growing body of literature by highlighting the timeline of symptoms seen over the course of the illness and the management of psychiatric symptoms by amisulpride, as well as the coordination of psychiatry, neurology, endocrinology, and internal medicine services in diagnosing and managing this complex disease.
Footnotes
Acknowledgements
The authors thank Dr Mohamed Mohamed Helmi Ahmed, Associate Consultant Radiologist at Hamad Medical Corporation, for his input on MRI imaging.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the Medical Research Center of Hamad Medical Corporation (MRC-04-20-163).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication of this article was funded by the Qatar National Library.
Informed consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.