
Abstract
Objectives:
This meta-analysis aims to synthesize the available data on the effectiveness of hamstring stretching exercises in relieving pain intensity and improving function for patients with low back pain.
Methods:
Google Scholars, PubMed, Embase, Cochrane, MEDLINE, CNKI, Wanfang, and VIP were searched from inception to August 2023. We included randomized controlled trials that investigated the effectiveness of hamstring stretching exercises in patients with low back pain. The primary outcomes assessed were pain intensity, hamstring muscle flexibility, and function. Study selection, data extraction, and assessment of risk of bias were performed independently by two reviewers.
Results:
Our searches retrieved 344 trials, of which 14 met the inclusion criteria for this review (n = 735 participants). The combined meta-analysis showed hamstring stretching resulted in lower pain scores (standardized mean difference = −0.72, 95% confidence interval: −1.35 to −0.09; I2 = 89%, p = 0.03) in different categories of low back pain. Subgroup analysis showed that hamstring stretching led to a larger range of motion for cases of back pain with radiating pain (standardized mean difference = 2.39, 95% confidence interval: 1.76 to 3.02; I2 = 0%, p < 0.001). The combined meta-analysis revealed that hamstring stretching resulted in lower Oswestry Disability Index scores in comparison to regular treatment, particularly in individuals suffering from low back pain across all subtypes (mean difference = −6.97, 95% confidence interval: −13.34 to −0.60; I2 = 95%, p = 0.03).
Conclusions:
This meta-analysis demonstrates the effectiveness of hamstring stretching exercises in reducing pain intensity in various categories of low back pain and improving the straight leg raise in patients experiencing back pain with radiating pain. Additionally, it highlights the improvement in function for patients with back pain across all subtypes.
Introduction
Low back pain (LBP) affects a staggering 568 million individuals, resulting in 64 million disability-adjusted life years each year. 1 Moreover, the first global estimate of the need for rehabilitation, published in The Lancet by the World Health Organization, reveals that LBP carries the largest burden of disease on a global scale. 1
The Lancet articles on LBP reported the effectiveness of exercise therapy (of any kind) in the treatment of nonspecific LBP. 2 Stretching exercises are recommended for the treatment of LBP, particularly for individuals with hamstring tightness.3,4 A lot of evidence supported that hamstring tightness was one of the causes for the development of LBP.5 –10 Many clinicians 11 support these findings in clinical practice, as they believe that normal hamstring flexibility can help prevent excessive lumbar flexion during postures that elongate the hamstrings, such as forward bending, using the lumbar-pelvic rhythm (LPR) theory. Previous studies reported the effectiveness of hamstring stretching exercise for LBP patients.4,12 However, other studies indicate that performing hamstring stretching exercises solely results in an improvement in hamstring muscle length rather than other aspects of functionality among individuals suffering from LBP. 13 The disparate results could potentially be attributed to the varying effectiveness of hamstring stretching exercises across different subtypes of LBP. Therefore, our objective is to examine the impact of hamstring stretching exercises on different subtypes of LBP, utilizing the International Classification of Functioning, Disability, and Health (ICF) model.
The ICF serves as the globally recognized standard for guiding the clinical assessment and intervention for LBP. 14 The ICF categorizes LBP into several subtypes including back pain with mobility deficit, back pain with referred pain, back pain with radiating pain, and back pain with movement coordination impairments. ICF provides an exclusive set of categories, which serves as reference units for the standardized reporting of functioning. 15 Though ICF is widely accepted, its implementation into clinical practice is still limited. 15 Interventions guided by the ICF model hold significant importance in clinical practice.
The significance of this article lies in evaluating the effects of the hamstring stretching exercises for different subtypes of LBP based on the ICF model. The objective is to determine the clinical applicability of this intervention and provide evidence-based support for clinical management.
Methods
Study design
A systematic review and meta-analysis was conducted to estimate the effects of hamstring stretching exercises on pain intensity and function in LBP Patients. This study was registered using the international prospective register of systematic reviews PROSPERO on 4 November 2019 with the corresponding reference number CRD42019146162. The study spans from November 2019 to August 2023. This systematic review adhered to the PRISMA 2020 guidelines for reporting.
Eligibility criteria
The inclusion criteria for studies in this review are as follows: (1) studies that include subjects identified as experiencing nonspecific LBP through various means, such as lumbar-pelvic pain; (2) participants of any age and of both male and female genders; (3) randomized controlled trials; (4) various subtypes of LBP based on the ICF model such as back pain with mobility deficit, back pain with referred pain, back pain with radiating pain, and back pain with movement coordination impairments; (5) interventional studies that involve both active and passive hamstring stretching in the experimental group, and the control group implementing regular treatment or placebo, with clear details provided regarding frequency, intensity, and application method; (6) clinician-assisted interventions conducted either in isolation or as part of a multimodal treatment approach; and (7) studies that utilize within- or between-group outcome measures, including pain intensity, hamstring flexibility, and function. Studies were excluded if: (1) the articles were not published in English or Chinese, as we were unable to interpret the findings; or (2) the participants specifically had LBP due to a particular pathology (e.g., infection, tumor, osteoporosis, fracture, structural deformity, or cauda equina syndrome); or (3) the articles were letters, conference papers, case reports, etc.
Information sources and search strategy
One reviewer (Xiang Chen) conducted a comprehensive search in several databases, including Google Scholars, MEDLINE, Embase, PubMed, Cochrane, CNKI, Wanfang, and VIP. The Google Scholars, MEDLINE, Embase, PubMed, and Cochrane were searched using the official websites of the databases via the Google web search engine. On the other hand, the Chinese databases (CNKI, Wanfang, and VIP) were searched through the database section of the library website of Fujian University of Traditional Chinese Medicine. We also searched for unpublished studies, contacting authors for additional data to assess and potentially correct for reporting bias in a meta-analysis. There were no restrictions placed on the sample regarding age, sex, pain duration, or publication date and focused on articles published in English or Chinese languages. The search terms used a combination of MeSH keywords and relevant keywords related to the topic, including “LBP,” as well as terms related to “hamstring stretching” (see Table 1 and Appendix of Search strategy). We also consulted previous systematic reviews published in this field to find any relevant terms not identified by our team. The search was conducted from their inception until August 2023.
Search strategy for database MEDLINE accessed on PubMed. PubMed (including MEDLINE) (1946 to August 2023).

Selection process
A screening process was carried out to determine the eligibility of the articles identified through the search. Upon completion of the search, all citations were imported into EndNote X9 software published by Clarivate Analytics, with duplicates removed. Following a pilot test, two independent reviewers (Yanyun Gou and Huangwei Lei) evaluated the titles and abstracts against the inclusion criteria of the review. Any sources considered potentially relevant were retrieved in full, and their citation details were integrated into EndNote X9 software for centralized management, evaluation, and review of the information.
Study identification and data extraction
To identify potentially eligible studies, the reference lists of included studies, clinical guidelines, registers, websites, and recently published systematic reviews were also searched. Data and results from the selected studies were extracted using a standardized Population, Intervention (Treatment), Comparison, Outcome, and Setting (PICOS) format. PICOS encompasses the characteristics of the studied population, performed treatments, comparative treatments, primary and secondary outcomes, and the data collection setting. Data extraction was carried out by Yanyun Gou and Xiangbin Wang, with cross-verification performed by Xiang Chen utilizing a standardized data extraction template.
Data items
The eligible outcomes were categorized into the following groups:
Pain intensity
Hamstring muscle flexibility
Function
Any assessment of pain intensity, hamstring muscle flexibility, and function was considered eligible for inclusion. Results could be presented as a comprehensive test score reflecting measures of pain intensity, hamstring muscle flexibility, and function. Articles included in the study were required to have measurements at baseline and post-intervention time points, with no limitations on the duration of the intervention period. We anticipated that individual studies would report data for multiple outcomes. Specifically, a single study may report results:
Using multiple methods or tools to measure the same or similar outcome, for example reporting measures of pain intensity using both visual analog scale (VAS) and numeric pain rating scale (NPRS).
Risk of bias
We assessed the risk of bias in the included studies using the Cochrane risk of bias assessment tool. 16 Two review authors (Xiang Chen and Yanyun Gou) independently performed the risk of bias assessment and resolved possible disagreements between review authors by discussion, or arbitration by a third review author (Xiangbin Wang) when consensus could not be reached. The criteria recommended and defined by the Cochrane Back Review Group were scored as “high,” “low,” or “unclear” and were reported in the risk of bias table. A trial with low risk of bias was defined as a trial that met, at a minimum, criteria A (randomization), B (allocation concealment), C5 (outcome assessor blinding), and any three of the other criteria (blinding of outcome assessment, incomplete outcome data and reported selective reporting). 17
Assessment of study quality
The evidence level was evaluated using the NHMRC hierarchy. 18 The methodological quality was assessed using the Physiotherapy Evidence Database (PEDro) scale 19 by Gou and Chen. To ascertain the validity of eligible randomized trials, pairs of reviewers working independently and with adequate reliability determined the adequacy of randomization and concealment of allocation, blinding of patients, therapists blinded, assessors blinded, <15% dropouts, intention-to-treat analysis, between-group comparison, point measures, and variability data. Final scores were calculated based on the last 10 items, resulting in a range of 0–10. The maximum score on the PEDro scale was 10 points (excluding item 1 from the total score). Scores of 9–10 were classified as excellent quality, 6–8 as good quality, 4–5 as fair quality, and scores below 4 as poor quality. 20
Data analysis
The methodological design, number of subjects, comparison groups, intervention protocol, and results for the outcomes of interest were extracted from the selected full-text papers by two independent reviewers (Gou and Wang). The outcome summary measures included the mean and standard deviation (SD) at the end of the intervention. Calculations were conducted using a random effects method. Researchers reached out to the authors of studies with incomplete data via email, in order to acquire results for synthesis or to evaluate study quality. Statistically significant findings were defined as a p-value ⩽ 0.05 and a confidence interval of 95% (95% CI). The prediction interval is utilized to depict the dispersion of effects when the estimate of variance (T2) exceeds zero; conversely, in instances where the estimate of T2 equals zero, the mean and confidence interval are usually documented. The effect size is represented using standardized mean difference (SMD), with SMD values of 0.2, 0.5, and 0.8 indicating small, moderate, and large effects, respectively. All analyses were conducted using Review Manager version 5.3. The study employed sensitivity analysis to evaluate the reliability of findings by investigating the influence of including conference abstract results that have not been fully published and studies with a high risk of bias, while comparing the effects of fixed-effect and random-effects meta-analysis models in the meta-analysis. To assess outcome reporting bias, we generated funnel plots for meta-analyses including at least 10 trials of varying size. If asymmetry in the funnel plot was detected, we planned to review the characteristics of the trials to assess whether the asymmetry was likely due to publication bias or other factors such as methodological or clinical heterogeneity of the trials.
Results
Study identification
The search strategy resulted in 1826 articles, out of which 74 studies were deemed potentially relevant and selected for further analysis. Ultimately, 14 of these studies met the eligibility criteria and were included in the systematic review (n = 735). Figure 1 illustrates the PRISMA flow diagram depicting the inclusion of studies in this review.

PRISMA flow diagram outlining study selection process.
Methodological appraisal
Two independent reviewers conducted a methodological appraisal using the PEDro scale. Disagreements among authors are resolved through consensus or by seeking input from a third author. The PEDro scale ranks from 5 to 9, with an average score of 6.5 out of 10 for all articles that met the criteria for good quality; see Table 2. The analysis of Cochrane’s risk of bias revealed that 71.4% of the studies included demonstrated a random sequence generation, 35.7% reported allocation concealment, 42.9% implemented blinding of participants and personnel, 21.4% applied blinding of outcome assessment, 14.3% had incomplete outcome data, and 7.1% exhibited selective reporting (refer to Figures 2 and 3).
Evidence hierarchy and methodological appraisal.

Item 1: eligibility criteria; Item 2: random allocation; Item 3: concealed allocation; Item 4: similar baseline; Item 5: subjected blinded; Item 6: therapists blinded; Item 7: assessors blinded; Item 8: <15% dropouts; Item 9: intention-to-treat analysis; Item 10: between-group comparison; Item 11: point measures and variability data; 1: described explicitly and in details; 0: unclear, inadequately described.

Risk of bias graph.

Risk of bias summary.
Characteristics of included studies
Fourteen RCTs were included in this study, involving a total of 735 participants, all of whom were diagnosed with non-specific low back pain (NSLBP). Among these studies, eight were categorized as uncertain type, four as back pain with radiating pain, and two as back pain with movement coordination impairments, all following the ICF model. Specifically, four studies compared hamstring stretching to common physiotherapy, three studies compared it to soft tissue release techniques, three studies compared it to nerve mobilization methods, two studies compared it to other muscle stretching exercises, one study compared it to instrument-assisted techniques, and one study did not specify the control group’s treatment. The sample sizes of these 14 studies ranged from 22 to 66 participants, and the participants had subacute to chronic NSLBP and were aged between 18 and 60 years. Regarding intervention duration, three studies reported a 4-week intervention, two studies reported a 6-week intervention, two studies reported a 3-week intervention, one study reported a 6-month intervention, and one study reported a 5-day intervention, while the remaining three studies did not mention the duration and instead used the term “sessions.” In terms of outcome measures, 12 studies used the VAS 21 or NPRS 21 to assess back pain intensity, eight studies used the Oswestry Disability Index (ODI) 22 to evaluate functional limitations, and six studies used straight leg raise (SLR) 23 to measure hamstring muscle flexibility. See Table 3.
Characteristics of included studies with PICOS format and conclusion.

EG: experiment group; CG: control group; NR: not reported; mos: months, VAS: visual analog scale, ODI: Oswestry disability index, SLR: straight leg raise test, SRT: sit and reach test, AKE: active knee extension, NPRS: numeric pain rating scale.
Table 3 summarizes the characteristics of these studies.
Effects of interventions
Primary outcome: Pain intensity
Twelve trials24 –35 with a total of 432 participants evaluated the impact of hamstring stretching on pain intensity using a VAS and NPRS. Hamstring stretching resulted in lower pain scores compared to regular treatment in different categories of LBP (SMD = −0.72, 95% CI: −1.35 to −0.09; I2 = 89%, p = 0.03). However, in cases involving subgroup analysis of back pain with uncertain type, radiating pain, or movement coordination impairments of LBP, hamstring stretching showed no significant difference when compared to regular treatment. Refer to Figure 4.

Analysis of ICF category on pain intensity
Secondary outcome: Hamstring muscle flexibility
Six trials24,32 –34,36,37 involving a total of 225 participants evaluated the impact of hamstring stretching on hamstring muscle flexibility. Subgroup analysis showed that hamstring stretching resulted in a greater range of motion for hamstring muscle flexibility compared to regular treatment specifically for cases of back pain with radiating pain (SMD = 2.39, 95% CI: 1.76–3.02; I2 = 0%, p < 0.001). However, with regard to overall effectiveness, there is no significant difference in improving hamstring flexibility between hamstring stretching and regular treatment (SMD = 0.93, 95% CI: −0.03 to 1.90; I2 = 91%, p = 0.06). Refer to Figure 5.

Analysis of ICF category on Hamstring muscle flexibility.
Secondary outcome: Function
Oswestry Disability Index
Seven trials 24,25,27,29,31,32,35 (n = 276) evaluated the effects of hamstring stretching on function using the ODI. Hamstring stretching was found to lead to decreased ODI scores in comparison to regular treatment, particularly in individuals suffering from LBP across all subtypes (MD = −6.97, 95% CI: −13.34 to −0.60; I2 = 95%, p = 0.03). Refer to Figure 6.
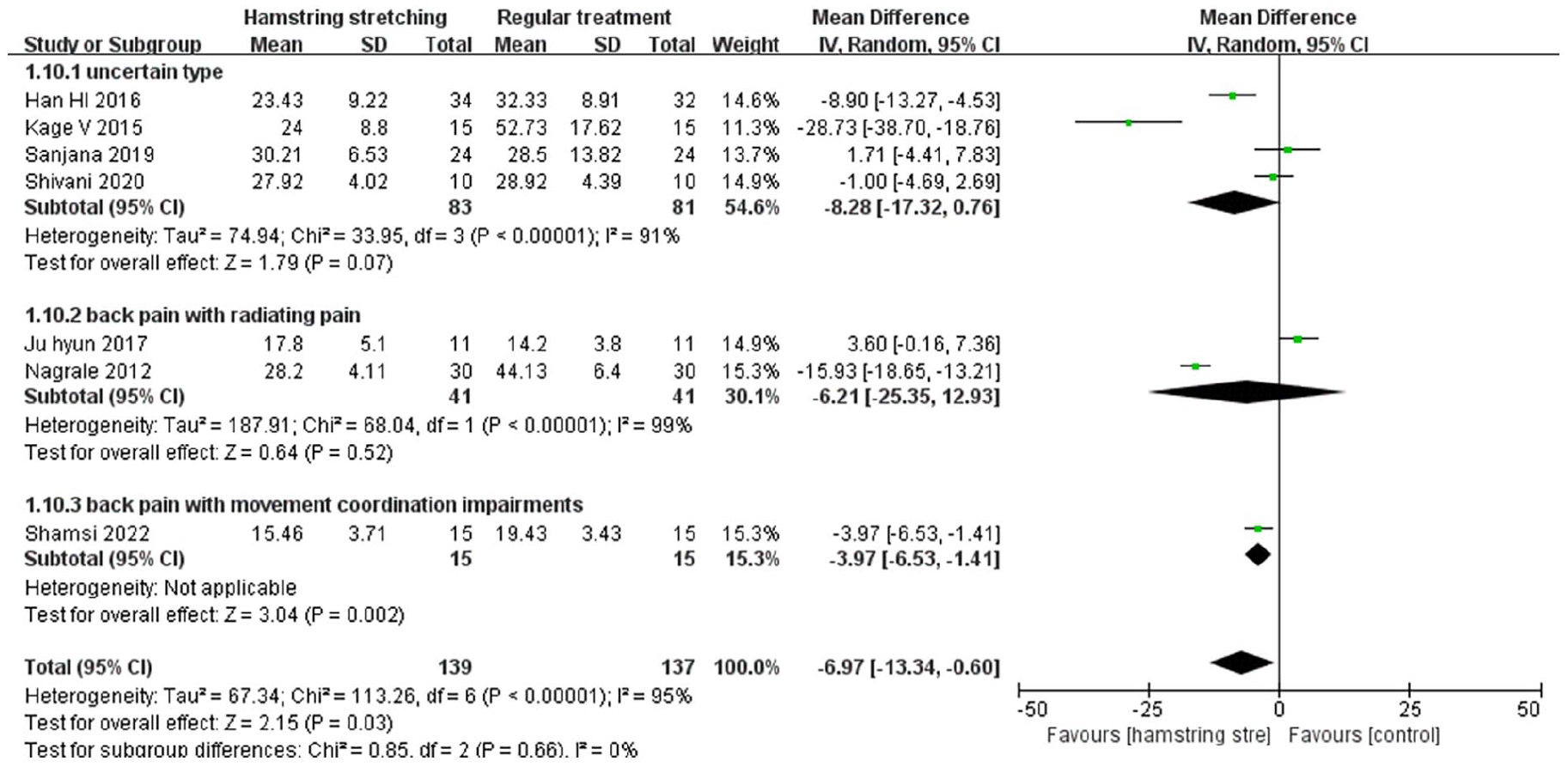
Analysis of ICF category on ODI.
Reporting biases
Funnel plots were employed to assess publication bias within the included studies, specifically concentrating on the primary outcome parameter of pain intensity. The symmetrical distribution displayed on the funnel plot suggests equilibrium on both sides, thereby suggesting an absence of publication bias (see Figure 7).

Funnel plot of pain intensity.
Discussion
This study represents the inaugural systematic review incorporating meta-analyses of interventions that specifically target the lower limb muscles, providing evidence of their clinical impact across various categories of LBP as classified by the ICF model.
Our study identified that hamstring stretching is effective in reducing pain intensity in individuals with various categories of LBP, in comparison to regular treatments. The concept of hip-spine syndrome was introduced by Offierski and MacNab 30 years ago. 38 This model posits that there exists evident impairment in two regions—the hip joint and the lower back. The model postulates that addressing the condition in one area can alleviate pain and enhance functionality in the untreated area. Despite having distinct function, the hip joint and lower back collaborate in a coordinated movement known as LPR, often involving flexion. 39 The tight hamstring alters the LPR, as can change the spine and hip’s range of motion and timing, which increases the bending stresses of the lumbar intervertebral discs and load on the lumbar spine pain,40,41 prolonged mechanical stress or repetitive stress by flexion of the trunk by deforming the viscoelastic tissues of the lower back and contributes to back pain, 42 previous study 43 states that alteration in the viscoelastic properties tends to increase the risk of LBP. The flexibility of hamstring muscles may help to maintain “normal” lumbar pelvic coordination and reduce pain intensity. Moreover, decreasing tightness in the hamstrings, which connect the lumbar region to the back of the thigh, can relieve tension in the lower back and ameliorate symptoms. 44 Numerous studies have corroborated these findings.45 –47 However, the subgroup analysis conducted based on the ICF classification of LBP did not yield significant findings. This could be attributed to the limited number of articles included under each specific classification, which hindered the derivation of meaningful results. It can be concluded that hamstring stretching exercises may provide relief for various types of LBP. However, further clinical trials are warranted in the future to ascertain its pain production efficacy for specific classifications.
The results of the meta-analysis indicate that hamstring stretching is effective in enhancing the ODI among patients with LBP of various types. Ferreira et al. 48 and LaRoche et al. 49 agreed that increased hamstring flexibility resulting from long-term stretching training enhances muscle performance and, consequently, improves functional capacity. Our findings are further supported by the study conducted by Baharam et al., 41 which demonstrated that hamstring stretching for LBP enables the appropriate muscles to function optimally, eliminating the need for compensatory muscle activation. Simultaneously, it reduces disability in performing daily activities and improves the overall quality of life. However, we observed conflicting effects of stretching on function in back pain with radiating pain, as evidenced by one included study. 27 Sensitivity analysis demonstrated the instability of this outcome, possibly due to variations in the severity of the participants and differences in intervention methods. Back pain with radiating pain patients often experienced increased irritability, and forceful hamstring stretching during intervention might exacerbate their symptoms, leading to functional impairment. Hence, we recommend reducing the intensity of hamstring stretching exercises for back pain with radiating pain patients and closely monitoring any changes in symptomatology.
Subgroup analysis revealed a significant difference in the SLR test between hamstring stretching and regular treatment for individuals experiencing back pain with radiating symptoms. As for stretching, Kuukkanen and Mälkiä 50 suggest that one of its main therapeutic goals is to promote the normal flexibility of muscles and connective tissues of the spine. The SLR test serves not only to assess hamstring muscle flexibility but also to evaluate sciatic compromise resulting from irritation of the lumbosacral nerve root. 23 Patients experiencing back pain with radiating symptoms consistently reported a positive SLR test, which may be due to nerve irritation or hamstring tightness. 51 Hamstring stretching exercises for LBP can improve muscle tightness and mobilize the sciatic nerve. Thus, hamstring stretching exercises, such as slump stretching, 3 have a significant effect on SLR in patients with back pain and radiating symptoms. However, stretching does not significantly improve hamstring muscle flexibility in patients with back pain with mobility deficit. This lack of improvement may stem from the compensatory excessive hip flexion observed in these patients during activities like bending forward, which is a result of restricted lumbar flexion caused by stiffness in the lumbar spine. Over time, this prolonged compensation can lead to overstretching of the hamstrings. As a result, stretching is ineffective in improving hamstring flexibility for those due to their pre-existing excessive flexibility.
Patients with LBP suffered weakened core muscle endurance tend to have excessive shortening of the hamstrings. 52 In clinical practice, we have observed that many individuals with radicular pain also concurrently experience coordination impairments. Future clinical interventions for patients with LBP accompanied by radicular pain or coordination impairments should prioritize the enhancement of hamstring flexibility and the strengthening of core musculature to promote spinal stability.
These findings underscore the significance of incorporating hamstring stretching into the treatment plan for individuals with LBP to alleviate pain intensity and enhance functional capacity. Our study revealed that hamstring stretching exercises can effectively alleviate pain intensity in various types of back pain. Back pain patients with radiating pain experienced a more significant improvement in SLR when engaging in hamstring stretching. Furthermore, hamstring stretching has demonstrated effectiveness in enhancing the ODI for patients with diverse types of back pain.
However, due to the limited number of included studies, we cannot confirm the relationship between hamstring stretching and the different types of LBP. Considering the ICF classification of LBP in clinical studies would provide more accurate assessment and treatment for future clinical practice.
Limitation
The main area of concern is inconsistency. In terms of inconsistency, a variety of methods involving clinician assistance were reported in the studies, such as hamstring stretching, hamstring stretching using proprioceptive neuromuscular facilitation (PNF) techniques, and clinician-performed slump stretching. In addition to variations in techniques, there were also inconsistencies regarding when the outcome measures were taken. Finally, in terms of inconsistency, there was also considerable variation in the duration of treatment, resulting in variations in the overall duration of treatment.
However, the inclusion of only 14 studies and moderate methodological quality reduces the reliability of the results. The number of study subgroups is rather small, which impacts the interpretation and conclusions of this study. Other limitations of this meta-analysis were the differences between studies regarding protocols, timing, types, and duration of stretching exercises, making it challenging to compare the literature-based stretching parameters. The elevated I2 value observed in the outcome measures suggests a substantial degree of heterogeneity, which may be attributed to the utilization of diverse indicators, including VAS and NPRS, for assessing pain intensity, as well as SLR and AKE for evaluating hamstring muscle flexibility.
To bridge this gap, there is a need for future systematic reviews and studies aimed at analyzing various stretching techniques, such as PNF stretch, static stretch, dynamic stretch, and ballistic stretch. Additionally, it is important to compare different stretching parameters in order to identify the most effective approach to alleviating pain intensity and enhancing the functional capabilities of LBP patients, while considering the ICF model. Future research should also investigating the effects of combining hamstring stretching with different training approaches on distinct types of LBP using the ICF model.
Conclusion
This meta-analysis demonstrates the effectiveness of hamstring stretching exercises in reducing pain intensity across different categories of LBP and improving SLR in patients with back pain and radiating pain. It also highlights the improvement in functional ability for patients across all types of back pain. However, the presence of methodological heterogeneity among the included studies rendered it unfeasible to ascertain the optimal parameters for stretching exercises, stretching type, and the benefits for various categories of LBP utilizing the ICF model.
Supplemental Material
sj-doc-1-smo-10.1177_20503121241252251 – Supplemental material for The effects of hamstring stretching exercises on pain intensity and function in low back pain patients: A systematic review with meta-analysis of randomized controlled trials
Supplemental material, sj-doc-1-smo-10.1177_20503121241252251 for The effects of hamstring stretching exercises on pain intensity and function in low back pain patients: A systematic review with meta-analysis of randomized controlled trials by Yanyun Gou, Huangwei Lei, Xiang Chen and Xiangbin Wang in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121241252251 – Supplemental material for The effects of hamstring stretching exercises on pain intensity and function in low back pain patients: A systematic review with meta-analysis of randomized controlled trials
Supplemental material, sj-docx-3-smo-10.1177_20503121241252251 for The effects of hamstring stretching exercises on pain intensity and function in low back pain patients: A systematic review with meta-analysis of randomized controlled trials by Yanyun Gou, Huangwei Lei, Xiang Chen and Xiangbin Wang in SAGE Open Medicine
Supplemental Material
sj-docx-4-smo-10.1177_20503121241252251 – Supplemental material for The effects of hamstring stretching exercises on pain intensity and function in low back pain patients: A systematic review with meta-analysis of randomized controlled trials
Supplemental material, sj-docx-4-smo-10.1177_20503121241252251 for The effects of hamstring stretching exercises on pain intensity and function in low back pain patients: A systematic review with meta-analysis of randomized controlled trials by Yanyun Gou, Huangwei Lei, Xiang Chen and Xiangbin Wang in SAGE Open Medicine
Supplemental Material
sj-xlsx-2-smo-10.1177_20503121241252251 – Supplemental material for The effects of hamstring stretching exercises on pain intensity and function in low back pain patients: A systematic review with meta-analysis of randomized controlled trials
Supplemental material, sj-xlsx-2-smo-10.1177_20503121241252251 for The effects of hamstring stretching exercises on pain intensity and function in low back pain patients: A systematic review with meta-analysis of randomized controlled trials by Yanyun Gou, Huangwei Lei, Xiang Chen and Xiangbin Wang in SAGE Open Medicine
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
Data curation: Huangwei Lei, Xiang Chen. Formal analysis: Yanyun Gou, Xiangbin Wang. Funding acquisition: Yanyun Gou. Investigation: Xiangbin Wang. Methodology: Huangwei Lei. Project administration: Yanyun Gou. Visualization: Huangwei Lei, Yanyun Gou. Writing—original draft: Yanyun Gou. Writing—review and editing: Yanyun Gou and Xiangbin Wang.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Project supported by the National Natural Science Foundation of China (Grant No. 82205306).
Ethics approval and consent to participate
Not applicable.
Informed consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.