
Abstract
Objective:
To report a case of a 12-year-old boy with intellectual disability and attention deficit hyperactivity disorder, who came to surgery for an examination due to a minor bulge on the left thumb, which had been growing for the previous month. His mother denied any trauma.
Methods:
After the removal of the clinically ambiguous bulge and a pathohistological confirmation that it was a periungual fibroma, complete patient analysis was performed due to the presence of hypomelanotic macules and a suspected tuberous sclerosis.
Results:
Considering the presence of hypomelanotic macules, as one of the main criteria, possible TS diagnosis was set.
Conclusion:
Early detection of the symptoms of TS enables a timely provision of protocols for further patient monitoring, which affects the patient’s morbidity and mortality.
Keywords
Introduction
Tuberous sclerosis (TS) or tuberous sclerosis complex (TSC) is a rare multi-system genetic disease which can be inherited from an affected parent or occur as a result of a new gene mutation. The usual incidence is 1 in 6000 newborn children. 1 The genes responsible for the development of TSC are TSC1 and TSC2. 2 Only 10%–25% of patients do not show pathogenic mutations of TSC1 and TSC2 genes during genetic analysis. While positive results have very high predictive value for family members, normal results do not exclude the diagnosis of TSC. 3 The disease is a consequence of the growth of benign tumors, hamartomas, in many organs. Changes most frequently occur in the brain, and they also affect other organs, such as the heart, kidneys, eyes, lungs and skin.
The symptoms can be classified into two groups: major and minor features. Major features are as follows: three or more facial angiofibromas or fibrous plaque; two or more ungual fibromas; three or more hypomelanotic macules—minimum 5 mm in diameter, shagreen patches, multiple retinal nodular hamartomas, cortical dysplasia, subependymal nodules (SENs), subependymal giant-call astrocytomas (SEGAs), cardiac rhabdomyomas and lymphangioleiomyomatosis (LAMs); and two or more angiomyolipomas. The minor features includes changes in tooth enamel, two or more intraoral fibromas, retinal achromic patch, “confetti” skin lesions, multiple renal cysts and non-renal hamartomas. Either two major criteria or one major criterion with two or more minor criteria is necessary for the definite diagnosis of TSC. Either one major criterion or two or more minor criteria are required for a possible diagnosis. 3
Case report
A boy aged 12 years, with notable developmental disorder, intellectual disability (ID) and attention deficit hyperactivity disorder (ADHD), was referred to surgery by a dermatologist due to a bulge of unknown etiology in the nail base area of the left thumb, which had appeared a month earlier. During the visit, the mother denied any trauma and stated that the bulge was growing. The boy was born as a child at neurological risk. First signs of ID occurred during childhood. The results of cognitive development assessment showed a major delay in the development of gross and fine motor skills, speech and socialization. Pronounced hyperactivity led to the diagnosis of ADHD. A month before visiting our clinic, the mother noticed skin lesions formed in the form of minor, light skin areas on the chest, which were expanding to the torso and upper arms (Figure 1).

Hypomelanic macules (“ash leaf spots”) as white or lighter patches of skin on the (a) back and (b) forearm.
Dermatological examination confirmed hypomelanotic macules. Additionally, a formation of unknown etiology in the left thumb nail base was detected, which was the reason for referral to a surgeon. Clinically, the formation seemed like a soft bulge with a large basis (Figure 2).
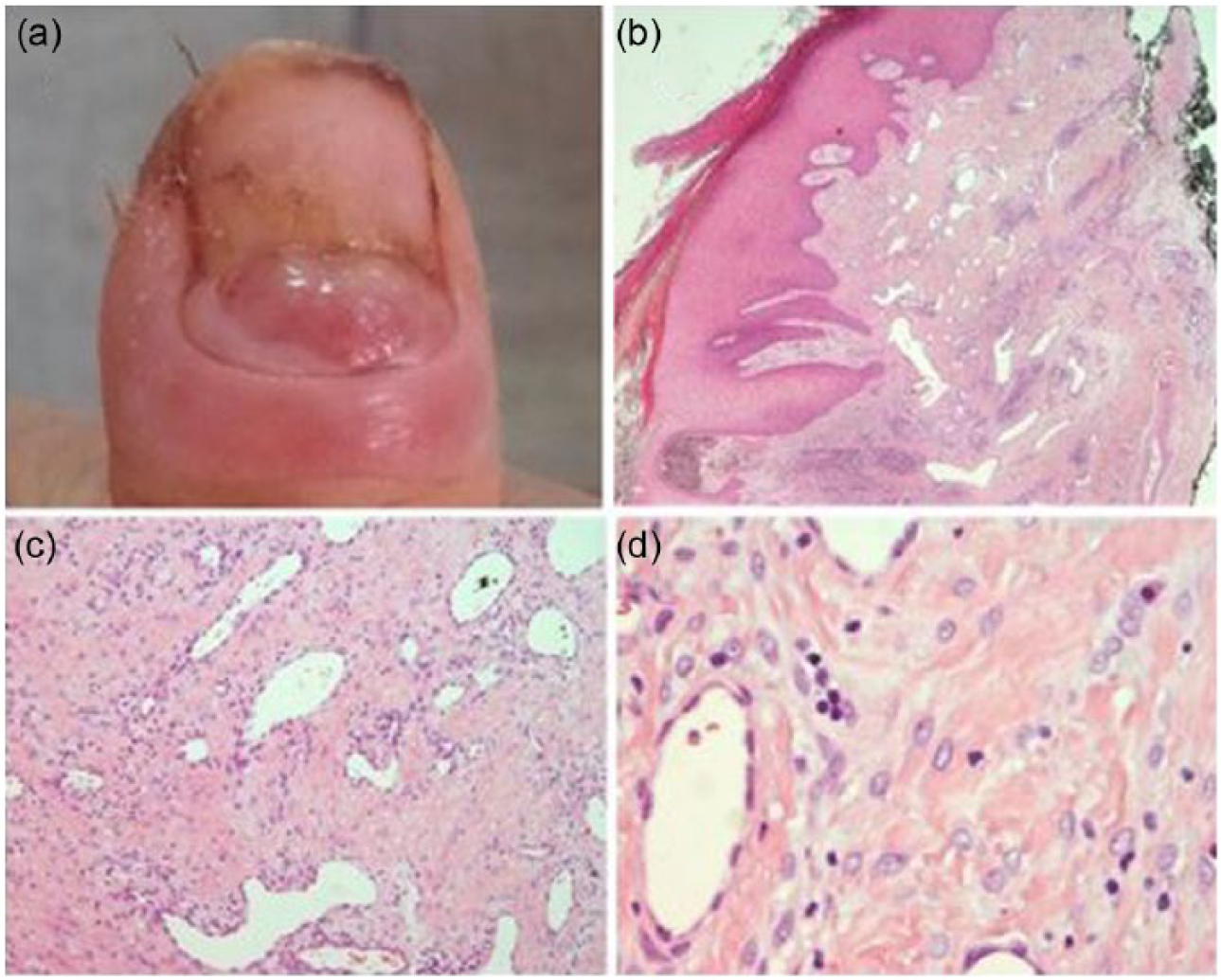
(a) Ungual fibromas on the thumb, (b) histological examination shows epidermal acanthosis and hyperkeratosis with expanded dermis, (c) a large number of dermal capillaries and (d) spindled cells embedded in haphazardly arranged collagen bundles in the dermis with no mitotic figures were seen.
We performed longitudinal incision on each side of the formation in the area of proximal nail fold and raised it, which enabled us to excide the entire formation. Pathohistological analysis suggested the diagnosis of periungual fibroma (Figure 2), which was followed by the complete patient analysis due to suspected TS. Magnetic resonance imaging (MRI) of the brain showed normal morphological results. Cardiac, pulmonary, ophthalmologic and dental examinations were normal, and so were the abdomen and kidney ultrasound examinations. TSC2 gene analysis showed no mutations. Considering the presence of hypomelanotic macules, as one of the main criteria, possible TS diagnosis was set.
Discussion
TSC is characterized by a broad range of symptoms, differing in intensity and age of occurrence. Some of the symptoms can be registered already in the prenatal period, such as cortical dysplasia. Some of them appear for the first time in early childhood, but their occurrence extends into adulthood, which is typical for hypomelanotic macules and shagreen patches. Adolescence is a period when ungual fibromas 4 most frequently occur for the first time. Hypomelanotic macules are one of the earliest and most frequent symptoms in children with TSC. 5 Unlike hypomelanotic macules, ungual fibromas, known as Koenen’s tumors, are observed in 20% of patients. 3 They appear as firm, smooth, skin-colored or reddish papules around fingernails and toenails. They are usually asymptomatic, with typical clinical features; so, a diagnosis is possible only on the basis of a physical examination by a dermatologist, although sometimes they can be painful or clinically ambiguous which requires surgical excision and pathohistological diagnostics. 6 The banner flap procedure, 7 which was applied in our patient, certainly leaves the minimum possibility for potential complications.
TSC is connected with a range of cognitive, developmental and mental disorders. TSC-associated neuropsychiatric disorders (TAND) is a new terminology used to describe the interrelated functional and clinical manifestations of brain dysfunction in TSC, including aggressive behaviors, autism spectrum disorders, intellectual disabilities, psychiatric disorders, neuropsychological deficits, and school and occupational difficulties. 8
The detection rate of mutations in TSC1 and TSC2 genes is approximately 80%. In our case, we opted for a TSC2 gene analysis since the reports published to date suggest that among the patients with the confirmed gene mutation, the mutation is present in the TSC1 gene only in 21% of cases and in the TSC2 gene in as much as 79% of cases. 9 With our patient, clinically suspected TSC could be neither confirmed nor excluded on the basis of the molecular TSC2 gene analysis.
By diagnosing possible TSC, our patient’s profile acquired a new dimension, considering the well-known fact that TSC symptoms occur in all life periods, which changes the previous manner of monitoring the patient due to ADHD and ID and includes the accepted algorithm of examinations which, in the case of TSC, recommends patient follow-up at least once a year, with regular electroencephalogram (EEG) monitoring, computed tomography (CT) or MRI of brain within a period of 1–3 years, including a thorough examination due to a possible occurrence of other systemic manifestations of TSC.
The aim of this report is to emphasize the importance of early detection of the symptoms of TS. This enables a timely provision of protocols for further patient monitoring, which affects the patient’s morbidity and mortality.
Footnotes
Acknowledgements
N.G. treated the patient, conceived and designed the case report, coordinated the evaluation of the case, drafted the manuscript and approved the final manuscript as submitted; I.L.-B. as psychiatrist involved in the treatment of the patient, participated in the draft of the manuscript and approved the final manuscript as submitted; B.G. as a molecular biologist isolated the DNA of patients for gene analysis, participated in the draft of the manuscript and approved the final manuscript as submitted; L.T. reviewed and edited the manuscript and approved the final manuscript as submitted; A.S. as neurologist treated the patient and approved the final manuscript as submitted; and N.J. supervised and gave expert opinion on the case, revised the manuscript and approved the final manuscript as submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.