
Abstract
Tuberous sclerosis is an uncommon neurocutaneous syndrome characterized by hamartomatous growths with unpredictable progression. Diagnosing and managing neonatal tuberous sclerosis can be challenging. We report a rare case of a 30-day-old male born out of a non-consanguineous marriage who presented with poor suckling and persistent abnormal body movement, required prolonged intensive care, and was diagnosed with tuberous sclerosis with multisystem involvement.
Introduction
Tuberous sclerosis, also called tuberous sclerosis complex (TSC), is an uncommon, multisystem genetic disease that causes benign tumors in the brain and other vital organs. The central nervous system involvement can produce seizures, impaired intellectual development, autism, and behavioral problems. 1 The reported incidence varies between 1/6,000 and 1/10,000 without sex predilection.2,3 Disease severity is tremendously variable in TSC. 4 Although the mean age at diagnosis is around 1 year, TSC is increasingly identified early due to detecting cardiac rhabdomyoma in antenatal ultrasound. 5 We report an infant with multiple cardiac rhabdomyoma and subependymal nodules who presented with refractory seizures.
Case report
A 30-day-old male born out of a non-consanguineous marriage presented with poor suckling and persistent abnormal body movement for 1 day. The seizure was focal and recurrent, lasting from a few seconds to a minute. He was the firstborn child to 28-year-old primigravida at 37 weeks of gestation via emergency lower segment cesarean section for antepartum hemorrhage. The child had a low APGAR (Appearance, Pulse, Grimace, Activity, and Respiration) score (4/10 and 4/10 at l and 5 min, respectively), developed cyanosis for which active resuscitation was done, and was eventually admitted to a neonatal intensive care unit (NICU). The child required active resuscitation and developed respiratory distress soon after birth, requiring NICU care for 21 days. Eight days after discharge, he presented with the aforementioned complaints. Family history was significant for recurrent seizures in the father, currently controlled with medication, without other identified abnormalities. Other family members followed up to three generations did not have identifiable symptoms. The patient’s father was evaluated for tuberous sclerosis but did not meet the diagnostic criteria. Antenatal scans were insignificant.
The neonate had a good tone and cry with stable vitals. The anterior fontanelle was level with the scalp, along with open sutures. Anthropometric parameters, including length (53 cm), occipitofrontal circumference (34 cm), and weight (3.5 kg), were between the 85th and 97th percentile according to the WHO growth chart. Age-appropriate neonatal reflexes were present. The ophthalmological evaluation was normal.
Complete blood count, liver function test, and renal function test were all within the reference range except for a hemoglobin of 7.4 g/dl and random blood sugar of 35 mg/dl. The cause for anemia and hypoglycemia could not be identified. Arterial blood gas analysis and cerebrospinal fluid (CSF) analysis were normal. Echocardiography (ECHO) was performed as a part of the evaluation of early neonatal respiratory distress and showed multiple echogenic masses in the left ventricular free wall, interventricular septum, and right ventricular posterior wall, the largest mass (2 × 1 cm) over the interventricular septum without right and left ventricular outflow tract obstruction, giving the impression of multiple rhabdomyoma (Figure 1). An electroencephalogram (EEG) showed epileptic discharge over the right centrotemporal region. Neurosonography showed mild dilatation of cisterna magna. Brain magnetic resonance imaging (MRI) showed high-signal-intensity subependymal nodules along the right lateral ventricle, focal cortical dysplasia in the left frontal lobe, and radial migratory bands (Figure 2). Ultrasonography (USG) of the abdomen and pelvis showed mild hydronephrosis of the left kidney, minimal ascites, and mild hepatomegaly. After MRI reports became available, the baby was examined keenly for any cutaneous markers again, and four hypopigmented macules were visualized over the abdomen that had been overlooked earlier (Figure 3).

Echocardiography showing multiple echogenic masses in the left ventricular free wall, interventricular septum, and right ventricular posterior wall (arrows).

Plain brain magnetic resonance imaging, showing high signal intensity subependymal nodules along the right lateral ventricle (arrow), focal cortical dysplasia in the left frontal lobe, and radial migratory bands.

Hypopigmented macules (arrows) over the abdomen.
A diagnosis of TSC was made. Despite vigabatrin being the drug of choice due to its nonavailability, other antiepileptics had to be used. As per the clinician's experience, the patient was initially managed with dextrose, normal saline, and levetiracetam injection. The patient had an intractable seizure needing frequent adjustment of antiepileptic drugs and was maintained on levetiracetam, phenobarbitone, phenytoin, and pyridoxine. The neonate was discharged after 4 days without seizures. The neurological examination of the patient was within normal limits.
At the time of completion of this manuscript, the patient was 9 months old. Despite adherence, he continued to have seizures. His gross motor milestones are delayed, although he is growing well (11 kg) and has achieved other developmental domains appropriate for his age.
Discussion
We report a TSC case diagnosed during the neonatal period. When the initial neonatal examination was performed, the skin stigmata were overlooked, but after the newborn developed seizures, further workup found subependymal nodules and cardiac rhabdomyoma that led to the diagnosis. As autosomal dominant multisystemic phakomatoses, TSC results from overactivation of the mammalian target of the rapamycin (mTOR) pathway due to mutation in either the TSC1 or TSC2 gene and affects multiple organs and systems such as brain (cortical tubers, subependymal nodules, and subependymal giant cell astrocytoma), heart (cardiac rhabdomyoma), kidneys (renal angiomyolipoma), lungs (lymphangioleiomyomatosis), and skin (shagreen patches, hypomelanotic macule, and angiofibroma). 6 Although the patient’s father had a history of seizures, TSC was not proven. Diagnosis relies on updated international TSC diagnostic criteria, as shown in Table 1.
International tuberous sclerosis complex diagnostic criteria.
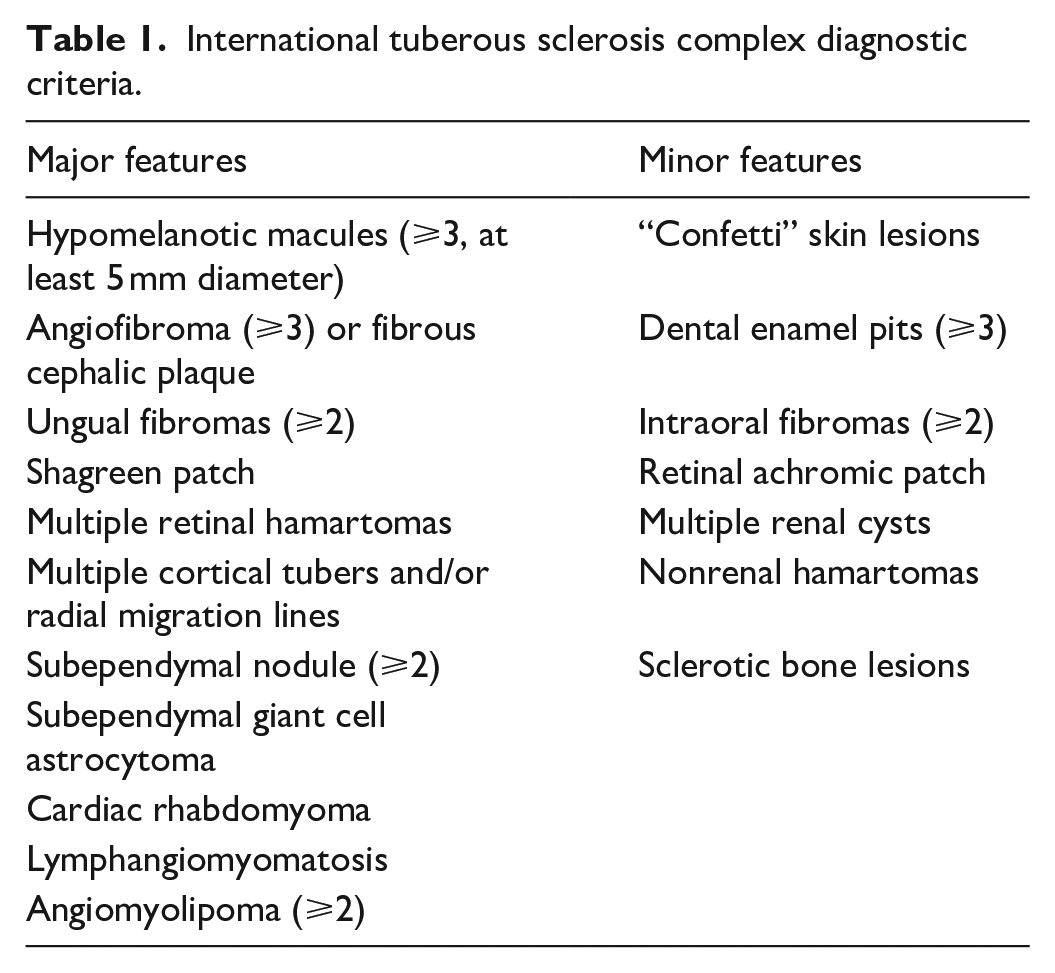
Definite TSC: Either two major features or one major feature and two minor features. Possible TSC: Either one major or ⩾ two minor features. 2 Our patient met three major criteria (subependymal nodules in MRI, multiple cardiac rhabdomyoma, and hypomelanotic macules), which suggests definite TSC.
Nelson et al. conducted a prospective longitudinal study in 130 patients where hypomelanotic macules, cardiac rhabdomyoma, and subependymal nodules were the most encountered pathologies. The appropriate diagnosis of TSC is made either clinically or genetically. In our case, due to a lack of genetic diagnostic facilities, the diagnosis was based on clinical criteria. Although identifying TSC 1 or TSC 2 mutation is sufficient for diagnosing TSC, 15% of the patients may not have identifiable mutation by conventional testing.7,8
Our patient was diagnosed with TSC at the age of 30 days; the mean age for early postnatal diagnosis observed in many cases was 72 days. 9 Antenatal diagnosis is increasingly made with fetal USG and MRI. 10 We followed the World Health Organization antenatal care (ANC) visits protocol and did not identify rhabdomyoma antenatally on routine anomaly scan, although cardiac rhabdomyoma has been identified as early as 20 weeks. 9
The symptoms are diverse due to high variability in the number of organs affected, the severity of the tumors within an organ, and the time of presentation. 10 Hence, no single symptom is present in every patient, and none of them is completely pathognomonic, making a diagnosis of TSC challenging. 11 Similarly, in our case, TSC being uncommon in our setup, four hypopigmented macules present over the abdomen were overlooked. Although TSC was not considered initially, our patient presented with respiratory distress, similar to a report by Isaac et al., 12 where respiratory distress, arrhythmia, and cyanosis were the common postnatal findings. The neurological manifestations include seizures, autism, and cognitive behavioral disorders, seizure being the most common presenting complaint, mostly beginning within the first month of life.9,10 The EEG may show ictal abnormality recordings much before the clinical seizures.9,10 Early-onset seizures and EEG abnormalities increase the likelihood of developing autism in the future. 10 The hypopigmented macules identified later in our case are common manifestations; other cutaneous findings, such as shagreen patches and fibromas, generally tend to occur later. 10 Our patient did not show any renal angiomyolipoma; it is usually detected after 3 years of age. 10 Rhabdomyoma is the most common cardiac anomaly detected antenatally, resulting in symptoms such as outflow tract obstruction, impaired valvular function, and arrhythmias. 10
TSC is caused by activation of the mTOR signaling pathway, leading to hamartomatous lesions caused by a mutation in TSC genes. The discovery of the relationship between TSC1/TSC2 and mTOR has resulted in using mammalian target of rapamycin inhibitors (mTORi), particularly sirolimus and its analog everolimus. Hence, mTORi is a potential treatment based on the pathogenesis of the disease. 13 About 63%–78% of cases of TSC suffer from epileptic spasms and focal seizures. For infantile spasms, vigabatrin is recommended; otherwise, antiseizure medications are used according to the type of seizure. Additional treatment options include everolimus, adrenocorticotrophic hormone, or prednisolone. For refractory cases, epilepsy surgery and CSF diversion can be considered. The EPISTOP (Epileptogenesis in a genetic model of epilepsy- Tuberous sclerosis complex) study concluded that preventative Vigabatrin treatment reduced the risk of infantile spasm, seizure, and drug-resistant epilepsy. 14 Our patient continues to have seizures despite under-dose-adjusted antiepileptics (levetiracetam, phenobarbitone, and phenytoin). Newer treatment modalities were not used due to unavailability and financial implications.
Counseling regarding compliance with the medication and regular periodic follow-ups is important to look for progression or regression of the pathologies and to watch for any new organ involvement (Table 2). 15 Despite diagnosis, treatment, and regular follow-up, there is a high rate of neurological and neuropsychiatric morbidity, and the presence of early-onset refractory epilepsy may lead to impaired cognitive development. 16
Surveillance and management recommendations for patients already diagnosed with definite or possible tuberous sclerosis complex (TSC).

Conclusion
TSC is an uncommon neurocutaneous syndrome that can be diagnosed during the neonatal period. Thorough evaluation of infants with unexplained seizures is important to ensure that the diagnosis of TSC might not get overlooked as in our case. Vigilance for cutaneous markers may help avoid costly and not-so-readily-available diagnostic modalities, narrowing our diagnosis toward neurocutaneous syndromes such as TSC. Nonavailability of newer treatment modalities and their cost may limit the proper management of patients in low-resource countries.
Footnotes
Acknowledgements
We, the authors, thank the patient party for their support in publishing this paper.
Authors contributions
S.K., P.B., A.P., K.K., D.R., K.A.H., and S.G. drafted, reviewed the literature, and edited the manuscript. AKS was in charge of the case and reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases.
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.