
Abstract
Management of patients with central nervous system tumors relies largely on magnetic resonance imaging scans to document disease progression or recurrence. The finding of new lesions always presents the challenge of differentiating between post-surgical changes, radiation necrosis, gliosis, and tumor, submitting these patients to more aggressive therapy and more toxicity. We reviewed the medical records of three patients with primary central nervous system tumors treated at the Children’s Hospital Los Angeles who had new false-positive magnetic resonance imaging findings suggestive of tumor recurrence. All of them had complete total resection of primary tumor, had received involved-field radiation therapy, had biopsies confirming absence of viable tumor, and all three patients are long-term survivors. These cases exemplify that not everything that enhances on brain or spine magnetic resonance imaging is viable tumor, and a biopsy should always be considered in the decision-making process in evaluation of potentially recurrent central nervous system tumors in pediatric patients. A step-wise approach for such challenging cases is presented in this article.
Introduction
The management of patients with central nervous system (CNS) tumors largely relies on magnetic resonance imaging (MRI) for diagnosis, surgical planning, and evaluation of response, progression, or recurrence. 1 Images obtained at diagnosis and immediate post-operative period guide further therapy, establish prognosis, and define follow-up. At diagnosis, scans of the brain and spine document the primary tumoral lesion(s) and dissemination, and allow surgical and radiotherapy planning. Routine scans repeated within 96 h after surgery document degree of resection,2–4 which directly correlates to prognosis and dictates intensity of therapy. The follow-up consists of MRI imaging every 3–6 months, depending on diagnosis, symptoms, and use of adjuvant therapy.5,6 The finding of new enhancing lesions presents the challenge of differentiating between benign lesions (such as abnormalities secondary to therapy, late post-surgical changes, radiation necrosis, or gliosis) and recurrent tumor.7,8 Assumption that any new lesions are tumor will lead to more aggressive therapy, causing more toxicity and sequelae.2–4,8
The Children’s Hospital Los Angeles (CHLA) is a free-standing pediatric hospital with one of the largest treatments and research programs in North America, currently receiving about 120 new patients with CNS tumors/year, of whom about 70% are treated accordingly to standard Children’s Oncology Group (COG) protocols. We report on three patients with completely resected CNS tumors who presented with new lesions on follow-up MRI scans suspicious for recurrent tumor, with no evidence of malignancy on biopsy.
Cases
All patients were treated at CHLA and identified by retrospective review of pathology database from 2000 to 2011 of cases with negative histological findings for tumor recurrence after gross total resection (GTR). Exclusion criteria were partial resection of primary tumor, unavailable MRI scans, unquestionable disease progression on serial MRI scans before biopsy, and parental refusal to informed consent. Patients and parents signed informed consent approved by the CHLA Institutional Review Board. Five patients were identified, but one was lost to follow-up, and one refused to sign the consent.
Patient 1 (Figure 1(a)–(c)) is a Hispanic female diagnosed at the age of 15 years with myxopapillary ependymoma of the spinal cord with 5.5 cm mass in the spinal canal L2–L4 and an isolated enhancing nodule at S2. After partial resection of the primary tumor, she received 54Gy intensity-modulated radiation therapy (IMRT) to the tumor bed. After completing irradiation for 2 months, local recurrence was documented (Figure 1(b)), and GTR of the tumor confirmed by post-operative MRI was followed by chemotherapy with weekly carboplatin 175 mg/m2, 4 weeks on, 2 weeks off, planned for seven cycles. While receiving chemotherapy, after the fifth cycle, a follow-up MRI scan showed a new enhancing mass at L3 level 14 months after diagnosis (Figure 1(c)). Multiple biopsies were performed that showed collagenous connective tissue with foci of hemosiderin on histopathology and no evidence of viable tumor (Figure 2(a)). Patient is now 62 months off-therapy with no evidence of disease progression and stable residual enhancement at the post-operative site on subsequent MRIs.
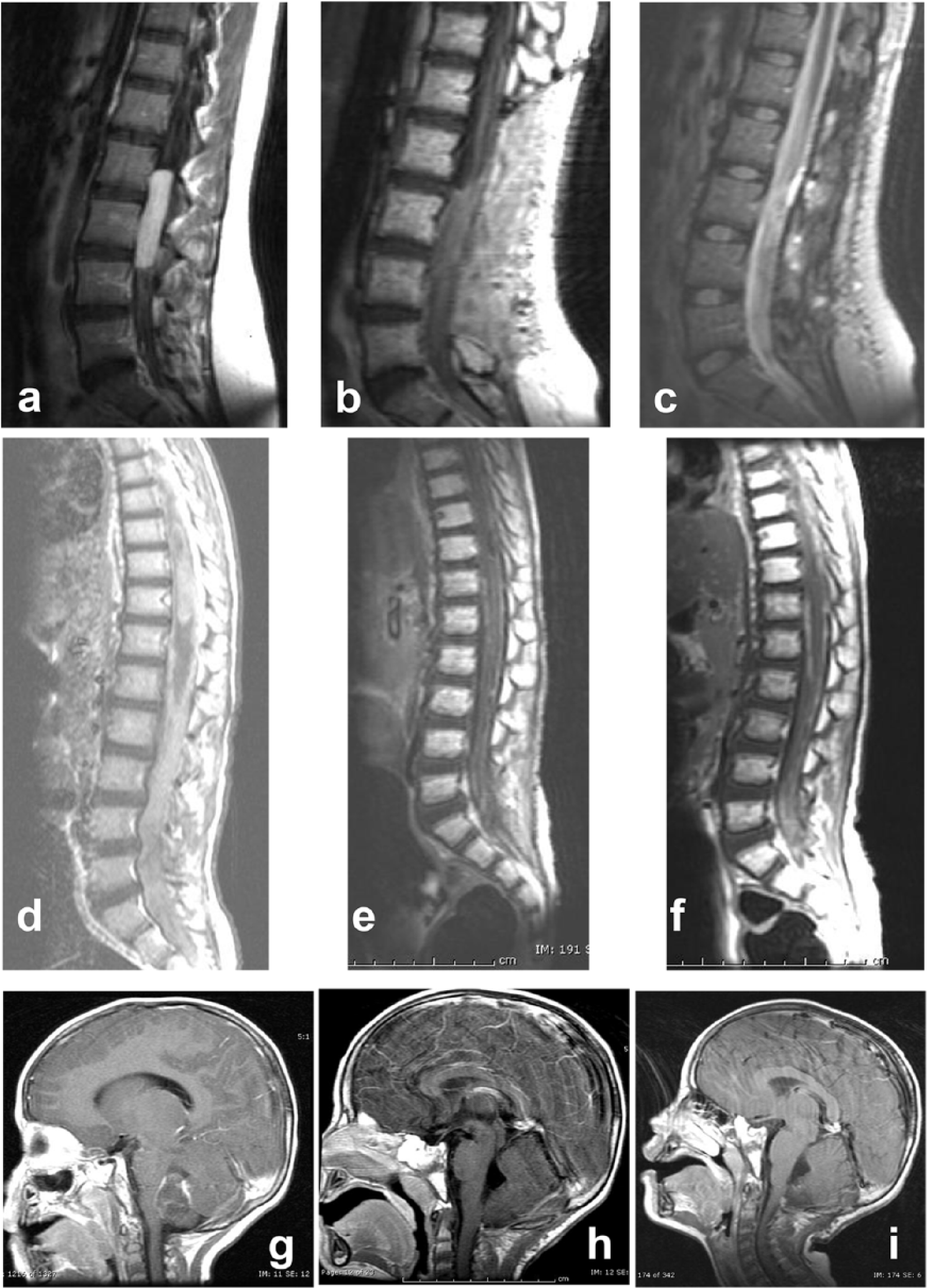
Patient 1: (a) lumbarsacral T1-weighted MRI images at diagnosis, (b) at recurrence 2 months after partial resection and radiation therapy, and (c) T2-weighted image showing new hyperintense nodule at 14 months after diagnosis. Patient 2: (d) lumbarsacral T1-weighted MRI images at diagnosis, (e) at 19 months from diagnosis showing interval increase in nodular enhancement in the region of the lower lumbarsacral spine that remained unchanged, and (f) at 23 months from diagnosis. Patient 3: (g) head T1-weighted MRI at diagnosis, (h) after resection, and (i) at 16 months from diagnosis showing a new 5-mm-enhancing nodule on the dorsal medulla.

Hematoxylin and eosin staining of histopathological samples—(a) patient 1: collagenous connective tissue with foci hemosiderin, (b) patient 2: leptomeningeal fibrosis with remote hemorrhage, and (c) patient 3: small fragments of glial tissue with no evidence of malignancy.
Patient 2 (Figure 1(d)–(f)) is a Caucasian male diagnosed at the age of 3 years with disseminated medulloblastoma with multiple leptomeningeal and parenchymal gross nodular disease in inferior cerebellar hemispheres, medulla, fourth ventricle, posterior optic chiasm, anterior temporal lobes, and thoracic spinal cord. After confirming the diagnosis, patient received five cycles of induction chemotherapy using cisplatin, vincristine, etoposide, cyclophosphamide, and high-dose methotrexate. Marked response to induction chemotherapy was documented, with almost complete response of the lesions in the brain and regression of the leptomeningeal enhancement in the spinal cord. He underwent second-look surgery after completing induction that showed viable tumor. This was followed by consolidation with a single cycle of myeloablative chemotherapy using thiotepa, carboplatin, and etoposide followed by autologous hematopoietic progenitor cell rescue (AuHPCR). The first follow-up brain and spine MRI after AuHPCR showed no evidence of residual or recurrent tumor. However, as gross residual disease had been confirmed by biopsy at the beginning of consolidation, the patient received craniospinal proton beam irradiation to 30Gy with focal boosts to 54Gy to areas of bulky disease followed by metronomic low-dose temozolomide and cis-retinoic acid for 13 months. On a follow-up MRI scan 19 months after diagnosis, small interval increase was detected in a new nodular enhancement in the region of the lower lumbarsacral spine, described as consistent with tumor recurrence (Figure 1(e)). Patient underwent a biopsy of the lesion at L3, which was reported as leptomeningeal fibrosis with remote hemorrhage and no evidence of malignancy on histopathology (Figure 2(b)). Lumbarsacral MRI at 23 months from diagnosis (1f) remained unchanged. This patient is currently doing well, with no evidence of disease progression 6 years after diagnosis and 57 months after completion of all therapy.
Patient 3 (Figure 1(g)–(i)) is an African-American male diagnosed at the age of 3 years with posterior fossa ependymoma. GTR was confirmed on post-operative MRI and was followed by IMRT to the tumor bed to 5940cGy. After resection for 16 months, he developed a new 5-mm-enhancing nodule on the dorsal medulla (Figure 1(i)), within the irradiation field, at the level of foramen magnum, persistent in repeated MRI after a month. Resection of this nodule showed reactive glial tissue with no evidence of recurrent tumor on pathology (Figure 2(c)). After completion of therapy for 77 months, this patient has no signs of radiographic or clinical progression.
Discussion
MRI provides excellent soft tissue contrast with less background interference in deep tissues, and new techniques allow assessment of molecular, physiological, and metabolic information of CNS tumors.1,9 Improved anatomical resolution allows visualization of structures previously not seen and detection of significant changes along treatment.7,8,10,11 Rapid technological advancement has brought multiple new approaches, higher resolution, and complex systems, and the expertise of the professionals interpreting the images may become a limiting step regarding the significance of the abnormalities, a phenomenon observed in other clinical scenarios, such as epilepsy or head and neck carcinomas.12–14
Despite all the advances, distinction between benign processes and recurrent malignancy has still not been reliably achieved using MRI.13–17 Considering patients with malignant CNS tumors, the scenario is even more complex due to changes caused by surgery, irradiation, and chemotherapy that evolve along time, and in many cases, the suspicious lesions are too small for functional studies.7,8 Advanced MRI techniques, such as magnetic resonance spectroscopy (MRS), diffusion/perfusion weighted sequences, diffusion tensor imaging (DTI), and positron emission tomography–computed tomography (PET-CT) have limited definition for small lesions (<2 cm) or for spinal tumors, as in two of our patients. Careful follow-up and repeated imaging at short intervals may provide information regarding the newly detected lesions, and hybrid MRI/PET imaging could be added, reducing radiation exposure and evaluating tissue metabolism.
All patients had GTR and received irradiation to the tumor bed, including proton beam therapy to patient 2. Radiological findings of radiation-induced injury in all stages can be indistinguishable from tumors, and surgical sampling is warranted for definite diagnosis.17–19 Pediatric patients present additional challenges not only for the surgical complications but also due to the most common tumors, tumor progression rates, and overall survival. The incidence of MRI abnormalities in pediatric CNS cancer patients has been described as high as 37%.20,21 The most common CNS tumors in adult patients, anaplastic astrocytoma and glioblastoma, have high recurrence rate and rapid progression, leading to the common practice of no re-biopsy, due to obvious fast progression in serial imaging and low prognosis.
Patient 1 had two lumbar spine surgeries, radiation therapy, and carboplatin chemotherapy when had a newly detected enhancing mass, barely a year after her first surgery. Under these circumstances, it is very common to find small enhancing lesions on MRI. Serial imaging every 4–6 weeks can allow careful and objective follow-up of their progression, and increasing enhancement, dimensions, or numbers will provide timely and robust indication for biopsy. Patient 2 had high-risk disseminated malignancy that responded very well to chemotherapy, leading to the indication of high-dose therapy with AuHPCR, consolidated by proton bean irradiation. His suspicious nodules were detected in the lumbarsacral spine, away from original disease sites. In his case, biopsy was warranted due to the presence of overly disseminated disease at diagnosis and the finding of viable tumor at total resection after induction chemotherapy. Histopathological finding of leptomeningeal fibrosis allowed long-term follow-up of the persistent enhancement on lumbarsacral MRI. Patient 3 had a tumor that is radiation sensitive, but poorly responsive to chemotherapy. The detection of a new enhancing nodule on MRI would certainly lead to intensive chemotherapy; the resection of the lesion and the finding of reactive glial tissue confirmed successful first-line treatment.
In this report, all patients had GTR of the primary tumors, but these considerations apply to any patient with CNS tumors, whenever biopsy and/or resection of the new suspicious lesions is feasible. At CHLA, MRI imaging of CNS tumor is obtained every 2–3 months during therapy, depending on the treatment protocol. After completion of therapy, MRI is repeated every 3 months for the first year, then every 6 months for the next 4 years. It is a routine to perform biopsy of any new suspicious enhancing lesions persisting in a repeat MRI 1 month later, as about 25%–30% of such patients present MRI abnormalities. Due to the clinical relevance of suspicious MRI findings during follow-up, high degree of evidence is fundamental to support decision-making process. Patients with higher risk of recurrence will receive more intensive therapy; therefore, with higher probability to have detectable anatomical changes in MRI scans, and further therapy for recurrent disease will incur in more toxicity and late effects. Newly detected MRI lesions should be re-evaluated by re-imaging after 1 month, with additional technique if possible, such as hybrid MRI/PET or MRS, followed by biopsy of persistent suspicious lesions to confirm malignancy and obtain sample for molecular studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
CHLA IRB does not require ethical approval for reporting individual cases or case series of up to three patients.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work of S.N.D. was supported by the Hyundai Hope on Wheels Research Grant Award, St. Baldrick’s Foundation Scholar Career Development Award, UCLA Clinical and Translational Science Institute Grant UL1TR000124, the University of California Cancer Research Coordinating Committee and UCLA Children’s Discovery and Innovation Institute (K-12 UCLA Child Health Research Center Development Award (CHRCDA)).
Informed consent
All patients were consented while still in pediatric age group. Informed consent was obtained from the parents and assent from patients when appropriate.