
Abstract
Objectives:
Although endovascular aneurysm repair of aorto-caval fistula offers a safe and efficient approach compared to traditional open repair, endovascular techniques for the treatment of aorto-caval fistula with ruptured abdominal aortic aneurysms in emergency circumstance are not well established. This study aims to evaluate the effect of endovascular repair of aorto-caval fistula of a patient with ruptured abdominal aortic aneurysm and hostile anatomy.
Methods:
we report a case of an aorto-caval fistula endovascular repaired in a 78-year-old male using a hybrid stent-graft technique.
Results:
The patient had an uneventful recovery and CTA follow up showed no sign of ACF or any endoleak.
Conclusion:
This case highlights ACF might be managed by composite endograft implantation with careful and solid sealing of anchoring zones on the two sides.
Keywords
Background
Aorto-caval fistula (ACF) is a rare complication reported in 3%–6% of all ruptured abdominal aortic aneurysms (RAAAs). 1 The majority of ACF occur spontaneously, either as a result of rupture of an existing atherosclerotic abdominal aortic aneurysm (AAA) into the vena cava or secondary to iatrogenic injuries during aorta angioplasty or surgery. 2 Symptomatic ACFs have traditionally been repaired using open surgical techniques with significant intraoperative blood loss and high operative morbidity and mortality rates. 3 Endovascular repair for RAAA (EVAR) provides an adequate, validated and safe option; however, there are limited cases that are simultaneously complicated by spontaneous ACF. We present a case that an RAAA with ACF was completely managed by hybrid aortic stent-graft implantations without inferior vena cava (IVC) endografting.
Case report
A 78-year-old male, presented to the emergency department with acute lower abdominal back pain, dyspnoea (New York Heart Association (NYHA) functional class III) and massive oedema of the lower extremities. Also, he has a medical history of remote myocardial infarction. Urgent computed tomographic angiography (CTA) demonstrated a 90-mm RAAA, with an ACF which was 12 mm in diameter. Angulated aneurysm and tortuous aorto-iliac access were also shown (Figure 1). Physical examination revealed that blood pressure was 70/52 mmHg and heart rate was 120 beats/min, which were unstable since that time. But unfortunately, laboratory investigation noted a slide decrease in haemoglobin from 90 to 72 g/L with an hour and the renal was slight impairment with 71 mL/min of glomerular filtration rate (GFR), 251 µmol/L of serum creatinine, and 15.6 mmol/L of urea.

Preoperation CT showed a 90-mm RAAA communicating with 12-mm aorto-caval fistula.
Subsequently, instead of surgical operation, an emergent endovascular approach was performed to maximize controlling the unstable haemodynamics, with a Zenith bifurcated stent-graft (Cook Medical, Bloomington, IN, USA) deployed below the origin of the bilateral renal arteries, precisely covering the ruptured aortic segment. After standard EVAR, however, persistent type Ia endoleak and Ib endoleak at the left common iliac artery (CIA) were confirmed via intraoperative angiography (Figure 2(a)). Although landing zones and device overlaps were ballooned again, the endoleaks were still existing, but we finally managed it by implanting a Gore Excluder Cuff (W.L. Gore & Associate, Flagstaff, AZ, USA) (Figure 2(b)) and a combination of Gore Excluder iliac leg with Zenith iliac leg at the left CIA (Figure 2(c)).

The angiography during the procedure: (a) intraoperative angiography showed continuing type Ia endoleak and Ib endoleak at the left common iliac artery and leakage into the venal cava; (b) a TRI-LOBE balloon was expanding to seal the Excluder Cuff stent-graft to the aneurysm neck; (c) expanding at the junction and dilating overlapping zone between Excluder iliac leg and Zenith iliac leg.
After procedure, the patient had an uneventful recovery and an impressive clinical course that could be characterized by a 10-kg weight loss and cardio-functional restoration (from NYHA class III to NYHA class II) associated with alleviating of the oedema of lower extremities. To emphasize renal protection, he was also treated with aspirin and unfractionated heparin until the renal function improved, and then fractionated heparin was carried on. The patient’s renal function was improved to 90 mL/min of GFR at 6 days after operation (Table 1) and he was symptom-free during hospitalization and discharged 10 days later, preventatively prescribed with aspirin and Rivaroxaban. Follow-up CTA at 12 months demonstrated complete resolution of ACF without type II endoleak (Figure 3).
Levels of blood test parameters at admission and on the sixth day after operation.
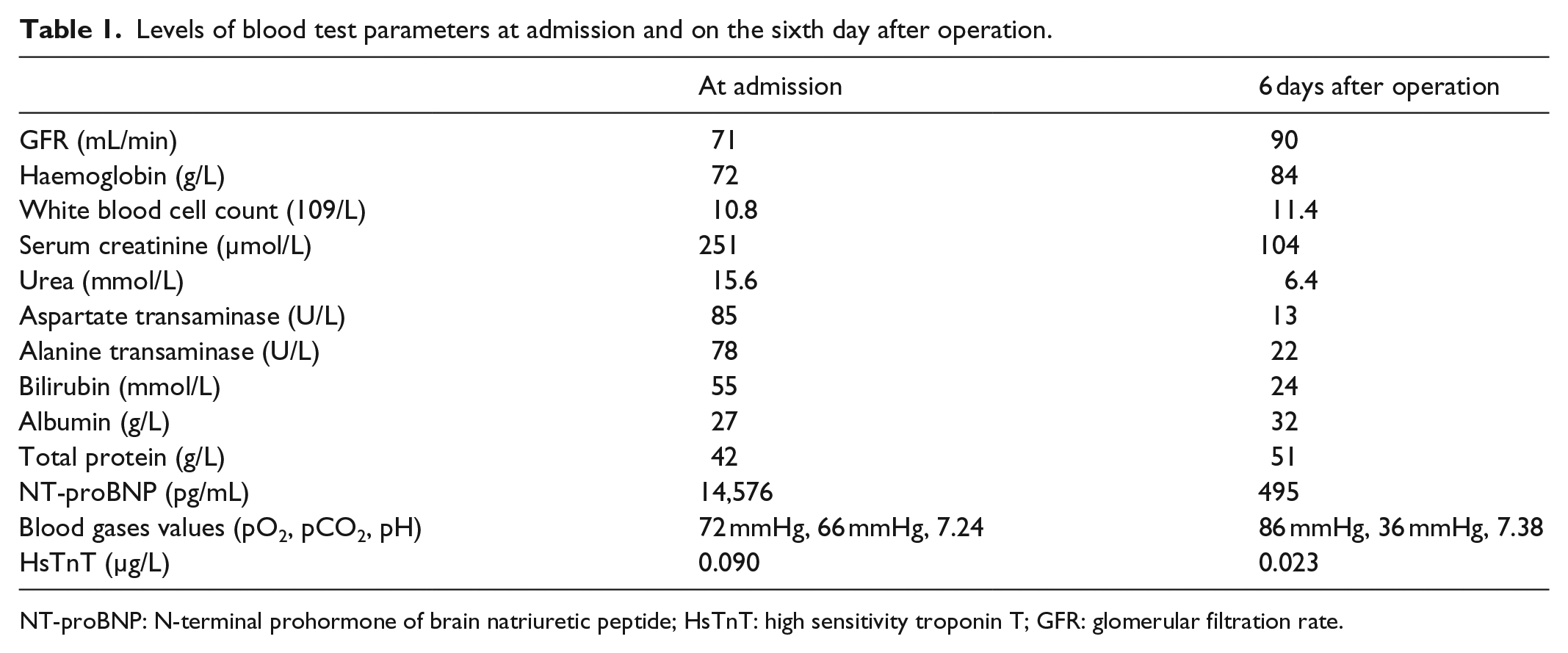
NT-proBNP: N-terminal prohormone of brain natriuretic peptide; HsTnT: high sensitivity troponin T; GFR: glomerular filtration rate.

CT angiography 12 months after EVAR procedure showing favourable remodelling of the aorta, no type II endoleak and no recurrence of the A-V, arterio-venous communication.
Discussion
Open surgical repair of RAAA with ACF consists of rapid suturing of the fistula from within the aneurismal sac which is associated with high mortality and morbidity. Calligaro et al. reviewed all reported open repairs of ACF up to 1990 and demonstrated a 30-day survival rate of 72%. Even in semi-elective cases, the mortality rate approaches 30%, especially in patients with cardiovascular decompensation. 4 However, endovascular surgery of ACF represents a good option in alternative to conventional surgery especially in old high-risk patient. 5 But patients with hostile neck anatomy developed perioperative morbidity more frequently compared with patients who have favourable anatomic neck characteristics. Antoniou et al 6 systemically reviewed the studies comparing the outcomes of EVAR in patients with hostile and friendly neck anatomy. They found that EVAR in patients with hostile neck required more adjunctive procedures to achieve proximal seal compared to the patients with friendly anatomy. Such procedures included aortic cuff insertion in most patients.
The advantage of hybrid endografting has been reported before. 7 Although there is no off label use of the available EVAR endografts or components from different manufacturers, hybrid endografting is a relatively safe and effective alternative of fenestrated and various branched endografts in emergency intervention. Theoretically different device’s characteristics facilitated utility and adjusted to the individual aorto-iliac anatomy, which is expected to improve EVAR results. 8
After AAA repair, the prevention of venous thromboembolism (VTE) should be addressed. IVC filter placement does not appear to be necessary and may be precluded by IVC dilation from central venous hypertension, especially before closure of the arteriovenous fistula (AVF). 9 But the patient treated with unfractionated heparin until the renal function improved may be necessary and then patient could be started on fractionated heparin or new oral anticoagulant NOAC after discharge. Generally, there is a dispute in optimal treatment of ACF. In the case of asymptomatic ACF, despite IVC endografting, conservative treatment could even result in favourable aneurysm sac remodelling and disappearing of type II endoleak.3,10 In this case, EVAR alone seems to close the AVF without the need of endografts in the IVC. But in other cases, some experts simultaneously intraluminal deployed endograft in both venous cava and aortic artery aiming at abolishing the shunt of high pressure blood flow from aorta to vena cava, which also had a good short-term result.11,12 Despite that, a major concern for IVC endografting is still the durability of graft patency, since veins are ‘low-flow’ vessels susceptible to thrombosis. Other potential complications include venous tears, migration, and side branch occlusion. 13 Practically, it still needs to be observed in the future.
However, as far as we are concerned, there is no specific protocol or guideline for the modern treatment of ACF with emergency endovascular procedure. The literature is continuing to build to demonstrate the feasibility of EVAR and IVC endografting for ACF.
Conclusion
ACF could be managed by solid sealing of both proximal and distal landing zones using endograft management. Although hybrid stent-graft repair of spontaneous ACF may be replaced by the newer and more suitable endovascular devices, it still remains a doable protocol in emergency circumstances. Finally, under what circumstance should we adopt IVC endografting still needs investigation. Therefore, we may not preemptively adopt IVC stent-graft inplantation and take a wait and see strategy to asymptomatic ACF and more clinical data are required to draw more solid conclusions.
Footnotes
Acknowledgements
Many thanks are given to the vascular team of the affiliated hospital of Qingdao University. All authors were involved in the preparation of this manuscript. M.L. assisted in performing the operation, collected the data and wrote the manuscript. H.W. operated and designed the study. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval
This article has been approved by the ethical committees of the Affiliated Hospital of Qingdao University No. 3745-2015.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received grant from the Science and Technology Support Program of Public Domain in Qingdao No. 2012-1-3-2-(16)-nsh.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.