
Abstract
We report a patient who had rhinogenic intracranial complication with postoperative frontal sinus pyocele and inverted papilloma in the nasal cavity. A 72-year-old woman had undergone surgery for frontal sinusitis via external incision at another hospital 13 years previously. Left-sided hemiparesis appeared in the patient and gradually worsened. Five days later, she exhibited disorientation, abnormal behavior, poor articulation, and difficulty in standing. Therefore, she was taken to the neurosurgery department by ambulance. An extensive frontal sinus pyocele was suspected, and a cerebral abscess and edema of the frontal lobe were observed on magnetic resonance imaging. After antibiotics, steroid and glycerol were administered for a few weeks; disorientation and left hemiparesis improved. Next, craniotomy for complete removal of the brain abscess by neurosurgeons and endoscopic endonasal surgery by otolaryngologists were carried out at the same surgery. From the analysis of the pathological mucosa sample taken from the right ethomoidal sinus during surgery, an inverted papilloma was diagnosed. The patient completely recovered and is currently receiving follow-up examination. Regarding rhinogenic intracranial complications, ascertaining clinical condition in order to determine the need for either immediate radical surgery, or for curative surgery after waiting for improvement of the overall body condition by conservative management, is still needed.
Keywords
Introduction
Rhinogenic intracranial complications have become rare in recent years due to advances in antibiotic development and diagnostic imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI). However, these complications still occur sometimes, and may be severe. Hence, careful diagnosis and care are required. 1 Performing surgery at the appropriate time is important in the treatment of intracranial complications. Whereas some cases require drainage in the acute stage, surgical treatment should be performed after sufficient preparation and administration of temporary treatment such as antibiotics to reduce central nervous system symptoms and acute inflammation in other cases. Here, we describe a case of nasal papilloma accompanied by intracranial complications apparently caused by an infection of a postoperative frontal sinus pyocele, including clinical course, treatment, and other clinical details as a contribution to the literature.
Case report
A 72-year-old woman complaining of occipital pain and mild dizziness after a recent bout of the common cold was placed under observation. Left-sided hemiparesis appeared and gradually worsened. Five days later, she exhibited disorientation, abnormal behavior, poor articulation, and difficulty in standing. Therefore, the patient was taken to a nearby neurosurgery department by ambulance. An extensive frontal sinus cyst was suspected, and a cerebral abscess and edema of the frontal lobe were observed on MRI. The patient had undergone surgery for frontal sinusitis via external incision at another hospital 13 years previously.
At initial examination, patient consciousness level according to the Glasgow Coma Scale (GCS) was E4V3M5, and the patient exhibited disorientation and partial left hemiparesis. Antibiotics (meropenem hydrate (MEPM) 1.0 g/day), step-down steroid therapy (betamethasone 4 mg), and glycerol (400 mL/day) were administered. Although the patient was still experienced disorientation, improvement in hemiparesis was observed on day 1. Therefore, emergency drainage of the cyst was not performed. After 10 days, slight disorientation was still present, but improvement in patient responses for compellation was observed. According to MRI, however, the frontal sinus lesion and intracranial abscess remained. Therefore, the patient was transferred to the neurosurgery department in our hospital for radical surgery 18 days after admission. Soft tissue shadows in the patient’s upper-right ethmoid sinus and a large cyst in the right frontal sinus accompanied by bone thinning were observed according to CT performed at our hospital (Figure 1). Displacement of the posterior wall of the right frontal sinus into the cranium was observed by MRI. Hypointensity was observed on T1-weighted images (Figure 2(a)) and hyperintensity on T2-weighted images (Figure 2(b)). A ring-shaped mass with an inner diameter of 1.5 cm and surrounding edema were observed in the right frontal lobe (Figures 2(b) and (c)). Contrast enhancement was seen on the margins of the frontal sinus pyocele and cerebral abscess (Figure 2c). They were removed via craniotomy and endoscopic sinus surgery (ESS) performed jointly with the neurosurgery department. At first, a right frontotemporal craniotomy was performed extending across the midline. Following burr hole placement, frank pus was drained and the pyocele was seen filling the right frontal region. Location of the brain abscess was confirmed by ultrasonography and then removed by detaching each capsule. The frontal sinus pyocele capsules were also completely removed. Next, the nasal cavity and frontal sinus passages were opened by ESS. At this time, a mucosa sample was taken from the right ethomoid sinus and a permanent pathological examination was performed. Next the pericranial flap was used to cover the frontal sinus defect. The head incision was closed after filling the cavity space with fat from the thigh.
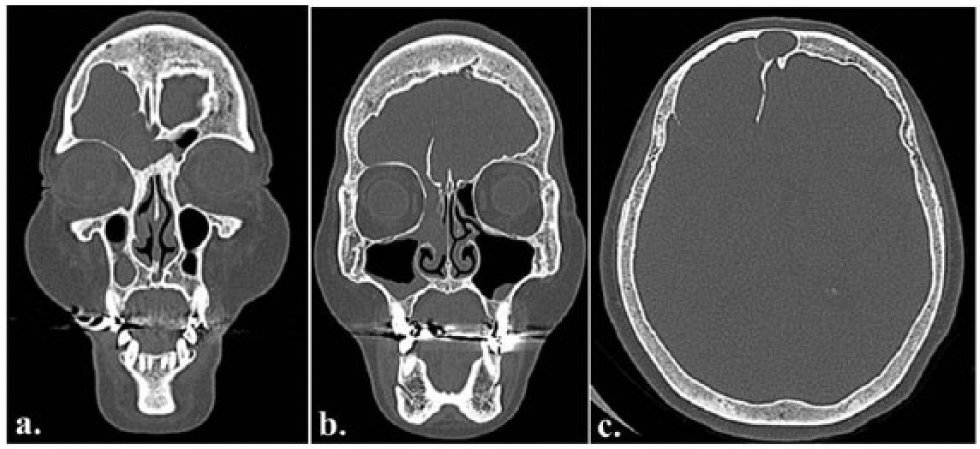
Pre-operative CT showed soft-tissue shadowing in the frontal sinus, with cystic enlargement to the posterior wall of the right frontal sinus; bone thinning was also noted. Soft tissue shadowing was also observed in the right anterior ethmoid sinus.

MRI showed brain abscess and edema on the frontal lobe due to inflammation of giant frontal sinus pyocele: (a) T1-weighted image, (b) T2-weighted image, and (c) contrast-enhanced T1-weighted.
After surgery, the patient underwent rehabilitation and was discharged 38 days later. Two months postoperatively, a CT exam showed that the cyst had disappeared from the posterior wall of the frontal sinus (Figure 3). An MRI performed after 4 months from the patient discharge disclosed hyperintensity in the frontal sinus which was thought to be fat, but no signs of abscess (Figure 4). From the analysis of the pathological mucosa sample taken from the right ethomoidal sinus during surgery, an inverted papilloma was later diagnosed. At the time of the last follow-up, 36 months have passed since surgery. The patient was under close outpatient observation for recurrence of the papilloma.
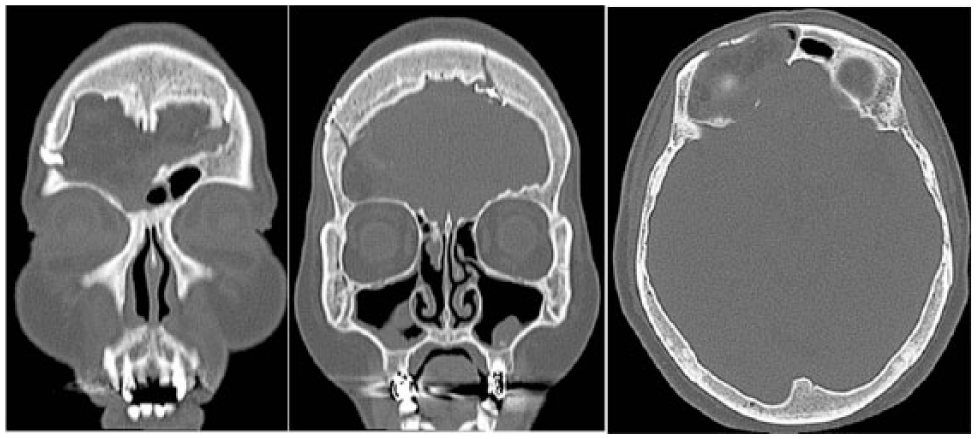
Postoperative CT showed no cyst in the frontal sinus posterior wall.

Postoperative MRI showed high signal of the fat in the frontal sinus but did not show any abscesses.
Discussion
Rhinogenic intracranial complications include intracranial diseases such as brain abscess, meningitis, subdural abscess, epidural abscess, or sinus thrombosis that accompany inflammatory diseases of the nose and sinuses.1–3 While recent advances in the development of antibiotics have reduced the chances of contracting these diseases, some patients are still at risk. Since these conditions can be life-threatening, patients should be monitored for symptoms of these diseases. 1 In particular, subdural abscesses have been reported to have a mortality rate of 10%–20% since antibiotics have difficulty in entering the intradural space. 4 Surgical therapy for intradural abscesses includes drainage of the abscess in the acute stage or surgery after administration of conservative therapy. However, treatment selection depends on the type of surgery to be performed. According to our research, no reports have addressed the optimal timing for surgical treatment of rhinogenic intracranial complications based on the patient’s consciousness level. As a criterion for performing brain surgery, patient consciousness level should not only be evaluated once at the initial examination but also when there is any decrease in patient consciousness level afterwards, and should be considered alongside any worsening of central nervous system symptoms, such as are seen in cases of poorly controlled brain or subdural abscesses. In other words, when there is a pressing need to operate, a decrease in the state of consciousness is considered to carry more weight than that of the initial examination.
Regarding the etiology in this case, the patient had undergone surgery for frontal sinusitis via external incision 13 years previously. It is possible that a papilloma existed at that time, but details of the previous operation are unclear. Over the course of many years, the papilloma may have recurred, and as it grew formed a frontal sinus pyocele. The frontal sinus pyocele may have become infected after a recent bout with a common cold, which then caused intracranial complications. In patients with a history of surgery for sinusitis, it is conceivable that intracranial complications could occur due to postoperative cyst formation and local infection. However in this case, papilloma was not observed during preoperative imaging. Cases in which papilloma of the sinonasal region progress into the cranium are rare. Of 11 reports available, only 1 described central nervous system symptoms (epileptic seizures). 5 Similar to this case, the authors reported a serious case of inverted papilloma presenting with acute neurological deterioration secondary to a large frontal sinus mucocele eroding the frontal sinus. Craniofacial resection, combined with ESS, was performed to achieve a complete recovery with no lingering disability. However, in that case, the abscess extended outside the cranium. In seven cases extending outside of the cranium, a mean of 4 disease-free years was achieved, but for three of the four cases extending inside of the cranium, mortality at a mean of 9 months after surgery was reported. 5 In this case, although an intracranial abscess had formed, the papilloma was thought to be limited to the inside the nose.
According to our experience, when pathological mucosa is observed during surgery, a quick intraoperative diagnosis should be provided even in cases of acute inflammation.
Rhinogenic intracranial complications most often originate in the frontal sinuses. Regarding the mechanisms of how these advance into the cranium, venous return in the frontal sinuses occurs as veins perforate their posterior walls and flow into the sagittal sinuses. 6 Veins from the brain parenchyma also connect to the sagittal sinuses, and most cases of bacterial thrombophlebitis are caused by reverse flow in this area. 6 Moreover, Thomas and Nel 7 reported that the frontal sinus mucosa is separated from the diploic vein by only an extremely thin bone wall, and veins of the sinus mucosa can freely communicate with the diploic vein and veins of the dura mater. Since these veins do not have flaps, reverse blood flow can occur. 7 In this case, thinning of the bone at the posterior wall of the frontal sinus cyst was observed by CT imaging. Hence, we consider that the subdural abscess was caused by a direct infection in this area.
Intracranial abscesses can be treated surgically through suctioning via trephination, removal by drainage though small trephination, 8 or radical resection using craniotomy. Methods that use trephination are minimally invasive and can be performed with local anesthesia. However, they are limited in their ability to remove the cause of the disease and might not achieve sufficient pus drainage. On the other hand, resecting an abscess through craniotomy is more invasive and requires general anesthesia. However, pathological focus can be confirmed by direct observation and handled definitively. Nathoo et al. 9 examined 699 cases of subdural abscesses and found a lower mortality rate and functional prognosis with primary craniotomy compared to drainage through small trephination. However, the importance of considering preoperative findings has also been pointed out; and in particular, patient survival prognoses has been shown to be directly related to the preoperative consciousness level. 10
Recent studies have reported on the treatment of intracranial complications accompanying frontal sinusitis by ESS.11,12 Gallagher et al. stated that ESS is the preferred surgical style for frontal sinus diseases, since opening the osteomeatal complex is important in treating these diseases. Views are divided as to whether to treat the sinuses or the intracranial lesions first. Although there are differences depending on the brain abscess size and location of the lesion, patients do not require repeated surgeries when the otorhinology and neurosurgery departments work cooperatively together for these surgeries. 13
In this case, conservative therapy was administered in the acute stage. After the central nervous symptoms improved and preparations for surgery were made, otolaryngologists and neurosurgeons jointly performed radical surgery. Our experience shows that a case with an initial consciousness level of GCS E4V3M5 could be placed under observation using antibiotics and steroids to reduce central nervous system symptoms and acute inflammation for the prepared surgery. In the future, more cases of rhinogenic intracranial complications with varying levels of central nervous system function should be examined.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.