
Abstract
Objectives:
This case report looks at a 53-year-old patient who had suffered a penetrating foreign body injury to the retro-orbital space and the surgical approach taken to remove the large glass fragments found and to correct the damage caused. Having fallen while holding a drinking glass, this patient suffered multiple laceration injuries to the maxillofacial region upon the glass shattering in contact with the face. However, unbeknownst to the patient, several glass fragments became embedded in the retro-orbital space, and this was only detected on presentation 2 days post-injury with unusual symptoms of sharp, sudden pain elicited on extreme gaze as well as ocular motility restriction.
Methods:
This embedded foreign body required a creative surgical approach to remove it involving gaining access to the retro-orbital space via a superior approach and cautiously following the path the glass shards took upon entry, all the way to the posterior aspect of superior rectus. Intra-operative radiographic guidance was required due to the restriction of operating within this space and particularly when removing glass fragments distal to superior rectus.
Results and Conclusion:
The patient recovered well and experienced an immediate improvement in ocular motility with a return to relative normality over the next few months.
Introduction
Foreign Body embedding can commonly occur following traumatic injuries of a penetrating nature. 1 The presence of a foreign body within a wound or anatomical space can result in unusual and unexpected signs/symptoms,1,2 and one should always be suspicious of foreign body presence when managing a patient with traumatic injuries.
If left untreated, foreign bodies have the potential to cause a multitude of problems 3 ranging from infection to loss of function 4 and are best removed as soon as possible after identification. However, respect must be given to nearby vital structures when removing a foreign body, particularly as in this case, with the foreign body being present within the retro-orbital space.
Case report
A 53-year-old female presented to University Hospital Aintree Accident and Emergency Department with pain and swelling around the right eye having suffered a traumatic injury 2 days previously. The patient tripped and fell while holding a drinking glass, resulting in said glass shattering upon contact with the face.
Having suffered some minor laceration injuries, the patient did not consider herself to be particularly injured and did not seek medical treatment at this time. However, over the following 2 days, pain and oedema began to worsen around the right eye, resulting in the patient presenting to Accident and Emergency.
On presentation, the patient had significant peri-orbital oedema around the right eye and a sub-conjunctival haemorrhage was visible (Figures 1 and 2). Ocular motility was restricted with sudden sharp pain elicited behind the right eye on superior and inferior gaze. Bony examination did not reveal any signs of fracture and palpation did not elicit pain.

Patient on initial presentation showing significant right-sided peri-orbital oedema and sub-conjunctival haemorrhage with mild infra-orbital ecchymosis. Smaller laceration/abrasion injuries to forehead can also be seen.

Patient on initial presentation showing significant right-sided peri-orbital oedema and sub-conjunctival haemorrhage with mild infra-orbital ecchymosis.
Vision was measured right eye 6/6 and left eye 6/9, and the patient did not report any perceived change in vision or colour vision from the norm. Vertical diplopia was present at superior and inferior gaze, with reversal between the two points. A small 15 mm laceration injury was present superior to the right eyebrow.
Due to the patient’s restriction in ocular motility, radiographs were requested to initially assess any bony injury. A standard occipitomental plain film view was taken (Figure 3). Upon reviewing the occipitomental study, a clear anomaly was noted overlying the right orbit. A large radio-opaque mass with sharply defined margins was apparent within the orbital contents of the right side. This was reported to be a possible foreign body within the right orbit.

Occipitomental view plain film radiograph demonstrating a large radio-opaque mass over the right orbit.
A head computed tomography (CT) scan was taken following this, in order to more accurately localize the radio-opaque mass and assess the surrounding vital structures for signs of damage. Upon reviewing the CT study, multiple radio-opaque areas of hyperattenuation were detected in and around the right orbit (Figure 4). With the largest being a 1.8 × 1.1 × 1.0 cm mass within the right retro-orbital space, directly in contact with the superior rectus muscle. Smaller fragments were also visible in the right pre-septal space and sub-cutaneous tissue. Thankfully, the globe appeared intact, as did the optic nerve.

(a–c) Head CT scan, selected axial plane slices demonstrating a right-sided retro-orbital area of hyperattenuation in direct contact with superior rectus, as well as smaller hyperattenuation areas in the pre-septal soft tissues.
Following the history, clinical examinations and special investigations, a diagnosis was achieved. The patient had peri-orbital oedema and a sub-conjunctival haemorrhage as well as restriction in ocular motility.
Due to the evidence of direct impingement on the superior rectus muscle, it was evident that this fragment/foreign body was resulting in the ocular motility restriction and pain elicited upon eye movement. The following multi-point diagnosis was made:
Peri-orbital oedema and sub-conjunctival haemorrhage of right eye with foreign body embedding in right retro-orbital and pre-septal spaces;
Resultant pain and restriction of eye movement due to ocular muscle impingement;
Foreign body, most likely glass fragments of varying sizes.
Due to the large foreign body present in the right retro-orbital space and the associated pain/impingement on muscles, intervention was required. A surgical approach was decided upon in order to attempt to remove the foreign body and assess the extent of the damage. Due to the known restriction of operating within the retro-orbital space, radiographic guidance would be required intra-operatively. The patient was consented for exploration of the right orbit and removal of foreign bodies under radiographic guidance. Consent was also obtained for clinical photographs and documentation of a case report.
Surgery went ahead under general anaesthesia. Initially, the sub-cutaneous glass fragments were removed and the area thoroughly cleansed with sterile saline irrigation. In order to access the larger retro-orbital glass fragment, the decision was made to enter via the existing wound and cautiously follow the path the fragment took upon entry. In order to achieve adequate access, the wound was widened slightly to allow for effective retraction and visualization. Within the right orbit, a superior approach was undertaken deep to periosteum, which allowed for negotiation to the retro-orbital region. The large retro-orbital foreign bodies were identified immediately distal to superior rectus.
At this stage, positional imaging was acquired with intensifying screens to verify instrument angulation, approach and position. The large foreign bodies were successfully removed and withdrawn along virtually the same path by which they entered. Complete removal was verified with another intra-operative radiograph (Figure 5).

Intra-operative radiographs: (a) prior to removal of large glass fragment – instrument angulation and position seen in a superior pathway of approach to the foreign body; (b) following removal of glass fragment indicating complete removal.
Thorough irrigation and cleansing was undertaken. Haemostasis was verified and the surgical site closed in layers. Following surgery, the patient remained with the Maxillofacial Unit and regular eye observations were undertaken on the ward overnight.
Following surgical intervention, the patient had an uneventful recovery. The patient reported immediately that the pain behind the right eye had gone. Clinical examination post-operatively, the following morning, revealed an improvement in ocular motility of the right eye, with no pain elicited on extremes of gaze and no diplopia. The patient was discharged later the same day.
At 1 week follow-up, it was noted the patient was pain free and the ocular motility had further improved. Some mild restriction remained and this was deemed to be down to weakness of the superior rectus muscle and contracture of the inferior rectus muscle. A mild ptosis of the right eyelid was also noted. The patient was placed on long-term follow-up with a view to potentially provide a levator prosthesis/ptosis repair if the ptosis does not improve with time.
Over the following 5-month long-term follow-up, the patient had three Hess chart plottings undertaken that indicated a significant improvement over time, returning to a relative state of normality (Figure 6). Initially, a lingering restriction to superior movements was present; however, as time passed, this became less profound and normalized in the fullness of time. The patient reported that she is pleased with the outcome of her treatment by the Maxillofacial Surgery Unit.
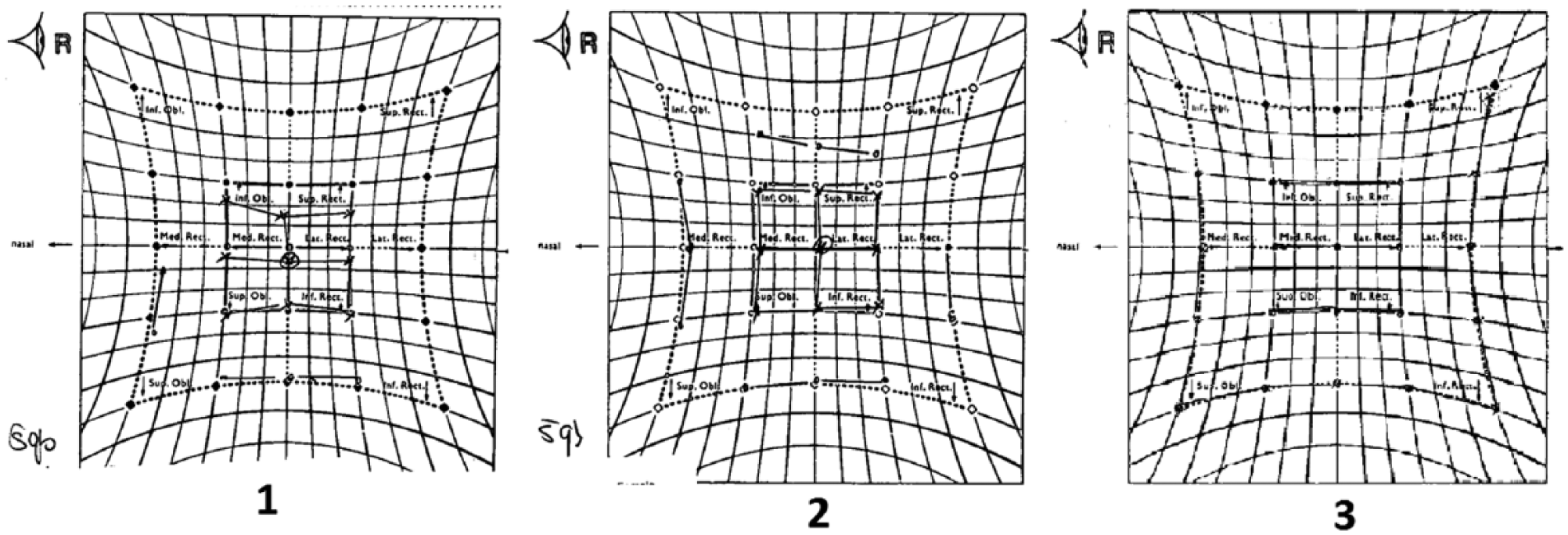
Hess charts showing improvement in right eye restriction over a 5-month period. (a) Post-operatively indicating a remaining restriction in elevation. (b) Two months progress indicating improvement and a reduction in restriction observed. (c) Further 3 months progress indicating a return to a state of relative normality.
Discussion
Any penetrating injury carries with it a risk of foreign body embedding. Injuries to the maxillofacial region most often stem from road traffic collisions (RTCs) or inter-personal violence. 5 With both these mechanisms, there is the potential for contamination of wounds with debris/foreign bodies, 6 with RTCs often resulting in a spectrum of foreign body debris – stones/gravel, glass, metal.
Foreign bodies can be missed on clinical examination and are often only apparent when relevant imaging is taken. However, imaging techniques are not a fool-proof method of detecting foreign bodies. Glass, wood and plastic in particular are not always obvious on radiographs (plain or CT). 7 Glass and plastic detection rates are reduced when embedded in muscular tissue or in close proximity to radio-dense structures such as bone, making foreign bodies in the maxillofacial region particularly challenging to detect at times and three-dimensional (3D) reconstruction rendering is often required to visualize the fragments. 8 If undetected, glass foreign bodies in particular can result in unfavourable consequences for the patient. 3
It has been documented that embedded glass in particular can migrate through soft tissue and result in significant damage to nearby structures such as nerves and vessels. 3 With a reported case of up to approximately 12.5 cm migration in a single day. 3
Other associated signs/symptoms can result in a re-presentation of the patient. This may arouse suspicion of an embedded foreign body, particularly as migration is often delayed and associated with healing of the injured tissues. 9 Hence, it is always important to be suspicious of a foreign body in any wound that may present. A re-attending patient presenting with unusual or delayed healing combined with the following signs and symptoms should raise suspicion of a foreign body:
Approximately 70% of patients re-presenting due to embedded foreign body had experienced altered sensation/unusual sensation localized to the injury that manifested as healing progressed rather than at initial injury. 2
Approximately 20% experienced delayed or fibrotic healing, 2 or persistent infection/discharge/chronic sinus. 4
Approximately 10% experienced pain from old injury. The character of the pain could be sudden, unusual character, acute, sharp and usually not associated with a healing wound. 2
Pain from old injury elicited on movement of hyperextension and in far position of gaze. 2
Conclusion
One should always be mindful when dealing with traumatic injuries; the possibility of foreign body embedding must be considered when examining any wound and in particular penetrating injuries. Patients could potentially be discharged with undetected foreign bodies, and this may result in significant issues. A ‘normal/clear’ radiograph or CT scan should not be taken as definitive proof that there is no possibility of a foreign body as the nature of the material and its position may render it undetectable with standard imaging techniques. Thorough history and examination are key, and wounds should be closely inspected.
Footnotes
Acknowledgements
The authors acknowledge the excellent guidance and leadership of Professor Richard Shaw – Consultant Maxillofacial Surgeon, Aintree Hospital, Consultant for Maxillofacial trauma at the time of injury – within the management of this case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information and images to be published in this article. Written and signed documentation of this consent is within the patient’s hospital records. Copies of the consent forms are available upon request.