
Abstract
Reports on the trans-lamina terminalis and trans-third ventricular approach are rare. The risk associated with this approach is unknown. After an unsuccessful endovascular surgery, we performed direct surgical clipping via the third ventricle on a 78-year-old woman presenting with an extremely high-positioned, ruptured basilar tip aneurysm. She experienced transient hypothermia for 5 days, and it was considered that this was due to hypothalamic dysfunction. It is necessary to recognize that there is the potential for hypothermia after surgery via the lamina terminalis and third ventricle, even though the mechanisms of hypothalamic thermoregulation are still unclear.
Introduction
With recent advances in the treatment of cerebral aneurysms, endovascular treatment is increasingly becoming the surgical intervention of choice, especially for aneurysms of the posterior circulation. However, in cases which fail to respond to endovascular treatment, direct clipping of the aneurysm has to be performed. Therefore, the quality and safety of direct clipping in such cases are important. We describe the case of a ruptured, extreme high-position, basilar tip aneurysm treated by direct clipping via the third ventricle, in which transient hypothermia occurred after surgery.
Case report
Patient’s informed consent to report this case was obtained. We have been approved to report this report in Clinical Research Institutional Review Board of our institution.
A 78-year-old woman, who had a medical history of hypertension and diabetes, complained of sudden severe headache and vomiting. On admission, the patient exhibited a moderate disturbance in consciousness, with the respective scores on the Glasgow Coma Scale and Hunt and Hess grading of 13 and 3 with World Federation of Neurosurgical Societies (WFNS) grade 2. Computed tomography (CT) demonstrated subarachnoid hemorrhage (Figure 1), and three-dimensional computed tomographic angiography (3DCTA) demonstrated an aneurysm, which was 4 mm in diameter at the tip of the basilar artery. The height from the posterior clinoid process to the aneurysm was 22 mm (Figure 2). When endovascular surgery was first attempted, the microcatheter could not reach the aneurysm because of a crooked vertebral artery (Figure 3). Therefore, we had to select surgical clipping. We adopted the trans-lamina terminalis and trans-third ventricle approach, after confirming the pathway to the basilar tip aneurysm on a sagittal view with a magnetic resonance imaging (MRI) (Figure 4). The interhemispheric fissure was divided by a sharp or blunt dissection to expose the lamina terminalis during the operation. We confirmed the position of the floor of the third ventricle and also the mesencephalic aqueduct behind the opened lamina terminalis (Figure 5, left). On opening the floor of the third ventricle, we could confirm the sclerosed yellow basilar artery and the basilar tip aneurysm (Figure 5, right). We performed the neck clipping after temporary clipping of the basilar aneurysm. The patient’s level of consciousness gradually improved after the procedure; however, hypothermia persisted to day 6 post-surgery (Figure 6). The lowest temperature registered was 33.3°C on the fourth postoperative day. Postoperative CT/MRI did not indicate any hypothalamic damage. Endocrinological examination did not reveal hypothyroidism or hypopituitarism (adrenocorticotropic hormone (ACTH): 57.3 pg/mL; thyroid-stimulating hormone (TSH): 0.90 mIU/mL; luteinizing hormone (LH): 17.4 mIU/mL; follicle stimulating hormone (FSH): 48.6 mIU/mL; growth hormone (GH): 0.081 ng/mL; prolactin (PRL): 28.55 ng/mL). We warmed the patient with an electric blanket for 3 consecutive days. 3DCTA did not show cerebral vasospasm, and we confirmed that the aneurysm was absent on the sixth postoperative day (Figure 7). The hypothermia gradually improved after the seventh postoperative day. On subsequent discharge, the patient had mild dementia and depression; however, the dementia improved, and 3 months after discharge, she was grade 2 on the modified Rankin Scale.

Computed tomography (CT) on admission showing subarachnoid hemorrhage.
(Left) Three-dimensional computed tomographic angiography (3DCTA) showing an aneurysm at the tip of basilar artery. (Right) CT showing the distance (22 mm) between the tip of posterior clinoid process and aneurysmal neck.

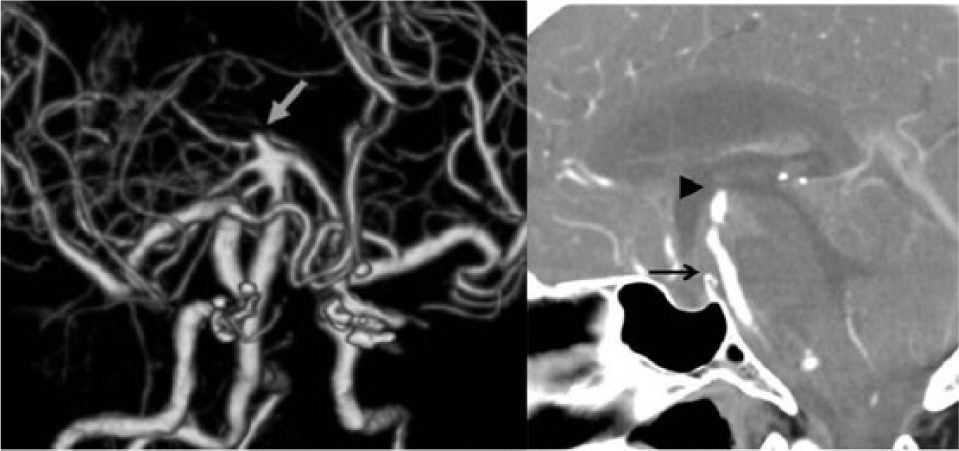
(Left) Three-dimensional computed tomographic angiography (3DCTA) (posterior view) showing the origin of right vertebral artery narrow and curved. (Right) Digital subtraction angiography showing crooked left vertebral artery.

Sagittal view of magnetic resonance imaging (MRI) showing the basilar apex aneurysm pushing up the third ventricle floor (arrow).

Intraoperative photographs. (Left) Opened lamina terminalis (arrow) and bilateral A1. (Right) The sclerosed yellow basilar artery (BA) with temporary clip (arrow head) and aneurysmal neck (arrow) at the back of opened third ventricle floor.
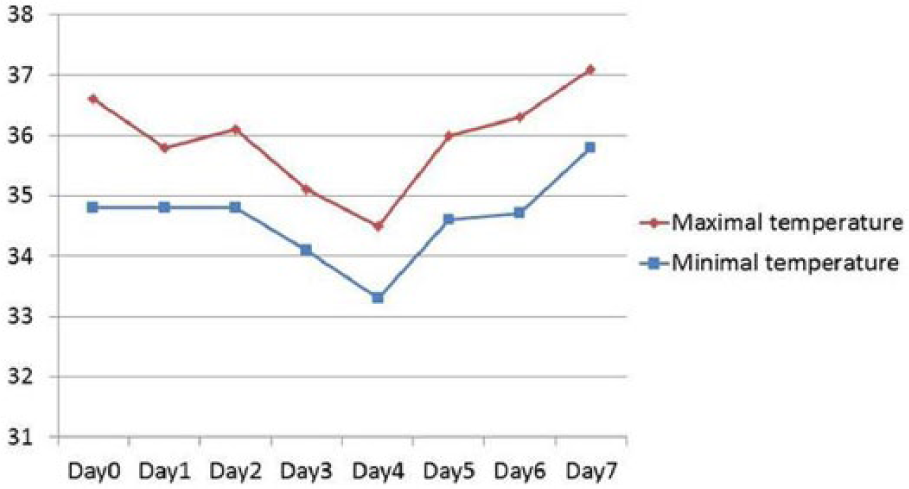
Postoperative temperature chart.

Postoperative 3DCTA showed the absence of aneurysm.
Discussion
Many approaches with various modifications have been implemented in the treatment of basilar bifurcation aneurysm.1–5 Nevertheless, it is sometimes impractical to treat a high-position basilar bifurcation aneurysm with conventional approaches. In our case, the basilar artery aneurysm was located at an extremely high-position. Because the surgery for high-position basilar aneurysms is one of the most difficult operations in neurosurgery, in this present case, we attempted surgical intervention with the trans-lamina terminalis third ventricular approach. This approach is limited to small aneurysms because of a narrow surgical field. Aneurysms measuring 5 mm or less are good candidates, because the average area of lamina terminalis is 52.84 mm2 (31.5–83.25 mm2); 6 aneurysm exists in a deeper position. The interpretation of the preoperative image is absolutely necessary in this approach. In our case, during the operation, single-shaft forceps were highly useful, as only a narrow operative field was available for surgical maneuver. To our knowledge, only five cases of surgical clipping with the trans-third ventricular approach have been reported in the past (Table 1).7–10 However, hypothermia after surgery did not occur in any of these cases. Although there is one previous report of hypothermia following surgical removal of a craniopharyngioma, 11 this is the first report of hypothermia following surgical clipping. In our case, the hypothermia was suspected to have been derived from related damage to the hypothalamus. Of the many important functional nuclei of the hypothalamus present in the lateral walls of the third ventricle, the medial preoptic/anterior hypothalamic area (POA) is considered the primary thermosensitive area of the central nervous system.12,13 In vitro studies have indicated that the POA contains the warm-sensitive (WS), cold-sensitive, and temperature-insensitive neurons. 14 The WS neurons, which trigger responses for heat loss (skin vasodilation and sweating), are activated by increased core temperatures and are inhibited by inputs from cold receptors in the skin, possibly via the responses of the temperature-insensitive preoptic hypothalamic neurons. The relationship between POA and hypothermia has been documented in animal studies. 15 The dorsomedial nucleus of the hypothalamus is also considered a thermosensitive area.13,16 In the trans-third ventricular approach, the hypothalamus is not directly damaged, although it is necessary to surgically expose the floor of the third ventricle for access to the basilar tip. Although postoperative CT/MRI did not show any hypothalamic damage, it is possible that retraction affected the hypothalamic nucleus surrounding the third ventricle because the operative field of this approach is very limited. More cases are required to understand the risk of hypothalamic complications from this procedure.
Reports of trans-third ventricle approach for basilar bifurcation aneurysm.

WFNS: World Federation of Neurosurgical Societies; NA: not available; PCP: posterior clinoid process.
Conclusion
We reported the first case of transient hypothermia apparently related to a hypothalamic disorder after surgery with interhemispheric trans-third ventricular approach for high-position basilar tip aneurysm. Possible occurrence of transient hypothermia should be noted during the operative period using this approach.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
No funds were received from any source to complete this work.