
Abstract
Objectives:
Mycotic pseudoaneurysms of the extracranial internal carotid artery are rare, and their management often represents a challenge, but treatment is necessary due to the high risk of rupture and distal brain embolization. Systemic antibiotics associated with open surgical excision of the infected tissues and carotid reconstruction using autologous grafts are the treatment of choice. The use of endovascular techniques still remains controversial in infective fields; however, it can be an attractive alternative in high-risk patients or more often as a “temporary” solution to achieve immediate bleeding control for a safe surgical reconstruction.
Methods:
We discuss the unusual case of an extracranial right internal carotid artery mycotic pseudoaneurysm following methicillin-resistant Staphylococcus aureus infection, in a patient with poor general conditions.
Results and Conclusion:
The lesion was successfully treated using a hybrid endovascular and surgical procedure.
Introduction
Mycotic pseudoaneurysms are uncommon occurrences. In the majority of cases, they are localized at the femoral artery and usually are consequent to a septicemia after drug injections or iatrogenic maneuvers.
Mycotic pseudoaneurysms of the extracranial internal carotid artery (ICA) are even more rare, and they are challenging to manage, being associated with a high morbidity and mortality. 1 The pathogenesis of these lesions is still under investigation, even if predisposing factors seem to exist. 1
Treatment is necessary, due to the high risk of rupture and distal brain embolization. 2 Systemic antibiotics associated with traditional open surgical approaches are the treatment of choice, usually including arterial ligation, debridement of surrounding tissues, and in situ or extra-anatomical revascularization. 2 The use of endovascular techniques still remains controversial in infective fields; however, it can be an attractive alternative in high prohibitive risk patients, in instances of a challenging surgical approach 3 or as a “bridge” solution to achieve immediate bleeding control for a safe surgical reconstruction.
We report the unusual case of a extracranial right ICA mycotic pseudoaneurysm and a left femoral pseudoaneurysm following methicillin-resistant Staphylococcus aureus (MRSA) infection of a femoropopliteal bypass, in a patient with coagulopathy due to alcoholic liver disease. The carotid pseudoaneurysm was successfully treated using a hybrid endovascular and surgical procedure, while the femoral pseudoaneurysm was treated through a conventional surgical approach.
Case report
An 81-year-old man arrived at IRCCS Policlinico’s Operative Unit of Vascular Surgery for a distal wound abscess of a right below-the-knee femoropopliteal composite bypass (prosthesis and autologous great saphenous vein), following a critical limb ischemia which occurred the previous month. A wound culture was positive for MRSA, which was sensitive to Teicoplanin.
The patient had a history of alcoholic liver disease and atrial fibrillation which had not been treated using anticoagulation therapy. He had also previously undergone a left carotid stenting for a significant asymptomatic stenosis and an endovascular exclusion of a left iliac aneurysm.
On admission, the patient had no fever. Blood tests were normal except for hemoglobin 12 g/dL and International Normalized Ratio (INR) of prothrombin time 1.38, and blood cultures were negative.
On physical examination, the patient was very thin and emaciated, with a body mass index (BMI) of 15. His abdomen was treatable, and no masses were palpable; physical and laboratory examinations of the heart and chest were normal. Femoral pulses were palpable bilaterally; popliteal and tibial pulses were absent bilaterally. The right femoropopliteal bypass was patent, having a valid flow at Duplex-scan examination. There was no exposure of the graft through the infected wound. The patient was immediately posed on anticoagulation using low-molecular-weight heparin and underwent intravenous antibiotic therapy using Teicoplanin 400 mg daily.
Four days later, an acute limb ischemia occurred, associated with bypass thrombosis and a significant increase of white blood cells count at laboratory tests. Moreover, the patient developed fever.
Under spinal anesthesia, surgical exploration of the popliteal artery below the knee was thus performed, but no run-off from tibial vessels was found. The graft was removed and, since ischemia had become irreversible, the patient eventually underwent right thigh amputation.
Postoperative course was uneventful, white blood cells count normalized, and the fever disappeared. No additional signs of infection were detected, and the wound of the stump was clean; however, antibiotic therapy with Teicoplanin was continued. The patient was discharged on the ninth postoperative day (POD) and referred to a clinic for rehabilitation.
Twenty-seven days later, the patient suddenly developed a pulsatile mass in the right side of his neck and another pulsatile mass in his left groin. He also had dysphagia and two episodes of hemoptysis. He underwent a duplex ultrasound of the neck and the left groin and an angio-computed tomography (CT) scan, both showing the presence of a right hypodense bulk at the common carotid artery and at the bifurcation, 40 × 37 mm in diameter, which extended for 58 mm in length and involved the ICA, dislocating the right internal jugular vein and invading the nearby parapharyngeal space (Figure 1). The mass seemed to resemble a pseudoaneurysm, as flow was recorded at duplex ultrasound examination (Figure 2). At the same time, a small hematoma enveloping the left iliac-femoral passage was present (Figure 1).
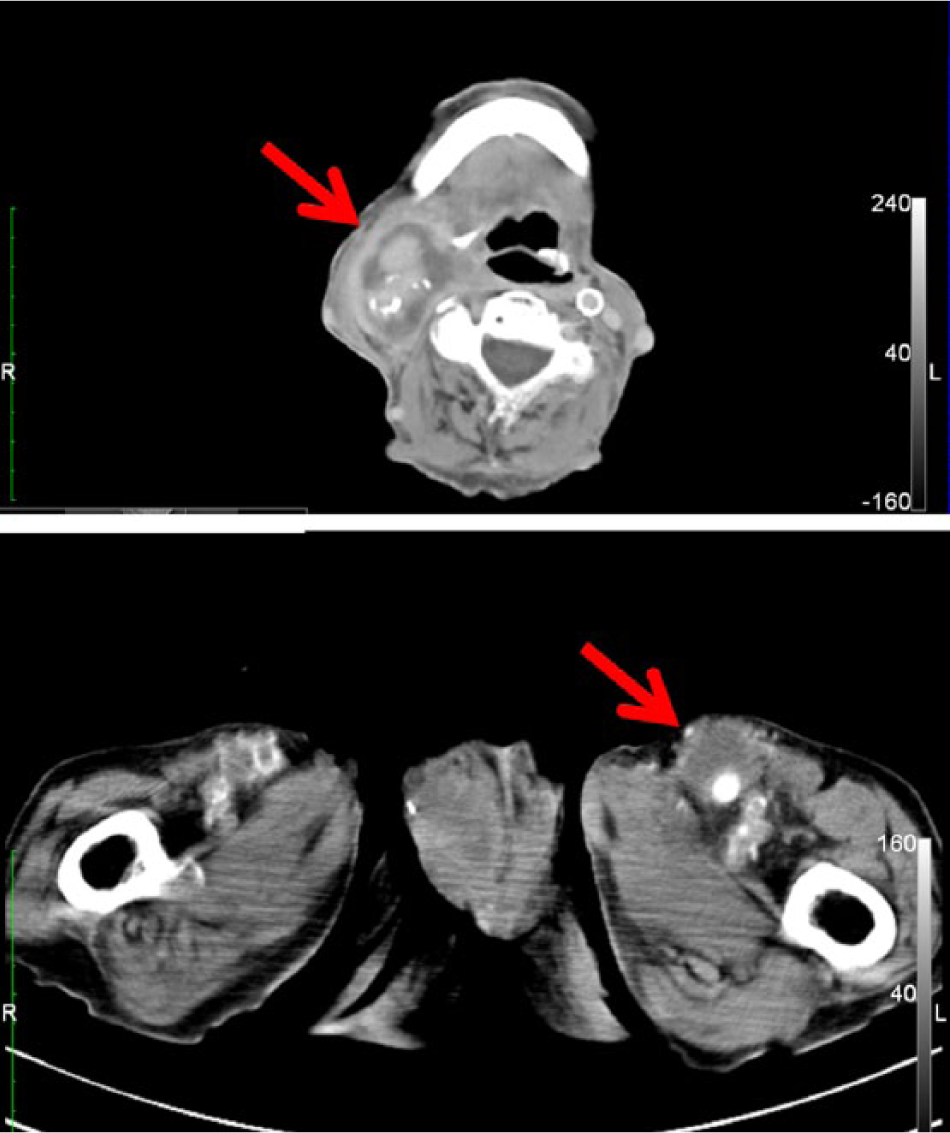
Angio-CT showing the hypodense bulk at the right common carotid artery and at the bifurcation, dislocating the right internal jugular vein and invading the nearby parapharyngeal space (upper part) and the small hematoma enveloping the left iliac-femoral passage (lower part).

The pseudoaneurysm at duplex ultrasound examination. Red arrow indicates the pseudoaneurysm surrounding the true lumen (yellow arrow).
The patient was then immediately re-referred to IRCCS Policlinico’s Operative Unit of Vascular Surgery. Upon admission, the patient had no fever. He was still taking Teicoplanin 200 mg twice daily. Blood tests showed an INR value of 5.5 in the absence of any anticoagulant or antiplatelet drugs. In addition, there was leukocytosis (14700/uL) and anemia (hemoglobin 10.4 g/dL). Clinical examination revealed a huge palpable tender pulsatile mass in the right neck and a smaller one in the left groin.
A trans-thoracic color-Doppler echocardiography was performed, excluding any valvular source of septic embolism. A normal preoperative heart ejection fraction (68.1%) was assessed.
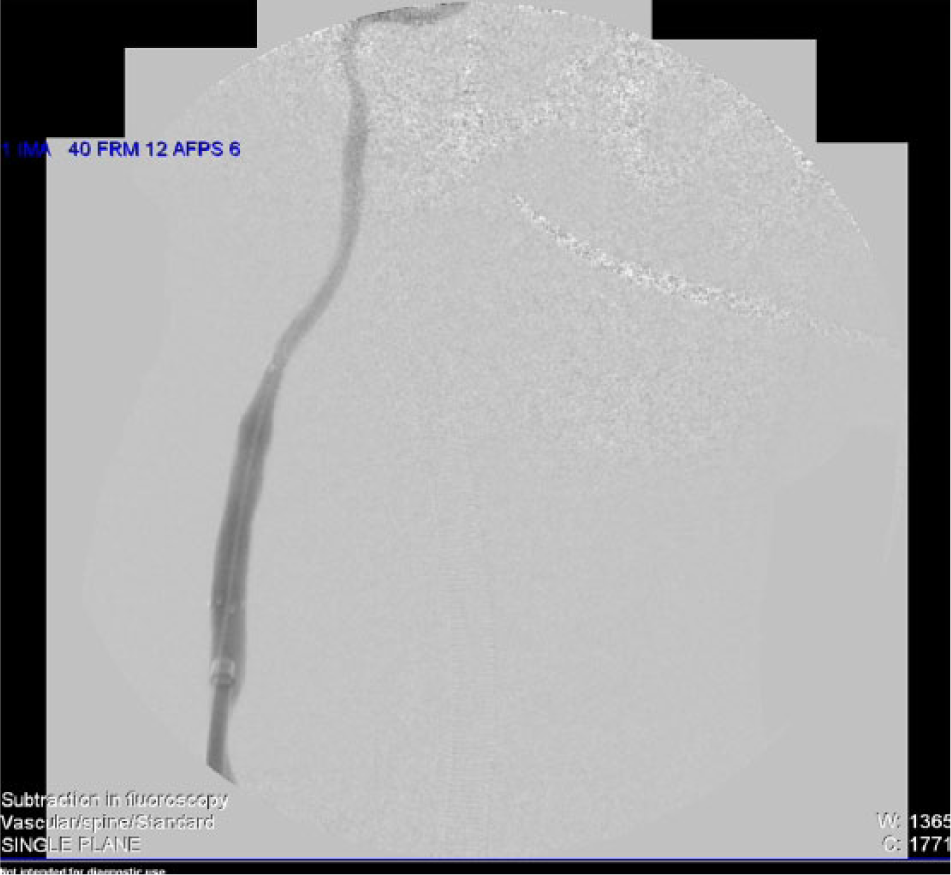
The patient was then referred to the operating room. Under general anesthesia, the right common femoral artery was isolated through a longitudinal cut-down in the groin. A selective right internal carotid angiography was performed using a 5F sheath and a 5F diagnostic catheter, confirming the presence of the voluminous pseudoaneurysm arising from the carotid bifurcation and extending toward the nearby parapharyngeal space (Figure 3). The external carotid artery was not visible, but the superior thyroid artery was visible.

Selective right internal carotid angiography confirming the presence of the voluminous pseudoaneurysm arising from the carotid bifurcation and extending toward the nearby parapharyngeal space.
A 0.035-in hydrophilic stiff wire was placed into the ICA. The short 5F sheath was then exchanged with a long guiding 10F sheath, which allowed the placement and the deployment of a Fluency (Bard Incorporated, Karlsruhe, Germany) polytetrafluoroethylene (PTFE)-covered nitinol self-expanding stent (8 mm in diameter and 40 mm in length). The angiographic control showed the patency of the ICA with complete exclusion of the lesion and absence of any signs of endoleaks (Figure 4). During palpation, the mass was no more pulsatile. Thus, a surgical right laterocervical incision was performed. The hematoma was evacuated and a PTFE graft was wrapped around the carotid wall where the covered stent had been placed. The incision was then copiously irrigated with saline solution and the wound was closed in layers. At the same time, the left femoral pseudoaneurysm was excised using a surgical approach and then the vessel wall was reconstructed using a small pericardial patch. At the end of the operation, the patient was admitted to the intensive care unit for 24 h and was then returned to the ward.
Angiographic control after placement of the covered stent, showing the patency of the internal carotid artery with complete exclusion of the lesion and absence of any signs of endoleaks.
Culture samples of the laterocervical mass and of the left femoral pseudoaneurysm were performed, both showing the presence of MRSA. Postoperative blood samples were negative, but a urine culture revealed the presence of extended-spectrum beta-lactamase-producing (ESBL) Escherichia coli. Antibiotic therapy with Ceftriaxone 2 g twice daily was added to the ongoing Teicoplanin. The dual therapy was continued with for 4 weeks since the two strains of microorganisms were sensitive to both antibiotics.
Postoperative course was uneventful, the laterocervical wound and both groin wounds healed completely with no signs of infection recurrence. The patient was then discharged on POD 15th on a dosage of acetyl salicylic acid 100 mg daily and low-molecular-weight heparin for his atrial fibrillation. He went back to the clinic where he was previously hospitalized for further rehabilitation. At discharge, an angio-CT scan of the neck showed the regular patency of the covered stent and of both common and ICA, without any signs of endoleaks (Figure 5). At duplex ultrasound, no flow impairment was observed through the carotid vessels.

Angio-CT scan of the neck at discharge, showing the regular patency of the covered stent and of both common and internal carotid artery, without any signs of endoleaks.
At 7 months follow-up, the patient was in poor general condition, but the laterocervical and inguinal wounds had no signs of infection and healed well, and the stent was still patent. The case report described in this article was approved by the institutional review board of our institution. The patient provided full informed consent to report the case for publication in an international medical journal.
Discussion
Mycotic pseudoaneurysms of the extracranial ICA are rare occurrences, being reported in less than 5% of all cases of arterial pseudoaneurysms. 4 They have been reported to be consequent to traumatic 5 or iatrogenic injuries or more frequently following systemic infective processes. 6 Systemic diseases which lead to the degeneration or malfunction of proteins of the arterial wall have also been advocated in the pathogenesis of mycotic pseudoaneurysms. 7 In about a quarter of cases, the etiology of the pseudoaneurysm remains unknown. 4
In the presented case, the carotid pseudoaneurysm was likely caused by the systemic spread of MRSA from the wound infection that the patient had during his first hospitalization. Despite appropriate systemic antibiotic therapy and removal of the infected graft with thigh amputation for irreversible ischemia, the patient’s poor medical condition favored the diffusion of the microorganism to other sites. The patient’s blood cultures were always negative, but it is possible that these results were distorted by the prolonged antibiotic therapy.
Treatment of such a lesion is necessary due to the high risk of rupture and distal infective brain embolization. 2 However, it often represents a challenge, being associated with a high morbidity and mortality 1 and given the need to manage an infective field in a delicate anatomical region. Systemic antibiotics associated with traditional open surgical approach are the treatment of choice.
Antibiogram-guided therapy is often recommended for at least 6 weeks, 8 but it should be always associated with surgical management of the lesions, as antibiotics alone may be unsuccessful. 9
Usually surgical strategies include arterial ligation, debridement of surrounding tissues, and in situ or extra-anatomical revascularization with an autologous vein interposition graft whenever feasible. 2 Ligation of the ICA alone is nowadays considered only in case of impossible carotid reconstruction or when the contralateral carotid flow through the Circle of Willis has proven to be valid. Otherwise, it is associated with a high incidence of neurological complications and death. 10
The surgical access to the site may be somewhat challenging due to the presence of intensive inflammation. Infective hematomas may in fact create adherence with the surrounding tissue with possible involvement of noble structures such as the hypoglossal or the vagus nerves, consequently carrying the risk of cranial nerve injury. 6
The use of endovascular techniques can be an appealing alternative in high prohibitive risk patients or in cases of a demanding surgical approach. 3 It offers a less invasive way to exclude the risk of both arterial rupture and distal infective embolization. Moreover, it allows the preservation of the antegrade carotid flow together with the achieving of an immediate bleeding control.
The range of endovascular options includes the use of both covered and uncovered stent-grafts, alone or in combination with coil embolization of the sac, which can successfully treat posttraumatic and postoperative carotid pseudoaneurysms. 11 The literature, however, still lacks reports about the use of endovascular techniques in primary mycotic carotid pseudoaneurysms. Concerns may be raised about the presence of heterologous prosthetic material in an infective field. A second issue is related to the possible distal embolization when crossing the pseudoaneurysm with the guidewire. Endovascular procedures are not free from complication, as stents and coils may migrate causing distal embolization and stents may occlude.
More frequently, the endovascular treatment represents the first part of a two-stage hybrid procedure, allowing initial control of bleeding for a safe secondary surgical definitive solution, as reported by Wales et al. 6 in 2009.
In our case too, the endovascular placement of a covered stent was the first step of a hybrid procedure. However, given the patient’s poor clinical condition, the extent of the pseudoaneurysm and the lack of autologous available venous tissue, we were not able to perform a complete reconstruction of carotid vessels, and we selected a second-step less invasive surgical approach with evacuation of the hematoma, debridement of surrounding tissue and reinforcement of the arterial wall with a PTFE wrap. Differently from Wales et al., 6 we decided to perform the surgical procedure at the same time as the endovascular procedure in order to minimize the risk of possible infection of the stent graft.
Even if there is no scientific evidence for PTFE wrapping as reinforcement, this technique was already tried by Kubo et al. 12 who combined wrapping with PTFE and clip occlusion for the treatment of a ruptured blister-like aneurysm of the ICA. It is certainly not possible to generalize this kind of approach for all patients with a carotid pseudoaneurysm, and the excision of the lesion associated with revascularization using autologous graft is still the treatment of choice. However, when the surgical approach is demanding or the patient’s condition is poor, the endovascular way may offer a safe alternative solution.
Conclusion
Mycotic pseudoaneurysms of the extracranial ICA are rare, and they are challenging to manage. Systemic antibiotics associated with the traditional open surgical approach are the treatment of choice; however, endovascular placement of a covered stent followed by laterocervical exploration with evacuation of the hematoma, debridement of surrounding tissue, and reinforcement of the arterial wall using a PTFE wrap has proven to be a safe alternative in a patient with a poor medical condition and the absence of available autologous veins.
Footnotes
Declaration of conflicting interests
The authors declare no conflict of interest in preparing this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.