
Abstract
Objective:
This study aimed to determine the association between adolescent socioeconomic status (father’s education and adolescent subjective socioeconomic status) and adult quality of life and the mediation roles of adult socioeconomic status, social capital and lifestyle (physical activity and exposure to smoke) among the “Tehran University of Medical Sciences Employees Cohort (TEC) Study” participants.
Method:
Data of 4455 participants were derived from the Tehran University of Medical Sciences Employees Cohort (TEC) Study. In this study, the World Health Organization quality of life-BREF, the World Bank’s Integrated and the International Physical Activity Questionnaire were used. Data were analyzed with structural equation modeling using SPSS Amos 24.0 program.
Results:
The mean age of the participants was 42.31 years (SD: 8.37) and most of the subjects were female (60.7%). Correlation analysis results revealed that, quality of life had a significant and positive association with adolescent subjective socioeconomic status (r = 0.169, p < 0.01) and father’s education (r = 0.091, p < 0.01). A mediation model testing the direct relationship between adolescent socioeconomic status and adult socioeconomic status and quality of life, showed a positive relationship between adolescent subjective socioeconomic status (β = 0.229, p < 0.001) and father’s education (β = 0.443, p < 0.001) with adult socioeconomic status. Adult socioeconomic status was positively related to quality of life (β = 0.205, p < 0.001). Adult socioeconomic status mediated the relationship between adolescent subjective socioeconomic status (β = 0.047, p < 0.01) and father’s education (β = 0.091, p < 0.01) with quality of life. While adult socioeconomic status fully mediated the relationship between the father’s education and quality of life, it partially mediated the adolescent subjective socioeconomic status-quality of life association. Other variables such as social capital and lifestyle did not have mediator role in a mediation model.
Conclusion:
This study provides the evidence for the role of adult socioeconomic status as a partial mediator between adolescent subjective socioeconomic status and quality of life. Therefore, there are several unknown mediators other than adult socioeconomic status that need to be explored in future studies.
Introduction
The concept of quality of life (QOL) is a multidimensional and subjective concept which generally includes both positive and negative aspects of life. 1 The World Health Organization (WHO) defines QOL as “individuals’ perceptions of their position in life in the context of culture and value systems in which they live, and in relation to their goals, expectations, standards, and concerns.” In fact, QOL is considered a subjective issue which cannot be evaluated by others and is based on people’s understanding of different aspects of life. 2 Health is a consistent determinant of QOL. Health related quality of life (HRQOL) is a subset of overall QOL, and it encompasses domains of mental, emotional, social, and physical health. It is a reflection of an individual’s mental status and reaction to disease. Self-rated health (SRH) is one way of measuring HRQOL. HRQOL systematically evaluates the association between health status and QOL; furthermore, it is regarded as an important indicator of health outcomes.3,4
Various factors influence QOL. Socioeconomic status (SES) is considered an important determinant of QOL. 5 SES refers to a person’s access to financial, social, cultural assets and human capital. 6 Studies indicate that SES is the most important determinant of QOL.7,8 Nutakor et al. 9 show that SES is a significant predictor of QOL. Abdollahpour et al. 10 showed that, among other factors, high SES consistently is the strongest predictor of SRH, promoting economic development can have profound effects on the health of the adult population, especially, improvement in adult SES versus adolescent SES further promotes SRH. Nouraei Motlagh et al. 11 also, found strikingly similar results. The results of this study showed that, among other factors, SES (41.2%) was the most important factors associated with the concentration of poor SRH in the poor groups.
Parental SES is defined as the relative social position of an individual or family, which influences their access to financial, social, cultural and human capital resources, and includes the parents’ educational status, occupation and income.12,13 For adolescents, subjective social class (economic well-being) or one of the parents’ three variables of educational status, occupation and income is frequently used to measure their SES.9,12,8,14 Of these three commonly used SES indicators, income may additionally mirror one’s degree of SES better than the other measures, as income is determined by occupation, which is in turn, usually, determined by educational attainment. Adolescents may not provide accurate information concerning parental SES (parental occupation and income). 13
Therefore, some studies have elected to use adolescents’ subjective social status to measure SES and have focused on the psychological effects of SES on adolescents. Adolescent-reported subjective SES (e.g., social status) is commonly more consistent with parent-reported SES than adolescent-reported objective SES (e.g., parental education and income). This is because subjective SES measures are extra age-appropriate for adolescents. 15
According to literature, adolescent SES significantly impacts health, education, income and job from adolescent to adult. 16 SES indicators can affect different aspects of people’s QOL directly and indirectly, especially during adolescence.17 –21 The adolescent subjective socioeconomic status (SSS) refers to an individual’s perception of his/her (or his/her family’s) SES in comparison to other members of society. 22 In contrast, Objective SES is the economic and social position of individuals in relation to others, and it is widely assessed by utilizing three indicators: income, education, and occupation. In line with other studies in Iran,23,24 education and wealth index were used to measure SES.
However, the indirect communication paths between adolescent SES and adult QOL have not been completely determined yet. Social capital is one of the most important QOL-related psychological factors.
Social capital refers to the set of norms in social systems that provide the possibility of people’s participation in social actions to gain mutual benefit. 25 The World Bank defines social capital as the hidden wealth of a society and defines it as “the institutions, relationships, and norms that shape the quality and quantity of a society’s social interactions.” 26 There are several definitions and measures for recognizing social capital, introduced by Asadullah et al., 27 in which the average response to the trust question is acknowledged as the standard measure for social capital that it is an essential element in the formation of social bonds and relationships. Social capital in traditional societies almost includes bonding aspect with specific social trust, and in modern societies is mostly a bridging aspect with generalized social trust. 28 The cultural context of Iran, is socially unbalanced that create a mixture of traditional and modern social capital. Thus, in this study, social capital is defined as “a network of relationship and links based on interpersonal and intergroup trust and the interactions of individuals with groups, organizations, and social institutions.” 29
According to the results of similar studies, increasing social capital improves QOL 30 and social capital acts as a mediator between SES and QOL. The results of this study showed social capital to be a significant mechanism by which adults’ SES influences their QOL, and crucial to invest in social infrastructure, encourage social cohesiveness, and decrease social inequities due to the significance of social capital in the connection between SES and QOL. 9 In the public health field, Kawachi et al. 31 proposed that social capital mediates the relationship between SES and health.
In addition, it has been discovered that a person’s SES situation has an effect on their health and QOL, directly32 –36 and indirectly through psychosocial factors such as the failure of the poor to form ties and networks for their own benefit.32,34,37 However, these psychosocial characteristics have the potential to operate as protective mechanisms, which can help mitigate some of the negative consequences that SES disparities have on QOL. Also, according to literature, SES is a strong predictor of social capital and QOL and social capital acts as a mediator in relationship between SES and QOL. 9
Lifestyle is one of the other influencing factors on the QOL. Wang and Geng, 38 in a cross-sectional study in China on 986 people, has shown that lifestyle plays the role of a mediator in the relationship between SES and mental health and physical health. Rohrer et al., 39 in a cross-sectional study in Texas on 170,000 people, showed that good mental health was independently associated with physical activity and poor mental health was associated with daily smoking. In contrast, health-promoting behaviors, such as physical activity, have been recommended to treat depression. In fact, the QOL can be improved with regular exercise and not smoking. 40
Therefore, it seems that QOL is influenced by many factors such as adolescent SES, adult SES, lifestyle (physical activity and exposure to smoke) and social capital. Moreover, it seems that adult SES plays both mediator and independent roles in this study. Because, statistically and theoretically, there is a strong relationship between SES (adolescent SES and adult SES) and social capital. Also, the results of earlier studies have shown SES (adolescent SES and adult SES) to be a strong predictor of QOL and social capital, the latter of which is a significant mechanism by which adults’ SES influences their QOL.9,8,14,41,42 So in the relationship between adolescent SES and QOL, adult SES can have played roles as a mediator in the relationship between adolescent SES and QOL, and as an independent variable in the relationship between SES and social capital and QOL. To identify the roles of adult SES as a mediator and independent variable, structural equations modeling is a suitable approach. Oshio et al., 43 in a cross-sectional study in Japan on 3292 people, has shown that adult SES plays both mediator and independent roles simultaneously.
As a result, it is possible to present a model in which the hypothetical adult SES, social capital and lifestyle (physical activity and exposure to smoke) play a mediating role in the relationship between adolescent SES and QOL. Therefore, it is important to determine the contribution of these variables and the indirect effects of adolescent SES on QOL.
In this study, we aimed to provide insight into the associations between adolescent SES (adolescent SSS and father’s education) and adult QOL. Therefore, we hypothesized that adult SES, social capital and lifestyle (physical activity and exposure to smoke) might play mediating roles in the associations between adolescent SES and adult QOL.
Methodological strategy
Study area and population
In this cross-sectional study, we used data from the enrolment phase of the TEC study. The TEC study was designed to investigate common non-communicable diseases and factors affecting health among the employees of Tehran University of Medical Sciences in 2018. 44 The first phase (cross-sectional study) of this study was the enrolment phase from January 2018 to March 2021. Tehran University of Medical Sciences (TUMS) is the oldest and most well-known medical center in Iran with approximately 19,000 employees, nationally as well as internationally. 45 In Cohort (TEC) study, all questionnaires were completed for all subjects by trained interviewers, therefore, we did not have a selection bias for literary. Data of 4455 people were applied in the analysis of this study. In this study, authors have followed the STROBE Guidelines when preparing the manuscript.
Inclusion and exclusion criteria:
Any kind of employment status within TUMS and its affiliated centers, and consent to participate in the study are the inclusion criteria. There are no exclusion criteria.
Data collection tool
WHO QOL questionnaire
The World Health Organization quality of life (WHOQOL-BREF) questionnaire that contains 26 items and evaluates 4 QOL domains: physical (7 items), mental (6 items), social (3 items) and environmental health (8 items). Two other items measure overall QOL and general health. The validity and reliability of this questionnaire have already been evaluated in national studies and have found to be acceptable. 46
Measuring adolescent SES
It comprised adolescent SSS and father education level. In Iran, the head of the household is the father, and the economic status of the family has most correlation with the father’s education. 47
To measure adolescent SSS, the following question was included: “If SES was divided into five categories, what would your status be when you were 18 years old?” The participants were asked to answer the abovementioned question by choosing one of the following options: “low, moderate to low, moderate, moderate to high and high status.” Various studies have used this index to measure adolescent SES, as it has acceptable validity and reliability.17,48 The adolescent SSS of the participants was assessed using the MacArthur scale which was converted to a five-point Likert scale.49,50
Father’s education was divided into seven categories (illiterate, primary, secondary, diploma, bachelor’s, master’s, and PhD levels).
Measuring the adult SES
Individuals’ education, assets and social activities 51 have been evaluated to measure their adult SES. The education levels of the respondents have been classified into illiterate, primary, secondary, diploma, bachelor’s, master’s, and PhD levels. Questions have been asked about household assets such as, owning a car, a dishwasher, a microwave, a personal computer, a washing machine, a TV, the number of rooms in the house, the area of the house, number of times going to a theater, cinema and/or concert, the number of times a person eats at a restaurant at one’s own expense, number of times traveling by plane, having internet access at home and its average monthly costs. In this study, household assets were combined using principal component analysis (PCA) and the first factor was considered as the SES of the asset.
Given the lack of a standard occupational classification system in Iran and the fact that there are people ranging from very rich to very poor in a single occupation class in available systems, occupation status, was not evaluated as a proxy of SES.
Social capital questionnaire
The World Bank Social Capital Questionnaire was designed to examine social capital among families in developing countries. This questionnaire included 27 main questions and 6 domains as follows: Membership in associations and groups (3 questions), the social trust rate (11 questions), contribution in team works and public activities (3 questions), information and communication (2 questions), social cohesion (10 questions) and the political empowerment and activity (5 questions). 52 Social capital questions have been derived from the World Bank questionnaire for developing countries which has been evaluated as having good reliability and validity in Iran. 53
Measuring the lifestyle
It comprised International Physical Activity Questionnaire (IPAQ) and exposure to smoke questionnaire as follows;
International physical activity questionnaire
The summary of the IPAQ was used to measure physical activity. This questionnaire has been used to measure physical activity by the WHO and in various studies in the country, and its validity and reliability have been confirmed.54,55
Examining the exposure to cigarette smoke (tobacco hookah)
The tobacco, cigarette and hookah consumption per day, month, and year by the individual, spouse, other family members, and friends was assessed to measure exposure to cigarette smoke. The reliability and validity of this questionnaire is acceptable for the population of Iran. 56
Statistical analysis
There are various methods to identify the role and contribution of mediating variables. Due to the investigation of a wide range of associations with the aim of exploring different paths in this study, structural equation modeling (SEM) was used, which is the best approach for exploratory purposes in cross-sectional studies, also in regression, each variable can only have one role. But in reality, a variable can play the role of independent, mediator and dependent variable at the same time, so to solve this problem, structural equations are a suitable approach. 57
To assess the correlations between the research variables, the Pearson correlation analysis was used. Maximum likelihood (ML) SEM based on the multivariate normality of observable variables and their significance was assessed using a 95% bootstrap confidence interval with 2000 samples replications. The current study followed the two-steps approach suggested by Hayes 58 to investigate the research multiple mediation model. First, the direct association between adolescent SSS and father’s education with adult QOL without including mediators were tested (total effect model). Second, the mediators (i.e., adult SES, social capital, physical activity, and exposure to smoke) were added to the model to develop a serial multiple mediation model (mediation effect model). Bootstrapping is more accurate and has higher statistical power than Baron and Kenny 59 and Sobel 60 approaches. Cat PCA was used to calculate the score of the adult SES indicators. All data analysis was performed using IBM SPSS Amos version 24.0.
Results
Table 1 presents the demographic characteristics of participants in the study. The mean age (range: 19–74 years) of the participants was 42.31 years, (SD: 8.37). Most of the subjects were female 60.7% (2703 people). Among the participants, 40.2% (1789 people) had a bachelor’s degree education and 79.1 (3524 people) were married. Other descriptive statistics are presented in Table1.
Demographic characteristics of participants.

Table 2 shows the results of conducting Pearson correlation analysis. Correlation analysis result revealed that adult QOL had a significant and positive association with adolescent SSS (r = 0.169, p < 0.01) and father’s education (r = 0.091, p < 0.01). In addition, adult QOL had a significant and positive association with physical activity, social capital, assets, social activity and education, ranging from small to moderate effect sizes (r range = 0.048–0.21). Also, social capital and physical activity had a significant and positive association with assets, social activity, father’s education, adolescent SSS and education in ranging from small to moderate effect sizes (r range = 0.048–0.21). Exposure to smoke had a significant and negative association with assets, social activity, father’s education, education and physical activity with exposure to smoke in ranging from small to moderate effect sizes (r range = −0.048 to −0.28). Moreover, asset was largely and positively correlated with social capital (r = 0.55, p < 0.001) and education (r = 0.50, p < 0.001), as shown in Table 2.
Correlation analysis results.
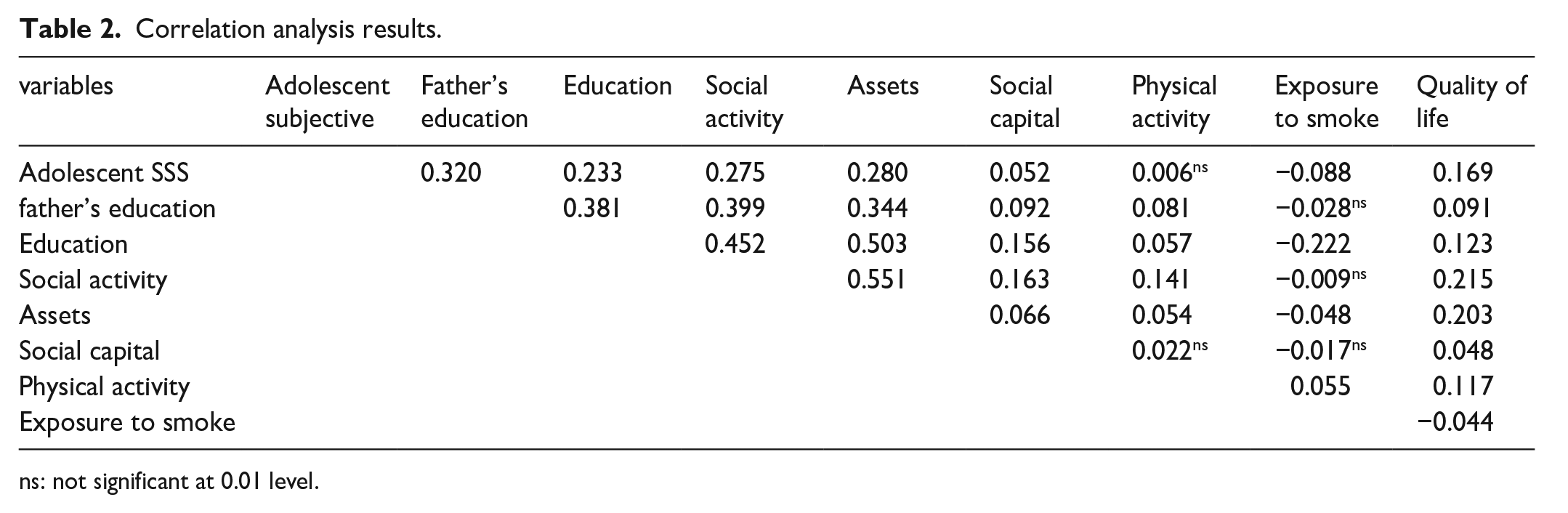
ns: not significant at 0.01 level.
The fit of the structural model using ML was determined based on GFI (93.98%), AGFI (92.11%), CFI (91.14%), and NFI (91.21%) indices. The reported results regarding the estimated indexes indicated the appropriate fit of the model, and all the fit indices obtained from the SEM analysis fell within an acceptable range. Therefore, the structure of the hypothetical research model was confirmed.
Standardized path coefficients of mediation effects models are shown in Figure 1 and reported in Tables 3 and 4 as well. As shown in Figure 1, in the measurement model, social activity (r = 0.74) had the greatest effect on the latent variable of adult SES, and assets (0.72) and education (0.66) were ranked second and third in this regard. In other words, social activity index explaining 0.55 of SES variance. In addition, the variable of mental health (r = 0.84) had the greatest effect on the latent variable of adult QOL, and overall health (0.67) and physical health (0.65) were ranked second and third, respectively. Mental health explaining 0.70 of adult QOL variance.

A final mediation analysis model of the association between adolescent SSS and father’s education with QOL through mediators in TUMS employee’s Cohort study (n = 4455) using ML SEM. Standardized coefficients for measurement and structural models presented on lines.
Assessment of the direct effects of model parameters.

Direct effect = the pathway from the adolescenthood SES and father’s education to the QOL while controlling for the mediators.
Non significant: p > 0.05.
Assessment of the indirect and total effects and 95% bootstrap confidence intervals of model parameters.

Number of bootstrap samples for percentile bootstrap confidence intervals: 2000.
Indirect or mediated effect: the pathway from the adolescenthood SES and father’s education to the QOL through the mediators. Total effect: direct effect + indirect effect.
Significant: p < 0.05.
The results of testing the direct association of the mediation model are shown in Table 3. All direct correlations were significant except for the correlation between adolescent (SSS) with social capital and physical activity, and the correlation between father’s education with social capital and exposure to smoke. The reported results show that the effect of all variables was positive, while the effects of exposure to smoke on QOL and adolescent SSS on social capital, physical activity and exposure to smoke was negative. Additionally, the correlation between father’s education and QOL was negative and did not allow the model to fit. Therefore, the correlation between father’s education and QOL was illogical and was not included in the model.
The results of this model show that the greatest effect was the correlation between father’s education and the adult SES (B = 0.44, 95% CI = 0.41, 0.47). Thus, increasing the father’s education score by one unit increases the adult SES by 0.44.
The results of assessing the indirect and total effects model are shown in Table 4. The results show that, the indirect path between adolescent SSS and adult QOL through adult SES (B = 0.047, 95% CI = 0.035, 0.058) was significant. Whereas, the indirect path between adolescent SSS and adult QOL through social capital (B = 0.000, 95% CI = −0.001, 0.000), exposure to smoke (B = 0.001, 95% CI = 0.000, 0.007) and physical activity (B = −0.002, 95% CI = −0.006, 0.001) were not significant. Moreover, the indirect path between adolescent SSS and adult QOL sequentially through adult SES and social capital (B = 0.001, 95% CI = −0.001, 0.004) was not significant.
The indirect path between father’s education and adult QOL through adult SES (B = 0.090, 95% CI = 0.071, 0.110) and physical activity (B = 0.01, 95% CI = 0.005, 0.015) was significant. However, the indirect path between father’s education and adult QOL through social capital (B = 0.000, 95% CI = −0.001, 0.001), exposure to smoke (B = 0.000, 95% CI = −0.001, 0.001) and consecutively through adult SES and social capital (B = 0.003, 95% CI = −0.0006, 0.006) were not significant. Also, the results of assessing the total effect model showed a significant association between adolescent SSS (B = 0.168, 95% CI = 0.132, 0.202) father’s education (B = 0.105, 95% CI = 0.087, 0.124), and adult SES (B = 0.212, 95% CI = 0.173, 0.254) with adult QOL.
The contribution of mediators is shown in Table 5. In the correlation between adolescent SSS and adult QOL, only the adult SES played a mediating role, and the contribution of this mediator was reported at 28.57%. Furthermore, in the correlation between father’s education and adult QOL, adult SES played a mediating role (88%). More specifically, while adult SES fully mediated the relationship between father’s education and QOL, that partially mediated the adolescent SSS—adult QOL link.
Mediation percentages of model’s parameters.
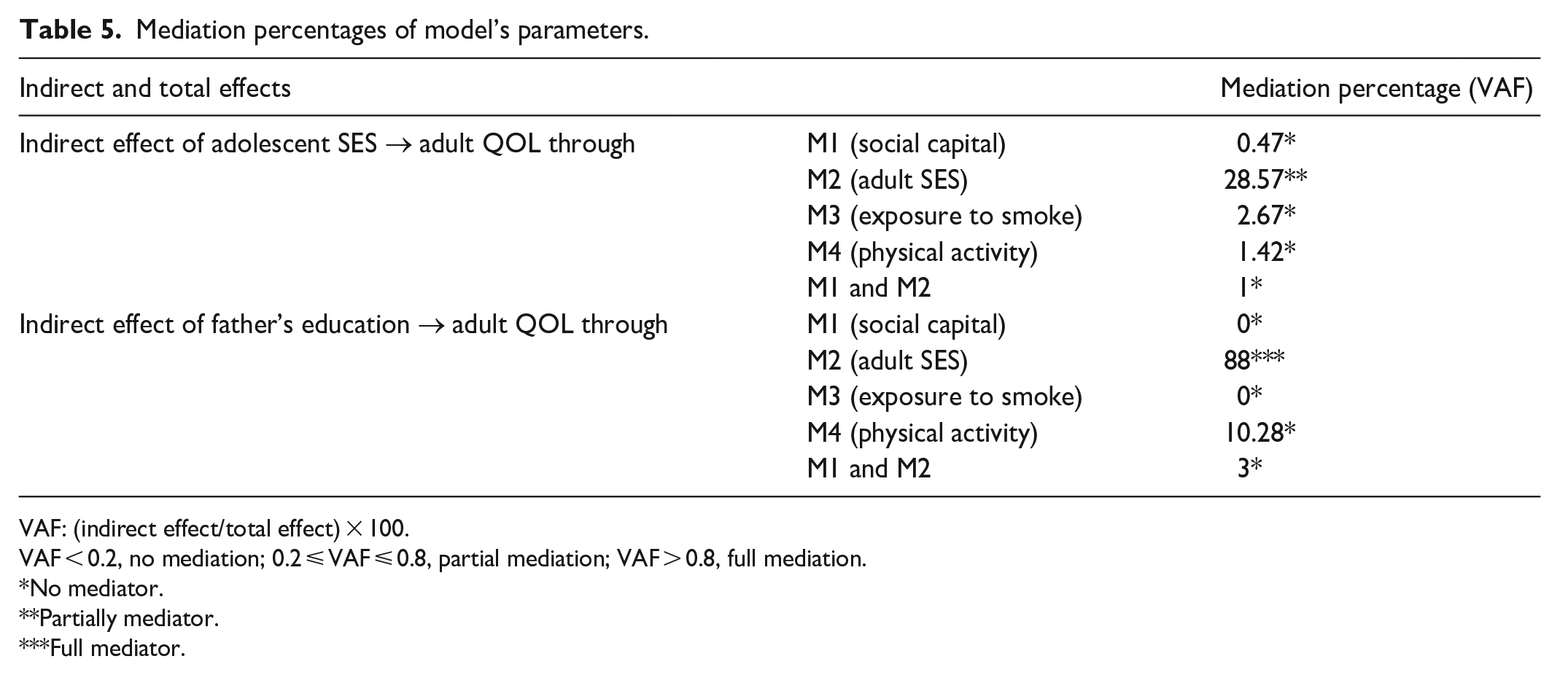
VAF: (indirect effect/total effect) × 100.
VAF < 0.2, no mediation; 0.2 ⩽ VAF ⩽ 0.8, partial mediation; VAF > 0.8, full mediation.
No mediator.
Partially mediator.
Full mediator.
Discussion
The main purpose of this study was to determine the contribution and role of mediators in the correlation between adolescent SES and adult QOL. We selected an adult SES, social capital, exposure to smoke and physical activity as potential mediators, all of which were theoretically plausible shown to be associated with adolescent SES and adult QOL. In this study, all direct correlations except the correlation between adolescent SSS with social capital and physical activity and the correlation between father’s education with social capital and exposure to smoke were significant.
Moreover, the indirect paths between adolescent SSS and adult QOL through adult SES and the association between father’s education and adult QOL through adult SES and physical activity were significant. The total effects in the correlations between adolescent SSS and father’s education with adult QOL were significant.
The results show that adolescent SSS had the strongest association with adult SES and adult QOL. Our mediation analysis show that only adult SES was significant partial mediator in correlation between adolescent SSS and adult QOL and full mediator in correlation between father’s education with adult QOL in our sample, suggesting this variable has the most robust effects. Mediation analysis confirmed mediating effects of adult SES through the following results: (1) adolescent SSS was significantly associated with adult QOL; (2) Adolescent SES had significant positive associations with the adult SES; and (3) when adult SES was added to the models as mediators, the strength of association between adolescent SSS and adult QOL were reduced, and the association between father’s education and adult QOL was not significant. So, according to the direct, indirect and total effect, correlations between adolescent SSS and father’s education with adult QOL through adult SES was confirmed and adult SES significantly contributed to the correlation between father’s education and adult QOL. Lower adolescent SES was associated with worse adult QOL. Part of the effect of adolescent SSS on adult QOL was through adult SES and all of the effect of father’s education on adult QOL was through adult SES. Both adolescent SES and adult SES are important for adult QOL. The negative impact of low adolescent SES can be partially ameliorated if people from a low SES position during adolescent mobilize to higher status in adult.
This result is consistent with that of Lee’s study that investigated the correlation between adolescent SES and QOL in the elderly. According to the results of this study, adolescent SES has a direct effect on QOL in old age, and as the adult SES improves, QOL in old age improves too, thus, the adult SES acts as a mediator in the correlation between adolescent SES and QOL in old age. 17 Also, our finding is consistent with some studies,20,43,61 –63 that adult SES had a significant mediating effect on the correlation between adolescent SES and adult QOL. All the aforementioned studies have confirmed the mediating role of the adult SES.
The second hypothesis, “The correlation between adolescent SSS and father’s education with adult QOL through social capital” was not confirmed, through the following result: (1) adolescent SSS was significantly associated with adult QOL; (2) Adolescent SES had not significant associations with the social capital; and (3) when social capital was added to the models as mediators, the strength of association between adolescent SES and adult QOL were not changed. So, according to the direct, indirect and total effect, correlations between adolescent SSS and father’s education with adult QOL through social capital was not confirmed.
Our result is consistent with the results of Li et al. 64 who investigated the mediating role of social capital in the correlation between poverty and mental health in children, where it was not confirmed. Also, our finding is not consistent with the results of some studies.20,43,62,63,65,66 that social capital had a significant mediating effect on the correlation between adolescent SES and adult QOL.
All these studies have confirmed the mediating role of social capital. These inconsistencies can be due to the difference in target populations and the employment of other analysis methods in estimating the mediators. This finding implies that social capital may not always serve as a mediator between adolescent SES and adult QOL and that other factors may be at play. The relationship between adolescent SES and adult QOL is complex and multifaceted.
The third hypothesis, “The correlation between adolescent SSS and father’s education with QOL through lifestyle (exposure to smoke and physical activity)” was not confirmed, through the following result: (1) adolescent SSS was significantly associated with adult QOL; (2) adolescent SSS had not significant associations with the physical activity and father’s education with the exposure to smoke; and (3) when exposure to smoke was added to the models as mediators, the strength of association between adolescent SSS and adult QOL were not changed, but when physical activity was added to the models as mediators, the strength of association between father’s education and adult QOL were reduced a little. So, according to the direct, indirect and total effect, correlations between adolescent SSS and father’s education with adult QOL through exposure to smoke was not confirmed and the mediating effects of physical activity were relatively limited, although statistically significant. Our result show that the strength of association between father’s education and adult QOL were not attenuated substantially even after controlling for physical activity.
This result is not consistent with the results of Umeda’s study, 21 which showed that adolescent poverty has a significant effect on smoking and physical inactivity and the results of Rohrer and Wang’s research,38,39 which showed that smoking and physical activity affect mental health. The reason for the inconsistency of these studies with our study can be the use of linear regression method instead of using SEM. This finding implies that life style may not always serve as a mediator between adolescent SES and adult QOL and that other factors may be at play.
The fourth hypothesis, “The correlation between adolescent SES and adult QOL sequentially through adult SES and social capital” was not confirmed. This result is not consistent with the Coleman’s social capital theory 37 and Kawachi proposed that social capital mediates the relationship between SES and health. 31
In this study, only adult SES was a significant partial and full mediator in the correlation between adolescent SSS with adult QOL, and father’s education with adult QOL, respectively. SES is mainly reflected in three aspects of an individual’s life: occupation, income, and education. All three aspects affect people’s physical and psychological state and cognition of the world around them.17,18 Having cognitive resources and knowledge about healthy behaviors and the skill to change one’s unhealthy behaviors are among factors that are effective in maintaining healthy behaviors and affect the probability of exposure to various disease risk factors. People with high levels of education are more likely to have stable careers and income, enabling them to invest in their health. Income determines people’s living and working environments and determines access to a variety of health products and services. Consequently, higher SES may be correlated with better physical health. Therefore, SES is the main factor affecting health inequality and SES inequality increases health inequality.
A higher SES usually translates into access to better healthcare, employment possibilities, and educational institutions, as well as extra profits and wealth. 54 Better living standards, including access to a clean and safe location to live, dependable transportation and other simple necessities are also related to better SES. 55 All of these elements may additionally lead to advanced physical and mental health results, greater social engagement and network involvement, and better tiers of personal contentment.
Therefore, the implementation of strategies that help improve SES can also improve QOL and health, such as, strengthening public health education, extensive health education programs, promoting healthy lifestyles, reducing inequality by reducing the unemployment rate and implementation of government support measures for poor families. Effective poverty alleviation policies would be helpful in improving the QOL and overall health.
Limitations
This study has several limitations. Causal inference should be done with caution since this research was a cross-sectional study and researchers were unable to determine causal associations and causal directions between variables, and they were unable to examine causal mediation in the mediation analysis process. In this study, only the consistency of the hypothetical mediation model with the data used was confirmed by the results. To overcome this limitation, prospective data must be used in determining the causality of the hypotheses. Moreover, due to the large number of participants, self-reported tools were used to assess the adolescent SSS of the TUMS employees, that it may not be possible to accurately assess adolescent SSS. Also, we may not be able to generalize the results to the entire Iranian population. Because the study population consisted of all TUMS employees, the results must be carefully generalized to the general population. However, the fact that the selected employees came from a variety of age groups and occupational backgrounds contributed to the diversity of their SES.
Conclusions
According to the results of this study, adult SES is a partial mediator in the association between adolescent SSS and adult QOL, also adult SES is a full mediator in the association between father's education and adult QOL. Therefore, in the association between adolescent SSS and adult QOL, there are a number of unknown factors other than adult SES that need to be investigated in future studies. Also, the findings of this study have substantial implications for public health policy and practice. Interventions aimed at minimizing health inequalities and improving health outcomes, especially among people with low SES, can improve QOL in adult life; therefore, policymakers and practitioners need to focus on reducing inequalities.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231220216 – Supplemental material for Does adult socioeconomic status mediate the relationship between adolescent socioeconomic status and adult quality of life?
Supplemental material, sj-docx-1-smo-10.1177_20503121231220216 for Does adult socioeconomic status mediate the relationship between adolescent socioeconomic status and adult quality of life? by Azam Biderafsh, Abbas Rahimi foroushani and Saharnaz Nedjat in SAGE Open Medicine
Supplemental Material
sj-pdf-2-smo-10.1177_20503121231220216 – Supplemental material for Does adult socioeconomic status mediate the relationship between adolescent socioeconomic status and adult quality of life?
Supplemental material, sj-pdf-2-smo-10.1177_20503121231220216 for Does adult socioeconomic status mediate the relationship between adolescent socioeconomic status and adult quality of life? by Azam Biderafsh, Abbas Rahimi foroushani and Saharnaz Nedjat in SAGE Open Medicine
Supplemental Material
sj-pdf-3-smo-10.1177_20503121231220216 – Supplemental material for Does adult socioeconomic status mediate the relationship between adolescent socioeconomic status and adult quality of life?
Supplemental material, sj-pdf-3-smo-10.1177_20503121231220216 for Does adult socioeconomic status mediate the relationship between adolescent socioeconomic status and adult quality of life? by Azam Biderafsh, Abbas Rahimi foroushani and Saharnaz Nedjat in SAGE Open Medicine
Footnotes
Acknowledgements
This work was adapted from a PhD thesis in Tehran University of Medical Sciences (TUMS). We are indebted to the participants of the TEC study for sharing their valuable time with the research team.
Author contributions
AB drafted the manuscript, contributed to the conception and computational framework, and performed the data analyses. AR designed the statistical model and the computational framework. SN conceived and presented the idea, designed the study, managed the data collection, and critically revised the data analysis and manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The datasets were derived from the TEC study. However, the datasets collected during the current study are available from the first author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tehran University of Medical Sciences, under Grant Agreement (IR.TUMS.MEDICINE.REC.1400.546).
Ethical approval informed consent for participation
Ethical approval for this study was obtained from the Ethics and Research Committee of Tehran University of Medical Sciences (IR.TUMS.MEDICINE.REC.1400.546). Written informed consent was obtained from all participants before participation. In Cohort (TEC) study, all questionnaires were completed for all subjects by trained interviewers, therefore, we did not have a selection bias for literary. A copy of the signed written informed consent form was handed over to each participant. The study was performed in accordance with the Declaration of Helsinki. Participants did not incur any cost by participating in this study and there was no financial inducement.
Written informed consent for publication
The participants gave their written informed consent to publish their data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.