
Abstract
Background:
Chronic kidney disease is on the rise globally and poses a significant public health concern. Patients with chronic kidney disease are receiving sustainable treatment through hemodialysis. However, hemodialysis is intensive, costly, and requires regular treatment. This study aims to explore the lived experiences of patients undergoing hemodialysis treatment.
Methods:
This study employed a phenomenological qualitative approach conducted between May and August 2023. Semi-structured, in-depth interviews were used with 16 participants selected purposively. Data were collected using an audio tape recorder and a notebook, and data collection ceased upon achieving thematic saturation. The data were analyzed using thematic analysis.
Results:
Seven themes were identified: (1) Threads of survival, (2) the price of survival, (3) the thirst of survival, (4) psychological and emotional distress, (5) physical effects, (6) social concerns, and (7) coping with treatment and the disease.
Conclusion:
Understanding the lived experiences of patients with end-stage renal disease and their coping mechanisms is crucial for healthcare providers in planning and delivering quality care, that is, centered on patient experiences. By focusing on what patients go through daily and how they manage their condition, healthcare providers can develop care plans that are not only effective but also empathetic and supportive. Expanding dialysis services, reducing costs, and emphasizing early chronic kidney disease detection and prevention are critical to reduce the burden.
Introduction
Chronic kidney disease (CKD) is a progressive decline in kidney function, indicated by an estimated glomerular filtration rate of <60 mL/min/1.73 m2 that persists for 3 months or longer. 1 If left untreated, CKD causes the kidneys not to work adequately and ultimately requires renal dialysis or kidney transplantation.1–3
CKD is a worldwide health problem.4,5 Globally, in 2017, it was predicted that 1.2 million people would die from chronic renal disease. 3 More than 70% of end-stage renal disease (ESRD) patients are projected to reside in low-income nations by the year 2030, particularly those in Sub-Saharan Africa. 2 In Tanzania, CKD is predicted to affect about 7%–15% of the adult population, with 15.2% of patients from urban and rural areas, which account 2%, making it a major public health concern. 6 Meanwhile, the number of people with CKD is increasing in the towns where awareness of prevention of non-communicable diseases is high compared to the rural areas. Furthermore, there is limited access to ESRD treatment, including dialysis and renal transplant, 7 where the centers of dialysis are very few, and most of them are located in urban areas in some of the regional referral hospitals and consultant hospitals, leaving patients in rural areas with low or no access. Limited access to dialysis centers puts patients and their families in a challenging dilemma, encompassing the costs of dialysis, travel, and temporary housing for those relocating from their homes – expenses that are unaffordable for many families. This restricted access also leads to poor health outcomes and, tragically, preventable deaths.
The most prevalent cause of CKD in the past was chronic glomerulonephritis, but to date, diabetes mellitus (DM) and hypertension are the major causes of ESRD, accounting for about 60% of the patients receiving hemodialysis (HD).2,3 To improve patient life expectancy and quality of life of patients with ESRD, HD, and/or kidney transplantation is important. However, the treatments are of high cost and limited access, specifically to low-income countries, including Tanzania.
In Tanzania, nearly three-quarters of the population lacks access to a health insurance fund. 8 Currently, only 15.3% of Tanzanians have any form of health insurance, while over 75% pay for healthcare out of pocket. 9 Progress in improving health insurance coverage has been slow; as of 2025, ~37% of Tanzanians are insured, up from 32% in 2023. 10 The government’s Universal Health Insurance Act (2023) aims to make coverage mandatory and to achieve 50% insurance coverage by 2030. Efforts to pass legislation for a mandatory nationwide scheme to include the large and diverse informal sector have not yet succeeded. However, in January 2026, the government announced a new initiative to provide health insurance for all citizens, proposing a minimum fee of 150,000.00 TZS for families of six members.
A kidney transplant is the recommended treatment for ESRD. However, due to the high costs and the fact that many patients are not covered by health insurance, along with the limited availability of donors, HD remains an alternative treatment for renal replacement therapy.1,11
HD is a medical procedure of purifying blood that removes toxins and excess fluid from the blood using an external device known as a dialyzer or artificial kidney.3,11–13 Depending on the patient’s health condition, treatments are typically scheduled three to four times a week, each lasting 3–4 h.12,14,15 To perform HD, vascular access is required, which can be established using one of three methods: an arteriovenous fistula, a vascular graft, or a vascular catheter.11,16 In addition, once vascular access is established, patients must take care to maintain this access and prevent infections during their treatments.
Patients undergoing HD must make significant lifestyle changes to maintain a satisfactory level of well-being. It is essential to adhere strictly to the treatment plan, which includes urgent dietary and hydration restrictions.16,17 However, these lifestyle changes cause a double burden on patients, including physical, psychological, emotional, and spiritual changes. To respond to these burdens, nurses and other healthcare providers need to understand what patients are going through daily. Health practitioners can provide adequate care and advance the standard of treatment through holistic care by learning about how patients who are reliant on HD for ESRD live their lives. 18
However, despite the improvement and increase in the healthcare facilities that provide HD, the mortality of patients dependent on HD is high. These have been a burden to the government of Tanzania and the community as a whole; hence, this treatment is expensive. Patients who depend on HD are not getting relief, and most of their lives are deteriorating instead of improving. Hence, morbidity and mortality for this patient are high. Due to this, there is a problem in following the restriction toward their disease condition, which therefore led to difficulties in their social, psychological, and financial on the start of dialysis. Therefore, we conducted a study to explore the lived experiences of patients undergoing HD treatment in Tanzania and their coping strategies.
Materials and methods
Study design
A qualitative descriptive design was employed to gather rich data about patients’ lived experiences on HD and their coping mechanisms. This design utilized a phenomenological approach alongside the constructivist method, enabling participants to share their daily lived experiences of HD. This was essential in developing and articulating the patient’s own experiences and concepts that are truthful, reflecting their reality as they determine the lived experiences of patients undergoing HD treatments.
Study setting
The study was conducted in the Dodoma Region, Tanzania. In the dialysis unit, which is found in Benjamin Mkapa Hospital (BMH). The hospital is located at the University of Dodoma. The BMH hospital was chosen as the study area because it has a HD unit which handles a high number of patients from Dodoma city and the surrounding regions, including Iringa, Morogoro, Singida, Manyara, and Tabora, among others.
Population
The study population included patients attending HD at BMH. These patients came from the neighboring regions such as Iringa, Singida, Kondoa, and Morogoro, among others. They included patients with acute renal failure as well as chronic renal failure. The majority of the patients have shifted from their homes and live in a nearby village, and wards to get dialysis in the BMH.
Inclusion and exclusion criteria
The inclusion criteria for the study participants were as follows: all patients who agreed to participate, free from hearing impairment, aged 18 years and above, received HD for at least 3 months or more, fluently spoke Swahili or English, were free from the influence of medications, especially sedative or hypnotics, or were critically ill. Meanwhile, patients who were seriously ill, unable to communicate, unable to be interviewed for 30 min, and those who did not consent to the study were excluded from the study.
Sampling technique and sample size
BMH was selected purposively because it is a large hospital in the city that serves a significant number of patients, with 45 individuals undergoing HD per day. Patients at BMH attend HD in two sessions, three times a week, from Monday to Saturday. Initially, 60 active patients were identified from the dialysis unit’s register book. Forty ESRD patients were purposively selected as study participants after meeting the inclusion criteria. However, the principle of saturation guided data collection, and after the 16th participant, when no new themes surfaced, recruitment was stopped (Jennings & Yeager, 2025). 19 As a result, the final sample consisted of 16 patients whose narratives were rich and detailed enough to meet the study’s goals.
Data collection tools and procedures
During data collection, an interview guide and a tape recorder were used. The researchers developed an interview guide after a thorough literature review, which guided the discussion, while probing questions proved useful depending on the participant’s explanations or details. The probing technique enabled the researcher to gather significant data. A tape recorder was used to record the discussion.
Data collection procedure
The interview took place in a separate and comfortable private room after the dialysis session. Data were gathered using a semi-structured questionnaire through in-depth face-to-face interviews until saturation was achieved, meaning no new information was obtained. The interview guide and probing questions were used to achieve rich and clear data. A pretest was conducted on 22% of patients in different settings to assess the tool’s validity. The interview was conducted by two research assistants: H.J.S., a male with a Bachelor of Science degree in Nursing, and A.T., a female with a Master of Science degree in Nursing. Both were students at the time of data collection and possessed experience in qualitative research. A professional rapport was established between the patients and the researchers before the study’s commencement, which involved explaining the study’s purpose, addressing participants’ questions, and ensuring informed consent. This was accomplished through a straightforward explanation of the research goals, procedures, risks, and benefits in simple Swahili, emphasizing that participation was entirely voluntary. Participants provided written informed consent. Participants were allowed to express their feelings. Each interview lasted 30–60 min, depending on the participant’s explanations. This was successful through the creation of a strong relationship and trust. Data collection was completed with 16 participants, marking the point of saturation for the study (Supplemental Material).
Rigor
To ensure credibility, in-depth interviews were conducted with each participant. A thematic analysis was conducted, and data derived from verbatim transcriptions of the audio recordings were cross-verified with the field notes. Member checking was implemented during face-to-face interviews, allowing participants to provide feedback to confirm the accuracy and genuineness of the information they shared. In addition, paraphrasing techniques were utilized during data collection to ensure that the responses accurately reflected the participants’ views. The study tool underwent a rigorous peer review to guarantee it effectively captured the intended data. Interviews were led by investigators who are experts in the care of patients with renal failure and those undergoing HD training. Dependability was ensured by sharing field notes with peers and professionals for their feedback, as well as integrating the researchers’ interpretations to foster a deeper understanding of the research context. To ensure confirmability, participants’ descriptions were paraphrased during the interviews and validated for precision. Transferability was achieved by providing comprehensive, detailed information on research procedures, including the methods and timelines for data collection. Researchers engaged in reflexivity by examining their own experiences and biases related to renal failure and HD patients, ensuring that they bracketed and managed these biases to prevent any influence on the study’s findings.
Data analysis
Discussions were transcribed verbatim from Swahili to English and proofread by two researchers to preserve the original meaning by paraphrasing. Interpretive phenomenological thematic analysis was conducted using NVivo software which is owned by Lumivero, a U.S.-based software firm headquartered in Denver, Colorado, following a step-wise template analysis process: This involved familiarization with data, preliminary coding, organization of themes, development and finalization of an initial coding template, and application to the full dataset. The procedures were performed by two research assistants. The researchers conducted independent analyses before merging the themes. In cases of coding disagreements, they compared their codes, discussed their interpretations, and agreed on a final code. This process of resolving differences through consensus helps to maintain trustworthiness and credibility. Another researcher, not involved in data collection, verified each transcript against the corresponding audio. The initial template was open to modification for thorough analysis. Data were analyzed thematically, providing descriptions and participant quotes for clarity and context. Given that this study employs a phenomenological approach aimed at uncovering the lived experiences of patients diagnosed with ESRD and undergoing dialysis, factors such as ethnicity or religion were deliberately excluded. This decision was made to maintain a focus on phenomenological depth rather than shifting toward comparative or sociological analysis.
Findings
Demographic characteristics of the participants
A total of 16 participants were involved in this study. Among them, 12 were males and 4 were females, with a mean age of 49 ± 17 years, ranging from 32 to 66 years. More than half (12 out of 16) of the participants were married. Most of them (nine out of 16) were living with a family member. Most (14 out of 16) participants relocated to Dodoma, where they can access HD treatment (Table 1).
Social demographic characteristics of study participants.
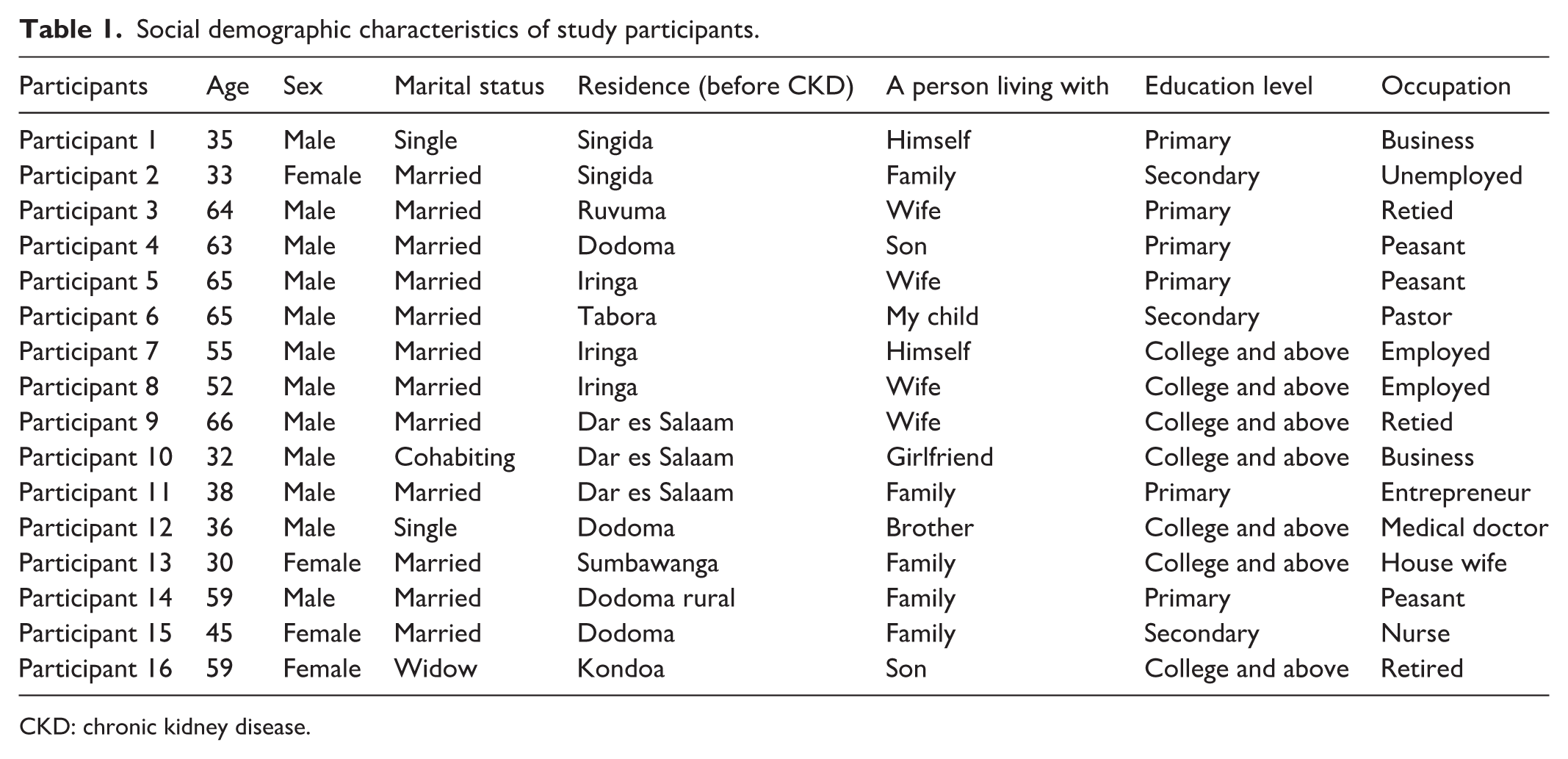
CKD: chronic kidney disease.
History of CKD
The study participants reported their past lifestyle histories; among them, 8 out of 16 had a history of cigarette smoking, 10 out of 16 had a history of alcohol consumption, and 5 out of 16 had a history of both. Most participants elaborated that their chronic renal disease resulted from an underlying condition. Among the causes of CKD mentioned, seven participants cited hypertension as a cause, four had DM, and four of them had both hypertension and DM. Two participants were noted to have an unknown cause of CKD, and one had toxicity from the use of herbal drugs (Table 2).
History of CKD.

CKD: chronic kidney disease; DM: diabetes mellitus.
Identified themes
Table 3 indicates that a total of 7 themes and 24 sub-themes were derived from the participants’ narratives. The themes include the following: (1) Initial reactions to disease and treatment, (2) financial burden and economic impact, (3) dietary and fluid restrictions, (4) psychological and emotional challenges, (5) physical consequences, (6) social concerns, and (7) coping with treatment and disease. Table 3 shows the sub-themes alongside their related themes.
Themes and sub-themes.

First theme: Threads of survival
Upon diagnosis of the disease and introduction to HD treatments, the majority of the participants described feelings of guilt, shock, acceptance, fear, and disbelief as they faced significant life changes and uncertainties. The participant elaborated the following perspectives.
Emotional confusion
Most of the participants said that once they were told that they had kidney failure, they had to start dialysis. They were shocked, and they were afraid because of the expensive nature of treatment, believing the disease was dangerous, and they could not afford it: For sure, at first, I was shocked after I was told that my kidneys had failed, and I had to undergo dialysis! wonder how I would manage the costs, when everyday survival was already a struggle, how could one fight a disease? You see, hemodialysis treatment is extremely expensive. (P1) I was scared, and I was fearing and asking myself what these are?. (P8)
Beliefs of consequence resulting in kidney failure
Many of the participants were young and seemed to struggle to believe their conditions. It took time for them to put it in mind. Some believe this treatment is like other treatments, which means they may be treated and go back home, while others believe they were being witched: . . .It was a painful experience, but at the same time, I struggled to believe it. I thought someone might bewitch me. When I consulted the doctor, he explained that even children could be affected by this disease. One question that remained in my mind was why I was suffering from this illness despite not smoking or drinking. (P11) I didn’t understand, I thought I would be like other patients that I would be treated, then I would go back home. . . during the start I was thinking what caused my renal failure because I am still young, I don’t use alcohol, so I was thinking of how this has happened, also I’m not aged. (P13)
ESRD contrasting with AIDS
Some of the participant shared their feeling of being unwell and how they viewed CKD as a huge disease. Whereby some asserted that HIV/AIDS is preferable to this disease: This disease is huge, it’s better than HIV/AIDS, but this is very crucial, if you don’t get immediate care, you will die. (P6) I felt very bad (patient wants to cry), even if it’s you, when you’re told that your kidney has failed, how will you feel, you will feel bad. . . this disease is very bad compared to other diseases, even AIDS is not a disease compared to kidney failure. . .. (P15)
Almost all participants expressed their thoughts that at first it was difficult to accept. But in the end, they just accepted because HD was the only option; in the end, they were humbled by the treatment: . . .It was difficult to accept, but as days go by, I just coped with it. . .. (P5) My body was swelling, and there was no removal of urine, but at the end I just accepted as I was told I have these and these problems. (P12) . . . even to accept it’s difficult, but at the end I said it’s me, then I accepted. . .. (P15) For sure, I accepted, but I felt so bad, then I said my life has ended, I gave up. (P16)
Second theme: The price of survival
For patients with ESRD, dialysis is not only a treatment but a means of survival at a cost. This is a significant challenge faced by most patients who depend on HD. Managing renal failure and undergoing regular HD places a considerable financial burden, economic loss, and resource impoverishment on patients and their families. Most of them put emphasis on high treatment expenses of (≈60–80 USD) per session, with an average income of 185 USD/month 20 out-of-pocket payment, cost for special diet, travel expenses, time commitment, reduced productivity, and distortion of their economy.
High treatment expenses of (≈60–80 USD) per session
The majority of the participants expressed that this treatment is expensive, which made them sell off home properties, delaying starting treatment, and also failing to afford treatment: Money! Treatment like this is costly, like 200,000Tsh, and sometimes it reaches 250,000Tsh per session, so it makes me come late and not adhere to the given date of follow-up. (P6) In every session I pay 250,000Tsh, and in the week I have to come two times, and sometimes it reaches about 500,000Tsh, can you tell me even a member of parliament can afford paying 4 million per month?. (P10) Leave out those with Health insurance, they are toiling and sometimes they die because they can’t afford treatment. (P15)
Out-of-pocket payment
Participants also shared that the other problem with this treatment is paying cash, whereby most of their friends died, failure to attend three dialysis sessions, and also seeing that it is difficult. This poses most of them with a financial burden and economic consequences: (Yan) Renal failure it’s a burden because its treatment is expensive, especially to the clients who are paying cash. Most of my friends who are paying cash have passed away because they couldn’t afford treatment. (P1) But the big problem is the issue of finances, I am not using health insurance, so I have to pay cash, so in every session I pay 250,000 Tsh, and in the week I have to come two times instead of three sessions, and sometimes it reaches about 500,000Tsh. (P10) I can tell you that this treatment, when you’re paying cash it’s difficult to sustain because of the expenses. (P11)
Cost for a special diet
Participants shared their experience that once you are doing HD treatment. Diet must change; this special diet is expensive. This places them in financial strain: Meat we don’t eat, but we are allowed to eat chicken, but do you have 20,000 Tsh to buy chickens daily?. (P2) The cost of treatment is very high, the good thing is I have health insurance, but there are other expenses that I cannot afford, for example, I don’t have means of transport, and also where I live I have to pay tax, and also food is expensive. (P5) Foods are available and easy example, you can buy fish for 10,000Tsh, and you can stay with it even for a week, but chicken is expensive, where it costs about 20,000Tsh, so it’s expensive. (P6) Now these will make you choose what to eat, you were in love with eating something, but now you can’t eat, so it’s an issue also, these foods are expensive, for example, you have to eat fish, chicken and some vegetables which are expensive for sure. (P7)
Travel expenses
Participants expressed their grief on accessing dialysis services that pose a challenge due to high travel expenses, not having a means of transport, and the cost of fuel. The cost of traveling to the hospital for dialysis sessions has resulted in a significant expenditure and financial burden: You know there is a high cost of transport, for example, I’m living in Mnada mpya, bus fare from there to here is 5,000 Tsh, so the cost is very high. (P4) Still, there are other expenses like travel expenses in week three times and also I am staying in the guest house, so we are suffering. (P7) You know the problem here is just travel expenses, for example, from home to here, I just use ten litres, so there is high expenditure, so in life you must go down because of the high cost. (Participant 8) You know this treatment has brought problems to me in terms of fare, bus fare from where I am living to here is high. (P14)
Time commitment
Most of the participants expressed their grief that dialysis requires the individual to visit the unit three times a week, significantly impacting their schedule and time available for work and other activities. These pose them to significant economic loss and financial burden: . . . you’re required to do dialysis three times a week, what kind of work would you do. . . . (P5) I have to come here three times a week, some production is reduced, also I am a government worker, but now I am here at the hospital, so the duties that I was doing, another person should do it. (P7) Attending three sessions consumes time, and you only have two days now. You will primarily use these two days to rest. . . .working hours have been reduced, now I just work for about three days per week. . . . (P12) Spending three days here at the hospital, every day when you wake up, you just think of going to the hospital, so nothing you can do. (P13)
Reduced productivity and distortion of the economy
Some of the participants expressed that this treatment has caused them significant economic loss. Because now they cannot work due to the limitations of this disease, and their economy is totally distorted: . . .my economy is fully distorted as I cannot do any work, and now I get help from family only. . . if you have kidney failure, you will not do any developmental work, as you will be tired every time and you will be in the treatment, so for the family to be with a good economy it’s difficult. . . . (P4) My economy has been distorted totally, let me tell you in short, you know when you’re a peasant you should have a farm and, in the farm, there are several things that give you money and other services, but bad luck, now my farm remains as forest and I can’t gain anything from the farm. (P5) I tell you I am the entrepreneur, but now my work is not just affected, but it’s beyond damage. (P10) I didn’t participate in agriculture this year. . . they are planting and harvesting millet. . . I have been affected in such a big way because I didn’t participate. . . I have a little harvest, not as planned. (P14)
Third theme: The thirst of survival
Participants shared their experiences that HD treatment affected their normal diet. The need to adhere to restrictions on water intake and also a limited portion of food has been distressing and hurt most of the patients. Restrictions on food choices, as certain foods and fruits become restricted. Most of the participants explained the following;
Restriction of fluid, including local beer
Almost all participants explained that now they are not allowed to drink water as before. Most of the time, they are allowed to drink water when they are taking medicine, and the amount of water should not exceed half a liter per week. Hence, all kinds of industrially made drinks are not allowed, so it is something that they say is not tolerable, and it makes them not enjoy life at all: I am not allowed to drink water, but before I was drinking up to one litre, and if you drink, you have to drink half a liter for one week, and you have to use water when you are taking medicine. (Participant 8) . . . I was using soda, but now no, all juice I can’t use. . . . (P9) . . . even water you’re told not to drink, leave those sodas, but when you drink is during taking drugs. (P11) You are told not to drink soda, but when you come across it, you drink, but you just drink a little because it can be a problem, and you will start coughing. (P15) You have to ask the doctor if it’s allowed. . . You don’t have to exceed a half liter a day. . . sometimes you have to use ice to relieve thirst. (P16)
Limited food choices and options
Nearly all participants explained that their diets have been restricted due to renal failure. They are no longer able to consume red meat or most fruits and face limitations on protein intake. These restrictions result in a loss of essential nutrients and involve specific cooking and preparation methods, such as boiling vegetables and removing the outer layers of chicken. In addition, the limited use of salt has been problematic, causing discomfort and distress for many participants: They impose restrictions that prevent you from eating goat meat, and instead, you should consume chicken meat, which requires you to remove its outer skin. You’re also allowed to eat fish, but the limitations make it challenging. Additionally, you can only have small amounts of ugali, rice, and spaghetti, and you cannot use salt, which is quite bothersome. You are not allowed to eat certain foods, particularly those high in protein, and you must follow specific dietary restrictions. As a result, I have been missing out on important nutrients since there are many foods I cannot include in my diet. (P8) Also, when you have this disease, you’re limited to eating several foods, but you have to get used to eating several kinds of food before, but now you’re not allowed, like everything you’re not allowed to eat (they say don’t eat this, don’t eat this), now you’re left with a few foods. Some of the food you were in love with, and you see them, but now you’re not allowed, so it hurts. (P15) Also, these green vegetables you have to boil and then pour water, then you prepare them and eat, but especially you are allowed to eat Matembele (green vegetable), because they increase blood count. (P16)
Fourth theme: Psychological and emotional disturbances
Almost all participants struggle with psychological and emotional problems, which is due to the distressing nature of this treatment and disease. As this treatment resulted in feelings of despair, loss of friends and loneliness, mental distress, and uncertainty.
Feeling of despair and loneliness
Participants express feelings of despair and loneliness due to being away from their family, not being able to eat food, and being unable to engage in regular activities like work and travel, a perception of other people that they will die, and feeling that life has ended. This situation takes a toll on their mental well-being: Ooooh, that is hurting me, because when I was in Iringa, I was doing my activities, as you know I am a farmer, I have my plans, and now adapting to a new environment and condition, it’s hurting. (P5) I was living at my place with my relatives, where I was respected and famous too, so being away from them affected me psychologically. (P6) The big issue is to stay far from them because I am here at Dodoma, and my family is at Iringa now. Being far from them it pains . . . being away from family, you’re not eating food, also you’re not working, you can’t travel, also coming here three times a week it’s destroying my mind. . . . (P7) Because when you have renal failure people will think that you’re going to die. (P10) Also, you will be stressed that they will dismiss me from my job, you will be thinking of your friends, and as you know now, I have left work for two years, I will always be stressed about what will happen?. (P15)
Loss of friends
Participants shared their feelings that when doing HD treatment, it requires them to spend a significant amount of time in the hospital: (agh) Also, this treatment can make you lose friends because most of the time you will be spending at the hospital because of the treatment, sometimes friends can see that you need their help every time, so they will be tired of you. (P1) Relatives, they were supporting me at first, but when they saw that I have stayed here at the hospital for more than a month, they started moving away one after another. I remained with my family. Then I decided to go and find a house near the hospital and am staying by myself, so all relatives left after they were told that this is a chronic disease. (P2)
Mental distress and uncertainty
Participants elaborated that the psychological impact of dialysis includes constant worry and thoughts about the future, survival, not enjoying life, frequency of hospital visits, being dependent, memory loss, and uncertainty surrounding the treatment. There is a constant concern about affordability and the consequences if the treatment cannot be afforded: I can’t recall easily, you know, before I was doing my activities, most things, I was able to remember, but now I forget. Mmmh!!! Now, I have lost memory. (P3) But to my side, it has distressed me because I was using meat and milk as food, but now, I can’t use it again, so I feel like I am not enjoying it. (P4) I can’t do any work; I just depend on others. Anything that I need, I should call my children for help, it’s disturbing me a lot. (P5) The big issue is thinking of what will happen, what next, am I going to survive or not, so this thing is disturbing and repeating in the mind, why me, what happened to me and sometimes I just come here but am asking myself what will happen because dialysis is just a machine helping me to remove waste. (P8) At first, when I am talking to you and recall the image of what I am passing through, I want to cry for sure, you can tolerate it, but it reaches the time it’s painful for sure. (P15)
Fifth theme: Physical effects
Almost all participants gave out their perspective that ESRD and HD posed significant physical limitations. These limitations include fatigue and tiredness, inability to walk, and changes in body image.
Fatigue and tiredness
Because the machine removes waste and water from my body, now after dialysis I feel so tired, not like a normal person. (P7) . . . when I come out from the machine, I will be so tired. . . . (P12) . . .my ability to do work has declined because of tiredness after dialysis. . . . (P9)
Walking inability
You know when I was at work, I was able to walk 60km, but now I can’t walk even a 1/4km. (P4) You can’t walk, and also you were able to drive a car, but now you have to find a driver. (P6) Before this treatment and disease, I was able to walk for a long period, but now, I can’t walk for a long time, also walking fast is a problem. (P9) For instance, I am not able even to walk, so I can’t do any productive work; moreover, I am just sitting. (P15)
Change of the body image
A person who knows me before and now he will be amazed, because my body has changed a lot, you know this shirt was fit to me, but now it’s not fitting (let me show you my pictures). (P10) My body weight has decreased. I was not having this weight. My weight was 65 kg, but now it’s 39kg. Then I didn’t feel good because I was having a good weight, but now, I have a low weight. (P15)
Sixth theme: Social concern
Most emphasis on family, social support, and good relationships with healthcare providers and other patients.
Support from family
Because it’s a disease, family support is high. . . I get support from my children, whom I supported when they were young, so now I get support from my children. So, it has helped me to cope with the condition. (P4) I get support from my two children, who are teachers, so one of them gave me BIMA, while the other gives me bus fare daily. (P14)
Relationship with healthcare providers and other patients
Participants shared that they have a good relationship with healthcare providers. These helped them to cope easily with the treatment and the disease condition. Also, they have a good and strong relationship among themselves, whereby they make stories together, also making contributions when their colleague has a problem: When we are in the sitting bay there waiting for medicine, we make different stories and just shout sometimes people say are these people fighting, and sometimes if your friend has no money for tea or bus fare, you get support from others so you forget if you have a problem. (P2) At first, health care providers were near to me and they were comforting. . . care here is maximum. (P4) We have a strong relationship with them, because when we come here, we make stories, even when our friend dies, we make some contribution to support. . . health workers here, they are cooperating with us even when you are absent, they can ask where you were?. (P16)
Social isolation
Participants shared their experience that dialysis centers are located in urban hospitals, and people who need dialysis need to shift from their homes to cities where they can get dialysis treatment. This geographical displacement puts them in social isolation; they cannot see their people. Because of the financial crisis, relatives cannot travel to visit their relatives. This physical separation contributes to the loss of social ties. Also, participants shared that their participation in society has decreased due to their health condition, life restrictions, and the time constraints imposed by dialysis. They feel separated from their family, friends, and neighbors. They also mention a shift in their mindset, where they no longer prioritize pleasurable activities: . . .other thing, if you’re invited to the ceremony, what are you going to do, it’s just putting me into temptation, because now people are just eating fried food like fried banana, meat and Soda, so what are you going to eat. . . . (P2) Now I am away from them, so they see I am separated from them, but most of them know that I have a problem. (P9) The disease has limited me from going to the nightclubs, drinking alcohol and all pleasures, so to some point it disturbs me. But now I don’t think about anything pleasurable. (P12)
Seventh theme: Coping strategies with treatment and disease
The coping mechanisms expressed by most participants included accepting the condition as it is and adhering to restrictions, venting emotions, and having hopes and expectations that a dialysis center could be established in their local regions and reducing the traveling cost. Most participants explained that, initially, it was difficult to cope with their condition, but over time, they accepted the treatment and managed well.
Accept the condition as it is and adhere to the restriction
A person receiving a diagnosis of ESRD, their attendance at dialysis sessions may indicate an acceptance of their condition. Our findings reveal that acceptance is not merely a prerequisite for treatment but rather an illuminating theme that represents a complex and ongoing process. In Tanzania, this acceptance is influenced by cultural beliefs regarding illness, financial constraints, and trust in family caregivers. Patients described a journey from initial shock and disbelief to a gradual reconciliation with the realities of ESRD, demonstrating resilience and adaptability in a resource-limited environment. This path emphasizes the uniqueness of acceptance as a lived experience, rather than simply an anticipated outcome of attending treatment.
Accepting renal failure and adhering to dietary restrictions, adjusting their working days, and seeking financial support through health insurance are some coping mechanisms employed by individuals undergoing dialysis treatment: I have to follow restrictions for the safety of my life, and if you can’t follow the restrictions, you will have more complications and your life will be in danger, so you have to follow what you’re told. (P1) I just force myself to eat, but in terms of finances, I just work for at least four days now, so I just go with it. (P9)
Venting emotions with family and friends
Participants shared their perspective that once a dialysis center is constructed in their area. It can treat their psychological stress because they will be with close relatives, families, and friends, they will share some emotions together, and also, it can help them cope with the disease and treatment easily: I wish I could be near my people; I could have time to speak to them about my problem, and I hope they could understand the situation and be close to me. If these services are provided at my place, it can help me in performing some activities at home, for example, small farming and also keeping chickens, so when these services are near, it will be easy to perform my activities. (P5) If God wishes when they accomplish building one of the center there in Tabora (my home place), I will go there because there at Tabora I have like 4 houses and Ulambo I have 3 houses so I will save money when I will be there, also it will treat my psychology as well because talking with people close to you its therapy. (P12)
Discussion
The study aimed to understand the lived experiences of patients undergoing HD and wanted to explore coping strategies with both the disease and the difficulties of therapy. The key emerging challenges include patients traveling long distances for treatment, bearing the heavy financial burden of HD, and adjusting to adhere to dietary restrictions, all of which deeply affect their physical, psychological, and emotional well-being. Recognizing these challenges is important as the increase of CKD poses a significant public health issue in Sub-Saharan Africa, including Tanzania, and HD remains the primary treatment option for most patients. These findings highlighted the medical, social, and emotional aspects of CKD management, indicating areas where health systems can improve quality of life and patient outcomes through accessible, affordable, and holistic care.
The current study found that participants had threads of survival after being diagnosed with CKD, and the need for HD includes emotional confusion (shock), fear, belief in CKD, and guilt. These reactions align with existing literature, for example, similar studies conducted by Sah et al. in Nepal. 21 Another study carried out in Taiwan reported comparable findings, revealing that some participants reacted differently; some experienced shock, hopelessness, restlessness, and cried for hours. 22 Another study from Iran found similar outcomes, with some participants expressing fear of HD mechanisms, fear of loneliness after being rejected by family and spouse, fear of becoming ill in the community, and fear of death 23 and a study conducted by Bonsra et al. in Ghana, which reported patients’ emotional feelings after diagnosis of CKD that were shocking and distressing, with many experiencing depression, anxiety, or suicidal thoughts.
The probable reason for these feelings in patients could be their lack of preparedness to receive information regarding CKD; moreover, its lifelong management, which is costly and requires HD to be conducted three times a week continuously until the patient can undergo a renal transplant. Moreover, these reactions, frequently accompanied by feelings of incomprehension, underscore the challenges patients encounter when struggling with a diagnosis of CKD and its associated treatment. Over time, the emotional turmoil characterized by confusion, fear, and guilt can evolve into more persistent and complex states of depression and sadness. This progression negatively impacts medication adherence, leading to poorer outcomes, reduced social support, feelings of helplessness, a diminished quality of life, and an increased risk of mortality. The ongoing emotional turmoil and guilt identified in this study underscore the necessity for a comprehensive integration of renal treatment and mental health interventions to better support patients’ emotional well-being.
The association between financial burden and HD treatment among patients with CKD who are undergoing HD has been reported by many studies. In this study, special dietary requirements, travel expenses related to treatment, shifting from home to stay in nearby areas for easy access to dialysis units, reduced productivity, economic strain, disruption of daily obligations, and significant time commitments were considered. Research conducted elsewhere supports our findings by highlighting the costs associated with HD treatment, including findings from studies in Pakistan, 24 Nepal, 21 and Taiwan. 22 The possible explanation includes the fact that HD treatment is expensive, especially for patients who pay out of pocket. The cost of a single session ranges from 200,000 to 250,000 TZS. Furthermore, patients are required to attend a minimum of three sessions each week. Consequently, some patients experience delays commencing HD, and some have poor adherence to treatment, which can result in adverse outcomes, such as increased intra-dialytic weight gain due to retention of fluid, leading to pulmonary edema, cardiovascular complications, high serum phosphate levels, and ultimately death.25,26 In addition, poor adherence to HD is linked to increased risk of hospitalization, the need for additional investigations, and increased medication expenses,25,27 which, in general, raises the cost of management and puts patients at a greater risk of morbidity and mortality.
In the current study, participants experienced restrictions on their dietary and fluid intake due to thirst for survival. They reported that their lives have changed due to limited food choices and options, as well as restrictions on portion sizes and water intake. These findings align with phenomenological studies conducted in Chitwan, 28 Pakistan, 24 Ethiopia, 1 Perumbavoor, and Kerala. 29 Other scholars reported that patients were guilty due to lifestyle restrictions, including foods and fluids. Although the restrictions were beneficial, most participants felt guilty about HD and perceived it as expensive and unfriendly because it is dependent. For instance, they reported being restricted to red meat and allowed to eat fish and chicken without skin. This also hindered their social functioning due to the limited selection of food and fluids.
Participants experienced psychological difficulties and emotional suffering, and patients feel despair and loneliness, loss of friends, mental distress, and uncertainty. This finding was supported by various studies, including those conducted in India,28,29 Pakistan, 24 and Ethiopia. 1 The probable reasons for these psychological effects could be lifestyle changes due to restrictions on food and fluids, alterations in physical activities, the cost of HD, investigations and medications, fluid retention causing edema, difficulty in breathing, and reduced productivity. Another reason could be experiencing the death of fellow patients with whom they used to perform HD together, as well as those who have healed and undergone a kidney transplant, uncertainties about disease progression, and HD therapy complications. Healthcare providers should be aware of these effects that patients are experiencing and offer holistic care in a friendly manner, maintaining a positive outlook toward these patients. The government should reconsider reducing the cost of treatment for the population undergoing HD, recognizing that their productivity has decreased and they are unable to earn enough money to cover HD and other expenses.
Regarding physical consequences, participants revealed that they experience fatigue and tiredness even after small activities, which leads to an inability to walk strongly, and they notice changes in body image. Our findings are similar to those of various studies conducted worldwide, such as the study in Turkey, 30 Scotland, 31 Iran, 32 and Oman. 33 The probable reasons for patients on HD treatment could be explained by the fact that these patients often have low levels of hemoglobin due to reduced erythropoietin production, iron deficiency, and malnutrition related to restricted diets. In addition, fatigue can be caused by the accumulation of toxins (waste products) in the body. Therefore, family members should be educated and should reduce the responsibilities they assign to these patients. Instead, they need to provide food rich in iron to help reduce fatigue.
Concerning social support, in this study, participants shared their experiences of receiving full support from family members and healthcare providers. In addition, participants reported that even their colleagues’ patients who are also treated with HD are shown support, for example, they can give each other food or bus fare support when one has a financial problem. This finding aligns with the previous studies conducted in Athens, Greece, 34 Technological Educational Institute of Athens, 35 Poland, 36 and Indonesia. 37 Social support is an important parameter in the care and management of patients with ESRD under HD.
Support from family
In this study, some participants described their coping mechanisms as accepting the situation, venting their emotions, and believing that treatment could be made more accessible near their homes. This result aligns with findings from other scholars, such as a study conducted in Portugal 38 and the United States, 39 which reported that participants’ coping mechanisms included following doctors’ orders, accepting renal failure and HD, and relying on family and friends. The fact that patients with ESRD experience psychological stress and need emotional support makes having coping mechanisms important for them to adhere to the treatment regimen and lifestyle changes.
Healthcare providers and family members need to understand what patients go through, be close, and listen to patients to help reduce their emotional distress by creating a welcoming environment with opportunities for informal social interaction during treatment sessions, which will improve adherence to dialysis schedules and dietary restrictions, reduce depression and anxiety, enhanced patient satisfaction and trust in providers, and better long-term survival and quality of life. 40
In this study, the majority 9 of participants were aged above 50 years. Similar findings have been reported in other studies, for example, a study conducted in Denmark reported that the mean age for CKD patients was 76.4 years, and DM, hypertension, and cardiovascular diseases were prominent in the patients with CKD, 41 Nepal reported that older ages of more than 60 years were significantly associated with CKD. 42 Aging is a crucial factor linked to various behavioral lifestyle elements, such as sedentary habits, excess weight, and unhealthy eating patterns, all of which exacerbate non-communicable diseases. The aging process heightens the risk of conditions like hypertension and DM, which, in turn, are leading causes of CKD. 43 Aging is a crucial factor linked to various behavioral lifestyle elements, such as sedentary habits, excess weight, and unhealthy eating patterns, all of which exacerbate non-communicable diseases. The aging process heightens the risk of conditions like hypertension and DM, which, in turn, lead to causes of CKD. 43 The study population represents the population with ESRD, since the majority of them are not financially well off because of old age, and some of them have retired from employment, and they cannot afford the dialysis services required.
The results highlight the critical need to improve renal health services in the larger context of universal health coverage. Tanzania is not an exception to the global increase in ESRD and CKD. With few dialysis facilities, unequal access to transplants, and insufficient preventive measures, current service delivery is dispersed. Patients suffer from poor outcomes, high out-of-pocket expenses, and delayed diagnosis in the absence of a coordinated plan. There is a need to create a Renal Health Plan which would offer a methodical approach to treatment, early detection, and prevention. Such a plan should guarantee sustainable funding, expand dialysis and transplant services fairly, and incorporate renal health into primary care. In addition, it would reduce the strain on tertiary hospitals, enhance patient survival, and improve the quality of life. Moreover, the findings of this study reveal clinical implications that the healthcare providers should focus not only on treatment but also on the psychological care, patients need holistic care, including psychological support.
Policymakers should know HD is a mandatory treatment for patients with ESRD. In addition, it is important to implement in-service training for healthcare workers on HD and to make HD services more accessible to the community while reducing travel costs. These strategies could significantly enhance patient adherence, satisfaction, and long-term outcomes. Future studies should focus on the psychosocial burden, stigma, guilt, and illness perception on how they influence disease prognosis using a mixed-methods approach, both quantitative and qualitative, to scale up a larger population, and also, should integrate patient-reported outcomes such as psychological issues into trial design and service evaluation, ensuring patients are treated with evidence-based research.
Limitations of the study
The study utilized a cross-sectional design, which means that no causal relationships or effects can be inferred. Another limitation pertains to self-reporting, which may result in recall bias and inaccuracies in reporting. In addition, the small sample size and the fact that the study was conducted in a single region could impact the generalizability of the findings, while the purposive selection of participants may introduce selection bias.
Conclusion
The findings provide valuable insights into the experiences of patients with ESRD who are dependent on HD for survival. The emotional and financial burdens associated with ongoing HD treatment significantly affect the lives of both patients and their families. Many patients find it necessary to reduce their working hours due to the time-intensive nature of the treatment and the physical side effects of HD. Nevertheless, some individuals can continue working with adequate support. Despite the challenges they face, many patients manage to maintain a positive outlook and stay engaged in their lives. In addition, several participants noted that while this disease can be cured through transplantation, issues related to funding, high costs, and limited access remain significant barriers. The government should take measures to reduce treatment costs and expand HD centers, as these patients have already faced a decline in their income. This is essential for attaining universal health coverage and ensuring that renal health receives the attention it deserves in public health policy.
Supplemental Material
sj-docx-1-smo-10.1177_20503121261437155 – Supplemental material for Costs beyond daily survival: Lived experience of patients with dependent end-stage renal disease on hemodialysis in Tanzania: A phenomenological study
Supplemental material, sj-docx-1-smo-10.1177_20503121261437155 for Costs beyond daily survival: Lived experience of patients with dependent end-stage renal disease on hemodialysis in Tanzania: A phenomenological study by Angelina A. Joho, Herman Joel Sule and Aisha Tambwe in SAGE Open Medicine
Footnotes
Acknowledgements
Special thanks to the Benjamin Mkapa Hospital administration for enabling us to interview the patients, the staff at the HD center in BMH for their cooperation, and patients with ESRD for providing consent to be interviewed.
Ethical considerations
Ethical clearance was obtained from the Institutional Review Committee (IRRC) of the University of Dodoma in May 2023, with reference number MA.84/261/01/62/332. Before participation, all participants had to sign the informed consent, and all principles of research ethics were adhered to according to the Declaration of Helsinki (World Medical Association, 2001).
Author contributions
The author’s contributions are written under the CRediT statement: A.A.J.: conceptualization, methodology, analysis, acquiring data, article writing, visualization, project administration, and supervision. H.J.S.: conceptualization, methodology, analysis, and acquiring data. A.T.: conceptualization, methodology, and article writing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Researchers interested in data from transcripts from the interviews will be made available to them after securing ethical approval from the University of Dodoma Research Ethics Committee.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.