
Abstract
Background:
Helicobacter pylori (H. pylori) infection remains highly prevalent in low- and middle-income countries and is a major cause of chronic gastritis and upper gastrointestinal morbidity. In endemic settings, infection was often influenced by environmental and hygienic exposures. Data examining these associations among symptomatic gastritis patients in Pakistan are limited.
Objective:
To describe the prevalence of H. pylori positivity and examine its association with environmental, hygienic, and lifestyle characteristics among patients with clinically diagnosed gastritis in Northern Pakistan.
Methods:
This multi-center cross-sectional study was conducted from January to December 2024 in 3 tertiary-care hospitals in Islamabad, Rawalpindi, and Wah Cantt. Patients aged ⩾16 years with clinically diagnosed gastritis were consecutively enrolled. H. pylori status was determined using invasive and non-invasive diagnostic modalities employed in routine clinical care. Sociodemographic, environmental and behavioural data were collected using a structured, pilot-tested questionnaire. Associations were assessed using chi-square or Fisher’s exact tests.
Results:
Among 250 participants, 225 (90.0%) were H. pylori positive. Infection status was not significantly associated with age, sex, education level or place of residence. In contrast, untreated drinking water, absence of household water treatment, poor hand hygiene, skipping or delaying meals and consumption of uncooked or undercooked food were significantly associated with H. pylori positivity (p ⩽ 0.001). There were substantial overlaps in gastrointestinal symptoms between infected and non-infected patients. In H. pylori-positive people, post-treatment eradication was noted in 65.6% and recurrence in 40.0%.
Conclusion:
In this endemic area, the prevalence of H. pylori positivity became very high among individuals who surpassed the clinical diagnosis of gastritis. Infection status was strongly associated with environmental and hygienic factors in this symptomatic population. These results reflect associations and not causal determinants and emphasize the need of longitudinal studies.
Introduction
Helicobacter pylori (H. pylori) is a Gram-negative, spiral-shaped bacterium, which inhabits the gastric mucosa of the human body is typically acquired at an early age by either faecal–oral or oral–oral routes.1,2Although it is still one of the most common chronic bacterial infections in the world, it is closely related to chronic gastritis, peptic ulcer disease and gastric adenocarcinoma. 3 Although the prevalence of H. pylori infection has declined in high-income countries worldwide, in low- and middle-income countries, where individuals are exposed to environmental exposure, crowded living conditions, may face lack of access to safe water and sanitation, the infection continues to impose a substantial clinical and public-health burden. 4
Pakistan has high prevalence of H. pylori infection that has been reported consistently among patients who presents with dyspeptic symptoms and endoscopically diagnosed gastritis. 5 With these endemic conditions, infection can frequently continue into adulthood and can be a combination of childhood infection and ongoing exposure. As a result, H. pylori gastritis often coexists in symptomatic patients with other etiologies of persistent upper gastrointestinal symptoms, which make it difficult to diagnose and treat. 6 Clinically, chronic H. pylori-related gastritis is also relevant as an important infectious mimic of inflammatory and functional gastrointestinal disorders, especially in areas that have a high rate of enteric and parasitic infections. 7
An emerging literature indicates that there is an association between environmental, hygienic and lifestyle factors that can lead to H. pylori infection in endemic environments these include unsafe, untreated or poor household water treatment, promotion of poor hand hygiene and dietary habits.8,9 A good part of the existing evidence, however, is community-based or paediatric-based populations, whereas limited studies have targeted adults with clinically diagnosed gastritis, in a highly selected and symptomatic group. 10 Identifying factors linked to being H. pylori positive in these type of populations may simply place the infection within real-world clinical practice, rather than implying upstream risk prediction or causality.
Furthermore, the interpretation of the H. pylori-related data is further complicated in high-prevalence settings by diagnostic heterogeneity, limited availability to culture and antimicrobial resistance testing and the use of a combination of non-invasive and invasive methods of diagnoses. 11 These challenges mentioned above highlight the importance of a careful interpretation of associations and the need to be specific when differentiating between correlates found in a clinical population and determinants of infection acquisition. 12
In this context, the present multicenter cross-sectional study aimed to describe the prevalence of H. pylori positivity and examine its association with environmental, hygienic and lifestyle characteristics among patients with clinically diagnosed gastritis presenting to tertiary-care hospitals in Northern Pakistan. By focusing on a symptomatic gastritis population in an endemic setting, this study seeks to contribute clinically relevant, context-specific evidence while explicitly acknowledging the limitations inherent to its design.
Materials and methods
Study design and setting
The study was a multicentric cross-sectional study that involved gastroenterology departments of three tertiary-care hospitals located in Northern part of Pakistan as follows: Pakistan Institute of Medical Sciences, Islamabad; Holy Family Hospital, Rawalpindi; and Pakistan Ordnance Factories (POF) Hospital, Wah Cantt. These are hospitals catering to the urban and peri-urban populations and referrals are from the neighbouring districts of Northern Punjab and the Islamabad Capital Territory. The research was conducted within 12 months January-December 2024.
Sample size calculation and study population
The sample size was estimated using the single-proportion formula for cross-sectional studies, assuming a prevalence of 60% for H. pylori infection, 5 a 95% confidence level and a 6% margin of error. The calculated minimum sample size was 256; however, 250 participants were included based on feasibility and complete data availability, which was considered adequate for descriptive and associative analyses. Eligible screening of patients who appeared with signs and symptoms suggesting the presence of gastritis were done. There were 285 patients who were initially assessed. Among these, 35 patients were eliminated because of very recent treatments of H. pylori eradication, severe comorbidity, being pregnant or having malignancy. In the final analysis, 250 patients met the eligibility criteria and participated in the study (Figure 1).

Flowchart illustrating participant enrollment, screening, inclusion and exclusion.
Eligibility criteria
Inclusion criteria were
Age ⩾ 16 years
Diagnosis of clinically diagnosed gastritis using endoscopic data and/or according to the compatible clinical evaluation.
Presence of a minimum of a single H. pylori diagnostic test outcome.
Living in the study area a minimum of 1 year.
The exclusion criteria were
H. pylori eradication therapy within the preceding 6 months
Known autoimmune gastritis or other chronic gastrointestinal diseases
Severe comorbid illnesses, including liver cirrhosis
Pregnancy or lactation
Gastrointestinal malignancy (stomach, oesophageal or oropharyngeal)
Outcome definition
The primary outcome was H. pylori infection status among patients with clinically diagnosed gastritis, assessed at the time of evaluation.
Diagnostics methods
Upper gastrointestinal endoscopy
Clinical indication was the basis on which upper gastrointestinal endoscopy was done on patients using standard Olympus fibre-optic gastro-duodenoscopes. Before the process, vital signs measurements were conducted and patients positioned in the left lateral decubitus. The oesophagus, stomach and anterior and first and second parts of the duodenum were thoroughly inspected. In line with the standard infection-control measures, endoscopes were disinfected between patients with cetrimide, 70% alcohol and the Cidex(r) solution, and then rinsed with distilled water. Endoscopy was mostly done to assess the mucosal pathology and severity of gastritis and not as a definitive marker of H. pylori infection status.
Gastric biopsy and histopathology
Pinch mucosal biopsies were taken on the gastric antrum, corpus and the visibly abnormal sites during endoscopy. The biopsy samples were preserved using formalin and subjected to histopathological analysis. The hematoxylin and eosin staining was used to diagnose chronic gastritis histologically, whereby the lamina propria is mononucleated by or without plasma cells. The infection of H. pylori was diagnosed by way of modified Giemsa staining that is very sensitive and specific in identifying the presence of H. pylori organisms. Microscopic examination was done by skilled consultant histopathologists.
Bacterial culture
H. pylori culture was performed in a limited subset of patients due to technical complexity, transport requirements and resource constraints. A sample of the gastric biopsy was collected in a transport media and transported within 24 h in a temperature-controlled environment to the Department of Pathology of the Pakistan Emirates Military Hospital. Specimens were placed onto selective culture media and incubated under 3–5 days under the microaerophilic condition of 37°C. H. Pylori was identified using the features of colon morphology, Gram staining and routine biochemical tests such as catalase, oxidase and urease. Culture was not a major diagnostic requirement because of its limited feasibility and was less than descriptively reported in places where it was covered.
Non-invasive diagnostic tests
Non-invasive diagnostic modalities were urea breath testing, stool antigen testing, and these modalities were conducted, based on standard clinical guidelines when they were available as shown in Figure 2. Immunoglobulin G (IgG) antibodies serologic testing was also a supportive, but not a relied upon, predictor of prior exposure, since it could not differentiate between current and past infection in endemic areas.

Diagnostic decision tree for Helicobacter pylori infection in patients with suspected gastritis.
Assessment of clinical characteristics
Through clinical assessment and patient interview, the clinical symptoms, such as epigastric pain, nausea, vomiting, bloating, abdominal discomfort, heartburn, loss of appetite and abdominal pain related to meals or associated with non-meal meals were observed. The symptoms were recorded as either being present or absent upon evaluation. 13
Treatment regimens
Patients with H. pylori-positive patients were recorded being treated according to the routine clinical practice as shown in Table 1. These were the usual triple therapy, the bismuth-based quadruple therapy and the rest which were the proton pump inhibitor-based and other therapies. Choosing therapy was selected as the doctor treating the patient chose at his/her own discretion, according to clinic judgement and regional custom. 14
Classification of treatment regimens according to guideline-based categories.

Assessment of treatment outcome
It was measured at a minimum of 4 weeks (1 month) after the completion of the eradication therapy according to the international recommendations. The non-invasive diagnostic testing (urea breath test or stool antigen test) was used to determine post-treatment H. pylori status, where possible. 15 A negative test result on post-treatment was considered to be a successful eradication measure that had been achieved at least 1 month post-therapy. Resolution of the symptoms was not taken as an indicator of effective eradication.
Definition of recurrence
Recurrence was defined as re-detection of the infection after negative post-treatment test which has been negatively detected during the clinical follow-up. No molecular strain typing was done, and the study was cross-sectional; hence, recrudescence mortality could not be distinguished by differentiation with reinfection; consequently, recurrence was described as a composite result of either persistent infection or newly acquired infection in this endemic locality. 16
Exposure variables
A structured interviewer-collected questionnaire was used to determine environmental, hygienic and lifestyle exposures. Primary drinking water, household water treatment (boiling, filtration, chlorination), shared water, handwashing habits, consumption of uncooked or undercooked food, meal skipping or postponement, physical activity, diet, self-report stress or anxiety.
Questionnaire development
The questionnaire was developed after the consideration of the existing literature17,18 and international guidelines on epidemiology of H. pylori. It was first made in English and translated into Urdu and then translating back to make sure it is conceptually correct. The questionnaire was pilot-tested before formal data collection in about 10% (n = 25) of the intended sample size in one of the participating centres. These subjects were qualified to be considered eligible; however, they did not appear in the final analysis. There were some slight corrections to enhance the understanding and sequencing. The final instrument demonstrated acceptable internal consistency for hygiene and lifestyle domains (Cronbach’s alpha = 0.78).
Data collection
Interviewer-administered questionnaires and medical record review were used to collect the data. Treatment, follow-up and diagnostic data were taken out of clinical files. Every data was verified of completeness and internal consistency before analysis.
Data analysis
IBM SPSS Statistics version 25 was used to analyze the data. The frequencies and percentages summarized categorical variables. Classification of H. pylori infection status was compared to categorical variables based on chi-square or fisher exact tests according to their appropriateness. Since it was based on cross-sectional design, results were interpreted as correlations and not causations. The level of statistical significance was p < 0.05.
Ethical considerations
The research was done in compliance with the Declaration of Helsinki (2013 revision). This research was carried out at POF Hospital, Wah Cantt, with the ethical approval of the Institutional Review Board of the Wah Medical College and administrative consent of the involved hospitals. Informed consent of the participants was obtained in written form. In the case of limited literacy, a consent form was read aloud in the local language and signed by thumb impression by the presence of a witness. In the case of minors, there was written consent by legally authorized representatives. Data anonymity and confidentiality of participants were observed.
Results
Table 2 shows the demographic, socioeconomic and behavioural characteristics of the 250 study participants. H. pylori infection was found in 225 (90.0%) of the cases. The majority of the population were female 146 (58.4%), aged 31–45 years 112 (44.8%), lived in Rawalpindi 130 (52.0%) and in urban settings 132 (52.8%). A third of the study population had received college-level education or higher 83 (33.2%). Most of them are self-employed 85 (34.0%), and 96 (38.4%) indicated they made less than PKR 50,000 a month. The majority of the water source was municipal tap water 135 (54.0%), and 126 (50.4%) had shared water sources. The water treatment practices were less than ideal as boiling 103 (41.2%), filtration 109 (43.6%) and chlorination 73 (29.2%). The prevalence of behavioural factors was high: spicy food intake 58 (23.2%), physical inactivity 77 (30.8%) and anxiety or stress 49 (19.6%). Additionally, 112 (55.2%) did not wash hands before eating, and 118 (47.2%) reported skipping or postponing meals.
Demographic, socioeconomic, and behavioural characteristics of the study participants (n = 250).
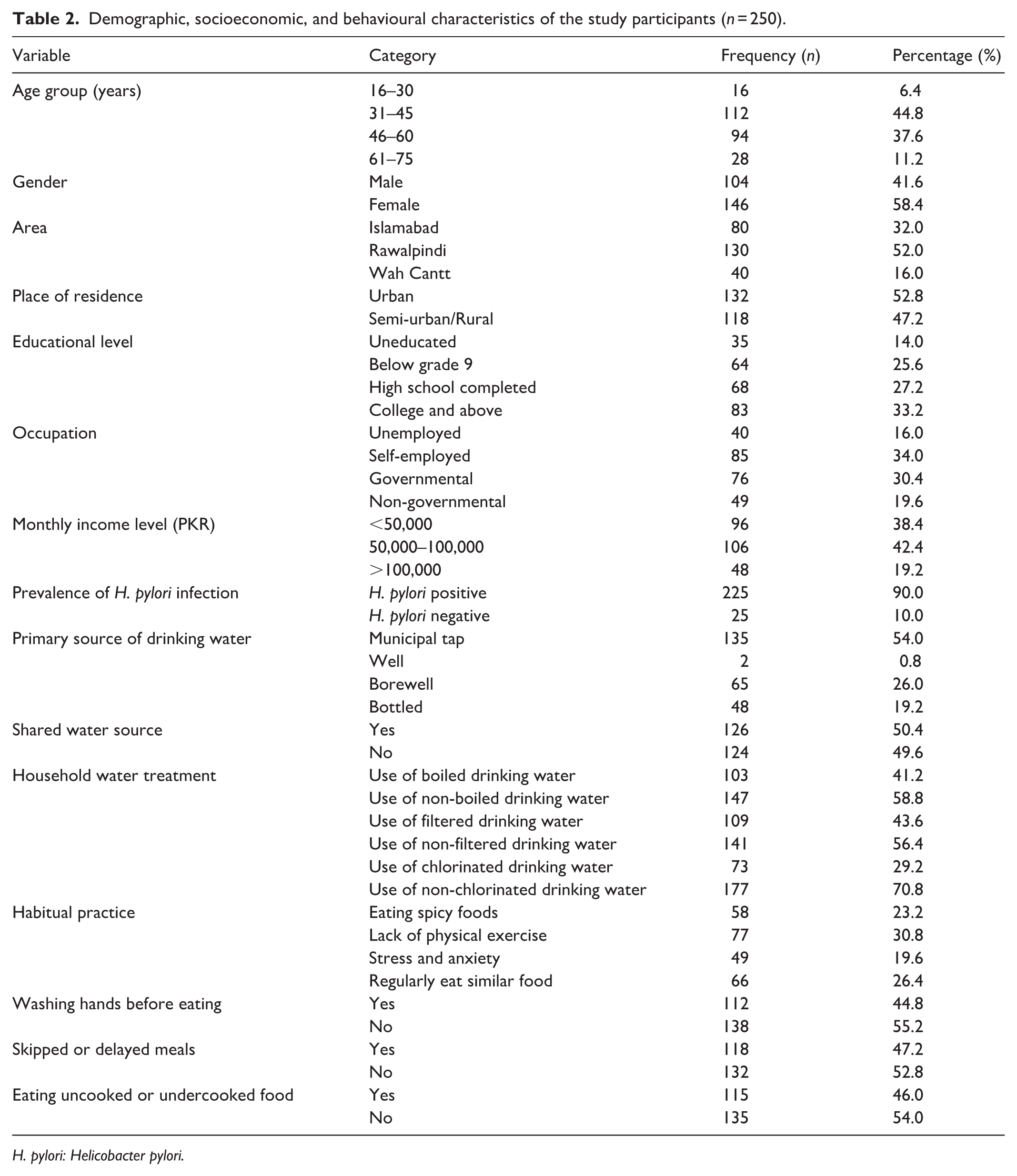
H. pylori: Helicobacter pylori.
Table 3 shows that gastrointestinal symptoms, such as epigastric pain, nausea, vomiting, bloating, abdominal discomfort and heartburn were frequent and significantly overlapped between infected and non-infected patients. Non-invasive diagnostic tests, such as urea breath test and stool antigen test, were commonly applied in both groups, and supporting test that is, serologic IgG was also commonly used, indicating its poor capabilities to differentiate between active infection. More often invasive diagnostic procedures were more commonly reported in patients with H. pylori such as rapid urease test, histopathology biopsy and cultures. Approximately half of the participants in both groups had upper gastrointestinal endoscopy. Altogether, clinical symptoms were not discriminatory of infection status, which was mainly ascertained by microbiological and histopathological results.
Association of clinical characteristics and diagnostic methods in study population with H. pylori status (n = 250).

IgG: Immunoglobulin G; H. pylori: Helicobacter pylori.
Table 4 shows that out of the patients infected with H. pylori (n = 225), the most frequently used treatment regimen was standard triple therapy (36.8%), bismuth-based quadruple therapy (32.8%) and other treatment regimens (30.4%). Evaluation of post-therapy showed that (65.6%) of patients receiving the treatment were negative and (34.4%) of patients remained infected after therapy. The results of the follow-up showed that (40.0%) of the total study population had recurrence of infection in the future and (60.0%) did not show any trace of infection. The findings suggest that the rate of initial eradication was moderate with a high percentage of patients having persistent or repeat infection in this endemic region.
Treatment regimens, outcomes and recurrence among H. pylori–positive patients (n = 225).
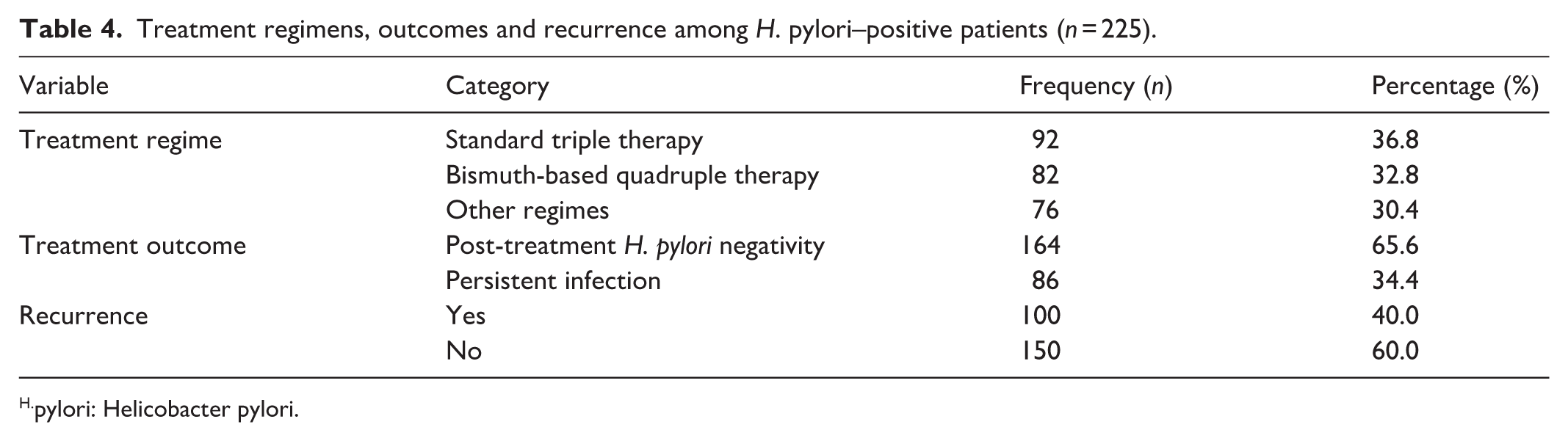
pylori: Helicobacter pylori.
Table 5 demonstrates that socio-demographic characteristics including age group, gender, area of residence and educational level association with the H. pylori infection status was not statistically significant. Conversely, some of the environmental and behavioural factors showed significant association. H. pylori was strongly associated to the intake of non-boiled, non-filtered and non-chlorinated drinking water (all p < 0.001). Poor hygiene and dietary practices including not washing hands before eating, skipping or delaying meals and consumption of uncooked or undercooked food, were also significantly associated with infection (p ⩽ 0.001). Habitual habits like the intake of cooked or uncooked food, lack of physical exercise and stress or anxiety were not significantly associated with the status of H. pylori. In general, drinking water that was untreated and possible improvement of hygienic-specific behaviours were the most regularly related factors with the H. pylori infection within this study population.
Association of socio-demographic characteristics, water sources, and habitual practices with H. pylori infection (n = 250).

H. pylori: Helicobacter pylori.
Discussion
In this multicenter cross-sectional cohort of patients with clinically diagnosed gastritis in Northern Pakistan, H. pylori positivity was extremely common. This high prevalence is consistent with findings from other symptomatic populations in Pakistan and neighbouring regions. 19 For instance, recent hospital-based studies have reported H. pylori positivity rates of approximately 86% among patients with gastrointestinal symptoms in Peshawar and nearly 68% among dyspeptic patients in Quetta and Turbat (2023–2024), underscoring the persistently elevated burden of infection within clinical cohorts in the region.20,21
Even though population-based prevalence estimates in the Asia and South Asia are highly varying, recent meta-analysis reports might indicate that the pooled prevalence rate is in the range of about 44%–57% with high disparities by country and study design. 3 Such estimates are quite lower than the prevalence recorded in the current study as it ought to be considering that community-based surveys involve asymptomatic individuals who are less likely to undergo diagnostic evaluation. Our results are, thus, most comparable with the hospital-based studies which have been performed in endemic areas and patients presenting with either a gastritis or dyspeptic symptomatology are naturally enriched in H. pylori infection.22,23
The gastrointestinal symptoms such as epigastric pain, nausea, vomiting, bloating and heartburn that were very common in both the patients with H. pylori-positive as well as those with H. pylori-negative such that there was a strong overlap between the two groups. 24 The observation is consistent with global clinical experience and highlights the limited value of symptom-based differentiation of H. pylori infection, especially in an endemic environment with several gastrointestinal disorders. 25
The application of multiple diagnostic modalities represents clinical practice in the real world but brings about heterogeneity in the classification of infections. Although often used, serologic IgG testing could not consistently differentiate active and past infection and could only be used as a supporting indicator. 26 Because of technical and logistical limitations, culture only took place in a restricted number of patients, which underscore the ongoing challenges of routine culture and antimicrobial resistance testing of H. pylori in the resource-constrained healthcare systems. 27
The identified eradication rate was moderate and in consensus with results reported in other high-burden settings in which traditional treatment regimens often yield suboptimal outcomes. Increasingly, there are signs that clarithromycin-containing triple therapy might fail to work in the parts of the world that have high or even unknown resistance patterns, whereas bismuth-containing quadruple therapy has proven more effective. 28 The results are consistent with the overall issues of persistent infection, treatment failure and reinfection even though the treatment regimens in the given study were a reflection of routine clinical practice and not a standardized regimen in endemic populations.29,30
The lack of statistically significant associations between H. pylori positivity and sociodemographic factors such as age, sex, education level and urban or rural residence also coincides with a number of studies on the regional clinical situation in Pakistan and South Asia. 31 The conventional demographic predictors might not hold much discriminatory power in adult-onset symptomatic groups due to ongoing exposure and early-life acquisition among adult symptomatic populations. 32
It was found that a strong association existed between, H. pylori positivity and untreated drinking water, lack of household water treatment, poor hand hygiene and the intake of uncooked or undercooked food. 33 Such results are biologically viable and are proven by the existing body of research indicating the faecal-orally based routes of transmission of H. pylori in conditions with the discrepant water sanitation and hygiene facilities. 34 Multiple research reports on various countries in Asia such as Vietnam have shown that odds of being infected with H. pylori are reduced in persons who reported regular handwashing, which supports the applicability of hygiene behaviours in endemic contexts.33,35
Dietary habits especially eating uncooked or inadequately handled food have also been cited as a potential transmission routes. Even though the current research did not examine specific food products or microbiological contamination, the determined co-relationship is in line with the accumulating evidence indicating that contaminated fresh food and raw vegetables may act as vectors of transmission in certain environments.36,37 However, since the design is cross-sectional, these exposures should be considered as correlates in a clinical population instead of being considered as conclusive risk factors of acquisition.
Strengths and limitations
The strengths of this study are that it has a multicentre design, standardized data collection, detailed assessment of the environmental and behavioural exposures in a real-world clinical population. Nonetheless, significant constraints should be admitted. This is because the cross-sectional design does not allow causal inference and the sample comprises of patients who have clinically diagnosed gastritis with restriction on the general population. Independence on the self-reported exposures creates the risk of information bias, and diagnostic heterogeneity and low feasibility of culture limit the interpretability. Furthermore, multivariable analyses were not done to identify independent predictors as they are very unstable due to high positivity rates of H. pylori.
Conclusion
Overall, this research study shows that the burden of the infection with H. pylori among patients with clinically diagnosed gastritis in Northern Pakistan is very high and it demonstrates that there are strong associations between environmental and hygienic factors within this selected population. Such results strengthen the role of the context and environmental exposure in the endemic context but should be understood with much caution and without non-causal interpretation. The further longitudinal and community-based research which includes standardized methods of diagnosis and antimicrobial resistance should be conducted in order to improve the understanding of the acquisition patterns, reinfection patterns and the successful preventive measures.
Supplemental Material
sj-docx-1-smo-10.1177_20503121261426073 – Supplemental material for Prevalence and factors associated with helicobacter pylori positivity among patients with gastritis in an endemic region of Pakistan
Supplemental material, sj-docx-1-smo-10.1177_20503121261426073 for Prevalence and factors associated with helicobacter pylori positivity among patients with gastritis in an endemic region of Pakistan by Abdul Rehman Shahid, Hamna Khalid, Hadeeqa Fatima, Noshaba Razaq, Iqra Mehboob, Muqadas Amir, Muhammad Dawood Nazir, Khansa Kaleem and Noof K. Binashikhbubkr in SAGE Open Medicine
Footnotes
Acknowledgements
We gratefully acknowledge the support of NUMS, Wah Medical College, and POF Hospital in facilitating this research.
Ethical considerations
The study was done in compliance with the standards described in the Declaration of Helsinki (2013 revision) and complied with institution and nation ethical guidelines for research on human subjects. Ethical approval for this multicenter study was granted by the Institutional Review Board (IRB) of Wah Medical College for research conducted at Pakistan Ordnance Factories (POF) Hospital, Wah Cantt (Approval No.:
Consent to participate
Informed consent of the participants was obtained in written form. In the case of limited literacy, a consent form was read aloud in the local language and signed by thumb impression by the presence of a witness. In the case of minors, there was written consent by legally authorized representatives. Data anonymity and confidentiality of participants were observed.
Informed consent was provided by all participants once the purpose of the study, the study procedures, and the voluntary nature of participation were described.
Consent for publication
All authors have read and approved the final manuscript.
Author contributions
●
●
●
●
●
●
●
●
●
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The data underlying this article will be made available by the authors upon reasonable request.*
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.