
Abstract
Objectives:
Chronic obstructive pulmonary disease contributes to substantial health and economic burden worldwide. Co-morbid depression and anxiety are highly prevalent in patients with chronic obstructive pulmonary disease. Depressive symptoms in chronic obstructive pulmonary disease are associated with poorer survival, longer hospitalisation and impaired quality of life. Literature on chronic obstructive pulmonary disease is largely derived from high-income countries; yet 90% of deaths related to chronic obstructive pulmonary disease occur in low- and middle-income countries. We aimed to establish the prevalence of anxiety and depression in patients with chronic obstructive pulmonary disease, as well as the association with psychosocial outcomes.
Methods:
This was a cross-sectional study of chronic obstructive pulmonary disease patients attending outpatient primary care clinics in Karachi, Pakistan. The Patient Health Questionnaire-9 was used to assess depression and the Generalised Anxiety Disorder-7 scale was used for the assessment of anxiety. Health-related quality of life was assessed with EuroQol–Five Dimensions, social support with Oslo-3 and social stress with Life Events Checklist. We recruited 293 subjects.
Results:
The prevalence of depression and anxiety in the sample was 51% (n = 149) and 20% (n = 59), respectively. Depressed chronic obstructive pulmonary disease patients reported significantly lower health-related quality of life scores as compared to non-depressed patients. Participants with depression had significantly higher levels of anxiety, less social support, higher social stress and more subjective impairment in quality of life.
Conclusion:
Given the association with reduced social support and increased perceived stress, the role of psychosocial interventions must be explored in improving outcomes of chronic obstructive pulmonary disease patients in Pakistan.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a long-term respiratory disorder characterised by persistent respiratory symptoms including dyspnoea, cough and excessive sputum production.1,2 The pulmonary obstruction in COPD is progressive and not fully reversible.1–3 COPD is a global public health concern attributing to 5% of deaths worldwide. 4 Reported prevalence rates vary from estimates of 251–328 million cases worldwide and high smoking prevalence alongside ageing populations means that rates are expected to continue to rise.4,5 The effects of this long-term condition extend beyond health and well-being to economic sequelae. The projected direct annual costs for people with COPD are expected to increase from £1.50 billon (1.18–2.50) in 2011 to £2.32 billion (1.85–3.08) by 2030 in England. 6 The majority of the literature on COPD is derived from high-income countries; yet 90% of deaths related to COPD occur in low- and middle-income countries (LMICs). 7 There are limited data on the prevalence of COPD in Pakistan; however, a multinational epidemiological study published in 2012 reported prevalence of 2.1% in individuals over the age of 40 years. 8 Distinct processes like high rates of exposure to noxious occupational substances and air pollution may contribute to variance in the aetiology and epidemiology in this setting.
Depression affects more than 300 million people globally and as of 2018 is the leading cause of disability worldwide.9,10 Anxiety disorders are also some of the most prevalent psychiatric disorders, with over 260 million people in the general population affected worldwide. 10 Depression and anxiety are often co-morbid and prevalence rates are increasing, particularly in LMIC. 10 In Pakistan, the prevalence of depression and anxiety is estimated to be between 22% and 60% of the population. 11
Depression and anxiety are associated with poorer health-related outcomes, especially when they are co-morbid with long-term physical health conditions.12–14 These conditions are commonly co-morbid in COPD, to the extent that they should be considered in all patients.15,16 Meta-analyses have commented on the varied prevalence of depression co-morbid with COPD reported in the literature, where estimates range from 24.6% to 27.1%.17,18 Depressed patients are more likely to have episodes of COPD exacerbation compared to non-depressed patients and even mild co-morbid depression is associated with a twofold higher use of emergency hospital resources. 14 Depression and anxiety in COPD are associated with poorer outcomes, increased mortality, more frequent hospital admissions, poorer quality of life and poorer social functioning.14,19 Quality of life is interlinked with depression and anxiety in patients with COPD, 20 where depression is potentially more predictive of functioning and quality of life than lung function alone. 21 Therefore, improvement in quality of life is becoming a major focus of COPD management strategies.
The majority of patients with common mental disorders and COPD reside in LMIC.4,9 There are numerous factors including unemployment, economic and political uncertainty, gender inequality and recent natural disasters that may contribute to the higher prevalence of depression in Pakistan. 11 Understanding how different disease states lead to multimorbidity and impact health-related outcomes is crucial for the development of effective health and social policy. 22 To our knowledge, there is limited literature on co-morbid anxiety and depression and their impact on psychosocial outcomes in patients with COPD from Pakistan. This study aimed to establish the prevalence of anxiety and depression in patients with COPD attending outpatient primary care clinics in Karachi, Pakistan and their association with psychosocial outcomes.
Methods
Design
This is cross-sectional study based on patients with COPD presenting to primary care in Karachi, Pakistan. The study received ethics approval from the Ethics Review Board of Pakistan Institute of Living and Learning (reference no. PILL/ERB/14-11). The study was conducted in accordance with the guidelines of the Declaration of Helsinki.
Patients
Subjects were approached and recruited by trained researchers from four primary care practices in a low-resource area of Karachi, Pakistan. Karachi is Pakistan’s most populous city with over 20 million residents. The Pakistan Institute of Living and Learning has a database of over 500 primary care clinics across Karachi. Research staff approached four primary care centres in Bilal Colony, informing them of the study and all four centres agreed to participate. Typically, primary care physicians (PCPs) in Karachi would see an average of 60 patients a day. Patients with a diagnosis of COPD were referred by the PCPs to research staff. We did not have access to Forced Expiratory Volume 1 (FEV1) scores or data on how COPD diagnosis was confirmed. Consecutive patients were recruited from the primary care clinics on two fixed days of the week when the researchers attended.
The study was conducted between June 2011 and August 2014. Subjects were recruited through consecutive sampling and there was no formal sample size calculation for the study as the primary aim was to establish prevalence of psychiatric co-morbidity in COPD. A total of 500 patients with diagnosis of COPD were referred across four participating primary care practices. Out of those who were approached by the research staff at PCPs, 17.8% (n = 27) could not complete the initial screening process because of time constraints, 62 were unable to participate because of their health status at that time, 58 refused to participate and for 60 patients their family were not willing for them to participate in the study. A total of 293 out of the 500 patients approached consented to take part in the study and completed the assessments (58.6%; see Figure 1). A participant information sheet in the local language was provided to all the participants. Written consent (thumb impression in case of those with no formal education) was obtained from all participants.

Flow of study participants.
The research staff were trained by the authors in the use of the assessment tools. Due to low literacy rates, all participant questionnaires were completed with research staff for standardisation. All assessment tools had previously been used in Pakistan and had already been translated into Urdu. Data on age, sex, marital status, level of education and employment status were collected on a socio-demographic questionnaire.
Assessments
Data were collected using structured questionnaires administered by trained researchers. All researchers were trained in Good Clinical Practice (GCP).
Socio-demographic Questionnaire
The Socio-demographic Questionnaire included information about age, gender, education (seven categories – no formal education, education from religious institute ‘Madrassa’, primary/middle, metric, intermediate, graduate degree and other), marital status (four categories – single, married, separated and widow), family status (extended/nuclear), number of family members, occupation (housewife, professional (doctor, engineer, lawyer, etc.), skilled and unskilled) and monthly income.
Patient Health Questionnaire-9
This instrument is a 9-item screening tool used to measure the severity of depression, having also been validated and widely used as a brief diagnostic tool. 23 Total scores ranging from 1 to 4 indicate minimal depression, 5 to 9 mild, 10 to 14 moderate, 15 to 19 moderately severe and 20 to 27 severe depression. Patient Health Questionnaire-9 (PHQ-9) has been translated and validated for the Pakistani population. 24 PHQ-9 has been used in other studies to assess depression in patients with COPD. 25
Generalised Anxiety Disorder-7
This instrument is a brief 7-item scale used to assess symptoms of Generalised Anxiety Disorder (GAD). 26 Total scores range from minimal anxiety 0–4, mild anxiety 5–9, moderate anxiety 10–14 and severe anxiety 15–21. GAD-7 has been translated and validated for the Pakistani population. 27 GAD-7 has been used in patients with COPD. 28
Oslo-3
This instrument was used as a measure of social support. 29 The Oslo-3 consists of three questions pertaining to relationships with neighbours, friends and family and how easily a person can rely on them for support. Higher scores indicate greater social support. We have previously used this instrument in Pakistan. 30
Life Events Checklist
This 14-item instrument is based on the Quebec Health Survey and was used to measure social stress. 31 This has previously been used in Pakistan. 30 Life events and difficulties were rated categorically as present or not in the previous 12 months.
EuroQol–Five Dimensions
Quality of life was assessed using the EuroQol–Five Dimensions (EQ-5D) (three level EuroQol–Five Dimensions (EQ-5D-3L)). 32 This is an instrument measuring health status as defined by five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The responses to each dimension have three levels of response, ‘no difficulties’, ‘some difficulties’ and ‘extreme difficulties’. The EQ-5D has been widely tested and used in both general population and patient samples and has been translated into over 130 different languages (https://euroqol.org/). We have previously used this in a Pakistani population. 33 The validity of EQ-5D as a measure of quality of life in patients with COPD has been demonstrated in the published literature. 34
Statistics
Statistical analysis was performed using SPSS 23.0 for windows. The analyses examining the association between ‘caseness’ of depression and demographics, anxiety scores, life events, social functioning and health-related quality of life used PHQ-9 as categorical variables with a cut-off of ⩾10 to define ‘caseness’ of depression.35,36 Pearson’s correlation was used to examine the association among continuous variables found to be normally distributed. The Mann–Whitney test was used to compare continuous data that was not normally distributed. Independent sample t-test was used to check the differences between depressed and non-depressed groups with continuous variables when data were normally distributed, for example, GAD-7, OSLO, Life Events Checklist (LECL), EQ-5D and EQ-5D Visual Analogue Scale (VAS). Chi-square and Fisher’s exact tests were used to assess differences between binary and categorical variables.
Results
For those who completed the study assessments, there were no missing data. The prevalence of moderate to severe depression and anxiety scores in the sample was 51% (n = 149) and 20% (n = 59), respectively (Table 1). The prevalence of depression in males with COPD was 39.7% (n = 29) and in females 54.5% (n = 120).
Prevalence of depression and anxiety.
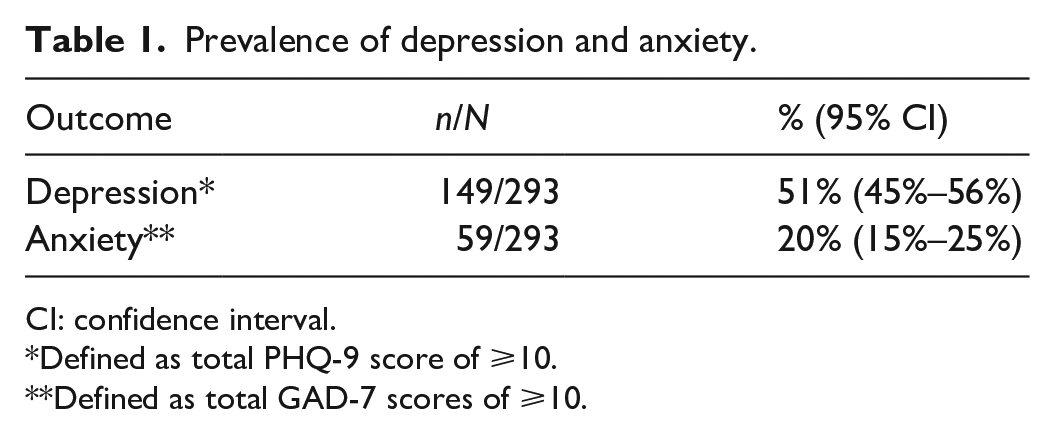
CI: confidence interval.
Defined as total PHQ-9 score of ⩾10.
Defined as total GAD-7 scores of ⩾10.
The mean age of the sample was 43.28 years (standard deviation (SD) = 10.96), and a significant association was found between age and depression with depressed patients being older (Table 2). The majority of participants (n = 127; 43.3%) were between 36 and 45 years of age. The sample consisted of mostly females (n = 220; 75.1%). Females proportionally reported more depressive symptoms than males. The majority of females were housewives and belonged to an extended family system. Depression (p = 0.142) and anxiety (p = 0.095) were not found to be significantly associated with reduced income. A statistically significant difference between education levels in the depressed and non-depressed groups was not found (p = 0.525) (Table 2). A statistically significant difference in education levels was found between anxious and non-anxious participants, with anxious participants having lower educational attainment (p = 0.017) (Table 3).
Characteristics of the sample comparing ‘non-depressed’ and ‘depressed’.

SD: standard deviation; IQR: interquartile range.
Fisher’s exact test.
Chi-square test.
Mann–Whitney U test.
Characteristics of the sample comparing ‘non-anxious’ and ‘anxious’.
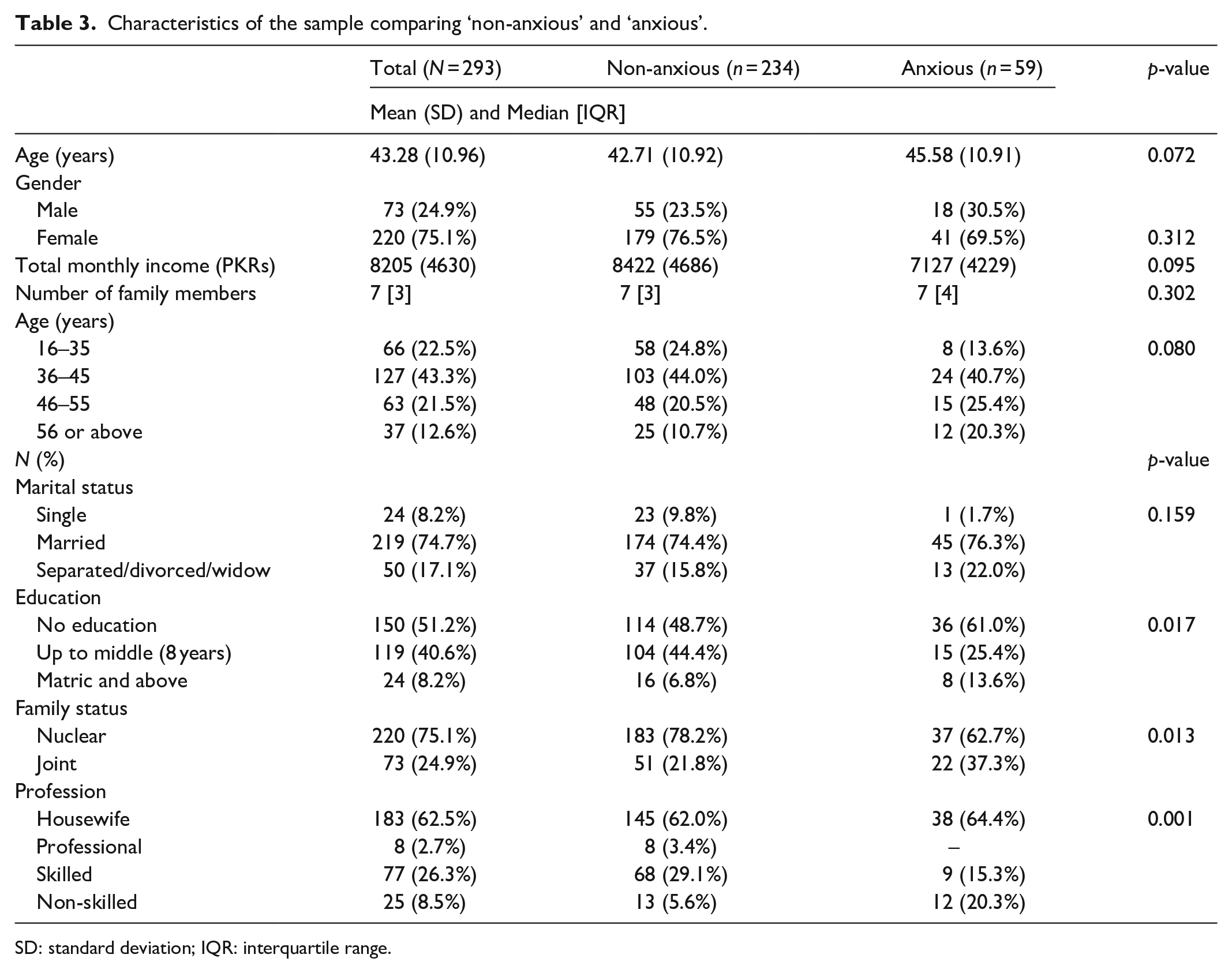
SD: standard deviation; IQR: interquartile range.
Table 4 summarised the average difference between the GAD-7, OSLO, LECL, EQ-5D VAS and EQ-5D in depressed and non-depressed groups. Participants with depression had higher GAD-7 scores, lower OSLO scores, higher LECL scores and lower EQ-5D scores. There were significant mean differences between groups and GAD-7, PHQ-9, LECL and EQ-5D scores, and these were highly associated. Further analysis adjusting the models for age also highlighted significant differences between the depressed and non-depressed groups. Even when controlling for possible influences of age, gender and marital status, the significant differences due to depression were still present. There was positive correlation between total depression scores and GAD-7 (r = 0.675). An additional set of analysis examined the association between anxiety and PHQ-9, LECL, OSLO and EQ-5D (Table 5). Participants with anxiety had higher scores of PHQ-9 (r = 0.675), lower OSLO scores (r = −0.162), higher LECL scores (r = 0.257), lower EQ-5D (r = −0.338) and lower EQ-5D VAS (r = −0.334).
Association between depression and psychosocial outcomes.

GAD-7: Generalised Anxiety Disorder-7; LECL: Life Events Checklist; EQ-5D: EuroQol–Five Dimensions; VAS: Visual Analogue Scale.
Independent sample t-test.
Pearson’s correlation.
Association between anxiety psychosocial outcomes.

PHQ-9: Patient Health Questionnaire-9; LECL: Life Events Checklist; EQ-5D: EuroQol–Five Dimensions; VAS: Visual Analogue Scale.
Independent sample t-test.
Pearson’s correlation.
Approximately half of participants had moderate to severe scores of depression (50.8%). Whereas the majority of the participants had mild anxiety scores (52.9%) (Table 6).
Depression and anxiety severity.

PHQ-9: Patient Health Questionnaire-9; GAD-7: Generalised Anxiety Disorder-7.
Discussion
There are established lines of evidence delineating co-morbidity of common mental disorders in patients with long-term conditions. COPD is a severe and enduring illness with catastrophic consequences on quality of life and general function. Depression and anxiety are often co-morbid conditions that can have a detrimental effect on social functioning and quality of life. Due to a confluence of factors, potentially including, unemployment, gender inequality, political instability and recent natural disasters, depression is more prevalent in Pakistan than other LMICs. 11 The majority of literature related to these co-morbidities emerges from high-income settings. To our knowledge, this is one of the few studies exploring the co-morbidity of depression and anxiety in patients with COPD, and the impact on a number of psychosocial outcomes from Pakistan. The prevalence of depression in our sample was 51%, which is comparable to the prior reported rate of 57.2% from respiratory clinics in Karachi, Pakistan. 37 The slight variation in prevalence rate may be due to the use of the Hospital and Anxiety Depression Scale and recruitment from secondary care in the previously published study. We found that participants with COPD who had a probable ‘caseness’ of depression were more likely to report higher levels of stress, less perceived social support and more subjective impairment in health-related quality of life.
Social stress
Anxiety and depression among COPD patients are intrinsic sources of stress provoked by physical symptoms such as breathing difficulties. 21 However, extrinsic stressors such as life events have also been reported to be associated with depression and poor quality of life in this population. 38 A recent longitudinal study reported that almost half of COPD patients reported to have experienced events that were stressful and significantly impacted their lives. 39 This study highlighted similar findings where depressed COPD patients had reported more perceived stressful life events when compared to non-depressed patients.
Social support
Social support is important for patients with chronic illnesses as it can contribute to improved self-care and self-management of disease, which can lead to improved health outcomes. 40 The findings for this study indicate that depressed COPD patients reported poor social support when compared to their non-depressed counterparts. Qualitative data from focus group discussions of patients with Asthma and COPD suggest that participants experienced lack of social support from family, friends and colleagues leading to feelings of sadness, anger and in some cases social isolation. 41 Evidence from quantitative studies supports the notion that higher social support is associated with better physical activity and higher level of participation in rehabilitation in patients with COPD. 42 Evidence also supports that COPD patients with limited social/emotional support are more likely to report depression and poor health-related quality of life. 43
Quality of life
Participants in this study who met ‘caseness’ for depression were more likely to report impaired health-related quality of life. The association between COPD and quality of life has been investigated in Pakistan, with Baloch et al. 44 reporting that exacerbation of COPD was associated with impaired quality of life. Prospective cohort data from elsewhere also support the association between increasing respiratory symptoms and deterioration in quality of life. 45 To our knowledge, there are limited published data from Pakistan exploring the associations between co-morbid depression and quality of life in patients with COPD. The impact of exacerbation of COPD on quality of life has previously been reported and depression was recognised as an important factor contributing to quality of life in patients with COPD. 21 Meta-analysis of longitudinal cohort studies and a recent narrative review indicates that both depression and anxiety predict health-related quality of life and this association is more pronounced with co-morbid depression than anxiety.19,46 Although causality cannot be inferred, our current findings raise the possibility that depressive symptoms may represent a modifiable risk factor in improving functioning and health-related quality of life in patients with COPD.
Age and gender differences
Our sample was relatively young with 65% of the participants being under the age of 45 years. The published literature from Pakistan has previously described a younger demographic with COPD. 43 A recently published cross-sectional study reported that over 70% patients with COPD in their sample were between the ages of 18 and 41 years. 47 Occupational exposure from coal mines, agriculture, welding and air pollution may contribute to a younger age of onset of COPD in Pakistan. 47 There are brick kilns and cement factories in the surrounding areas of where our sample was recruited. There was a female predominance in our sample, accounting for more than 75% of participants. This could also potentially be explained by the contribution of exposure. Exposure to biomass smoke in poorly ventilated homes contributes to higher risk in females developing COPD in LMIC. 48 Wider literature indicates that the prevalence and disease burden of COPD affects males and females equally.49,50 However, being female is a risk factor for the development of depression in patients with early COPD. There is also a female predominance in COPD with regard to the risk of developing anxiety disorders with manifestations such as phobic disorder, panic disorder and generalised anxiety disorder.51–54 Worldwide, the prevalence of depression is higher in females, potentially indicating that the differential risk may be attributed to biological differences. 55
Strengths and limitations
There are a number of limitations which must be considered when interpreting the findings of this study. Given the cross-sectional design, a causal relationship between variables cannot be concluded. In addition, although the patients were referred with confirmed diagnosis of COPD by PCPs, we did not have access to data on diagnostic measures used for confirmation of COPD diagnosis. Our inability to assess for severity of COPD is also a major limitation of this study, and we could not ascertain the correlation of depression and anxiety with severity of COPD. The lack of data on medication and treatment of psychiatric co-morbidity is another limitation. Despite the fact that 42% of patients initially approached for screening did not participate in the study, we were able to recruit a relatively large sample of participants. However, a formal sample size calculation was not performed for this study and subjects were recruited through consecutive sampling. We have no ability to compare differences in those who agreed to participate in the study and those who did not. We also acknowledge that the overrepresentation of females in our sample limits the generalisability of our findings even within this setting. Although we did not use a gold standard interview to confirm ‘caseness’ of depression and anxiety, we did use instruments that have been validated in this population. However, instruments used were self-report measures, and therefore liable to reporter bias.
Conclusion
Depression and anxiety are commonly co-morbid in patients with COPD. Depression and anxiety are important predictors of outcomes in COPD. Recognition and management of depression and anxiety in COPD may improve outcomes and potentially decrease health service utilisation, which is pertinent in a setting like Pakistan where resources are scarce. Less than 1% of health budgets are allocated to mental health delivery; therefore, the role of primary care and respiratory physicians is crucial in identifying these patients. Screening tools could be used routinely by physicians. Given the association with reduced social support and increased perceived stress, the role of psychosocial interventions must be explored in improving outcomes. There is a need for future trials investigating the feasibility of psychosocial interventions in treating psychiatric co-morbidity for COPD patients in Pakistan.
Footnotes
Acknowledgements
The authors thank all participants in the study and staff at recruitment centres for their support and contribution.
Author contributions
The idea of the study was conceived by I.B.C. and N.H. N.H. and I.B.C. shared responsibility for the training and supervising researchers as well as preparing the manuscript. M.O.H. and M.A.H. contributed to the interpretation of results and drafted the manuscript. F.J. and T.K. contributed to recruitment of participants and carrying out assessments. T.K. also contributed to the drafting of the manuscript. S.S. and S.L. contributed to statistical analysis. A.B., R.M. and M.P. made intellectual contribution to the interpretation and assisted in writing of the manuscript. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I.B.C. and N.H. have given lectures and advice to Eli Lilly, Bristol Myers Squibb, Lundbeck, AstraZeneca and Janssen pharmaceuticals for which they or their employing institution have been reimbursed. I.B.C. and N.H. were previously trustees of the Pakistan Institute of Living and Learning. N.H. is the Chair of Board of Trustees of Manchester Global Foundation. N.H. is a past Trustee of The Pakistan Institute of Living & Learning (PILL), Abaseen Foundation UK and Lancashire Mind UK. N.H. is the Chair of Board of Trustees of Manchester Global Foundation (MGF), a Charitable Incorporated Organisation (CIO) registered in England and Wales. He is a board member of the executive committee for the Faculty of Academic Psychiatry, at the Royal College of Psychiatrists, London. N.H. has received honorarium and travel grants from various pharmaceutical industries. I.B.C. has given lectures or advice to Eli Lilly, Bristol Myers Squibb, Lundbeck, AstraZeneca and Janssen pharmaceuticals for which he or his employing institution have been reimbursed, outside the submitted work, and Professor I.B.C. was previously trustee of the Pakistan Institute of Living and Learning (PILL).
Ethics approval
The study received ethics approval from the Ethics Review Board of Pakistan Institute of Living and Learning (reference no. PILL/ERB/14-11).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Pakistan Institute of Living and Learning under grant (PILL-COPD-012/2010). The design conduct and analysis of the study were completely independent of the funder. The content is solely the responsibility of the authors and does not necessarily represent those of the funder.
Informed consent
Written informed consent was obtained from all subjects before the study.
Data sharing
The corresponding author of the study can be contacted to request data of this study for further analysis from this study.