
Abstract
Background:
Dysmenorrhea is a common menstrual health problem among adolescents, often managed through pharmacological and non-pharmacological strategies. However, the factors that predict adolescents’ choice between these management approaches remain poorly understood, particularly in settings where traditional and modern practices coexist. This study examined the predictors of pharmacological and non-pharmacological management practices among school-going female adolescents in Ghana.
Methods:
A cross-sectional survey was conducted among 490 female students aged 13–24 years in 2 senior high schools within the Effutu and Agona West Municipalities. Participants were recruited using simple random sampling. For minors (aged 13–17 years), written informed consent was obtained from Legally Authorized Representatives and written assent from participants; adult participants (aged 18–24 years) provided written informed consent directly. Exclusion criteria included diagnosed gynecological disorders, inability to provide informed assent or parental/guardian consent, and cognitive impairments. Data were collected using a structured questionnaire and analyzed with chi-square tests and logistic regression.
Results:
The prevalence of dysmenorrhea was 82.4%. Pharmacological management was significantly associated with dysmenorrhea experience (χ2 = 11.51, p = 0.003). Pain intensity emerged as a strong predictor, with adolescents reporting moderate (Exp(B) = 1.7, p = 0.03) and severe pain (Exp(B) = 2.42, p < 0.01) more likely to use medications. Non-pharmacological practices were significantly associated with program of study (χ2 = 28.75, p = 0.001), while demographic factors showed no significant associations.
Conclusion:
Pain severity drives pharmacological management, whereas educational exposure influences non-pharmacological choices. Comprehensive menstrual health education is needed across academic programs to promote effective, evidence-based management of dysmenorrhea among adolescents in Ghana.
Introduction
Dysmenorrhea, defined as painful menstrual cramps originating from uterine contractions, is one of the most prevalent gynecological concerns affecting adolescent girls and young women globally. 1 Primary dysmenorrhea occurs in the absence of pelvic pathology and typically begins within 3 years of menarche, often persisting throughout adolescence. 2 The condition has gained increasing attention in global adolescent health discourse due to its widespread prevalence and its significant physical, psychological, and social implications for young people.3,4
In many low- and middle-income countries, including those in sub-Saharan Africa, menstrual health remains insufficiently prioritized within adolescent health programming. Limited access to menstrual health information, inadequate pain-management resources, and persistent cultural taboos surrounding menstruation continue to affect adolescent girls’ ability to manage menstrual pain effectively.5,6 These challenges are particularly critical in school settings, where menstrual health directly influences girls’ daily functioning and educational experiences.
Globally, the prevalence of dysmenorrhea among adolescents ranges from 45% to 95%, depending on assessment tools and diagnostic criteria used in different studies. 3 Systematic reviews consistently show that more than 80% of adolescent girls experience dysmenorrhea, though with substantial regional variation. 4 In sub-Saharan Africa, recent evidence underscores dysmenorrhea as a major yet under-recognized public health issue. Studies in Ghana report prevalence rates between 70% and 85% among adolescent girls—higher than many global estimates.7,8 Although national initiatives such as the Ghana Health Service’s Adolescent Health Strategy (2016–2020) and the School Health Education Programme (SHEP) Policy (2022) have acknowledged menstrual health as a critical priority, implementation of comprehensive menstrual health education remains inconsistent, particularly in rural and peri-urban schools.9–11
The consequences of dysmenorrhea extend beyond physical discomfort, affecting academic performance, psychosocial well-being, and participation in daily activities. Adolescents with dysmenorrhea commonly experience school absenteeism, reduced concentration, lower academic participation, and overall diminished educational outcomes.12–16 In Ghana, a recent survey reported that one-third of girls with dysmenorrhea missed school due to menstrual pain, losing up to one to three school days monthly. 14 The condition also affects adolescents’ quality of life, limiting participation in sports, social interactions, and extracurricular activities, while contributing to heightened stress, anxiety, and depressive symptoms.17–21 Cultural stigma surrounding menstruation may further restrict help-seeking and exacerbate both physical and psychological burdens.22,23
Multiple factors influence how adolescents manage dysmenorrhea. Pharmacological methods—including nonsteroidal anti-inflammatory drugs (NSAIDs) and hormonal contraceptives—remain the main evidence-based approaches, although access, affordability, and knowledge gaps frequently limit their use among Ghanaian adolescents.24–28 Nonpharmacological strategies range from heat therapy, exercise, and dietary adjustments to herbal and indigenous remedies such as Aframomum melegueta, ginger, and Ocimum gratissimum, which are commonly used in many Ghanaian communities.29–31 Despite the availability of these varied options, knowledge among healthcare workers and community pharmacists regarding adolescent-friendly dysmenorrhea management remains inconsistent, often resulting in inadequate counseling and support for affected adolescents.32,33
However, despite the substantial impact and high prevalence of dysmenorrhea, important knowledge gaps remain unaddressed. Existing studies in Ghana have largely focused on prevalence and general management patterns, with very limited empirical examination of the determinants influencing adolescents’ choice between pharmacological and nonpharmacological management approaches. Research has not sufficiently explored how pain characteristics (such as intensity and frequency), demographic factors, cultural influences, or exposure to academic programs shape the management strategies adopted by adolescents. Furthermore, the interplay between modern medical approaches and traditional practices in Ghana remains poorly documented. Little is also known about how students’ academic program of study—which may influence health literacy and exposure to health-related information—affects their dysmenorrhea management choices.
This study addresses these critical gaps by examining predictors of both pharmacological and nonpharmacological management practices among school-going female adolescents in the Central Region of Ghana. Using an ordinal logistic regression framework, the study differentiates predictors across management categories rather than treating dysmenorrhea management as a single, uniform behavior. The research focuses on adolescents—a population often overlooked in menstrual health research—and provides insights not previously documented in Ghana.
The findings of this study have important implications for strengthening adolescent menstrual health programming in Ghana and similar contexts. The evidence generated can support the design of targeted educational interventions that reflect the diverse needs of adolescents across different academic programs, ensuring that menstrual health information is both relevant and accessible. By identifying the specific subgroups of adolescents who require greater support in managing dysmenorrhea, the study provides practical guidance for school health coordinators, community health nurses, and healthcare providers. Additionally, the results contribute to the development of pain-severity-sensitive management guidelines that can be integrated into school health services to improve timely, appropriate, and safe pain management. Beyond its immediate relevance, this research offers baseline data that can inform and strengthen the long-term implementation of the SHEP and other national adolescent health initiatives. By embedding menstrual health education and dysmenorrhea management strategies into existing school and community health structures, the findings promote sustainable, low-cost, and scalable approaches that can enhance adolescent well-being and support progress toward Sustainable Development Goal 3 (good health and well-being).
Materials and methods
Study design
This study employed a cross-sectional survey design to investigate the association between the experience of dysmenorrhea and the management practices (pharmacological and nonpharmacological) employed by adolescent girls in senior high school (SHS). This design is appropriate for assessing the prevalence of dysmenorrhea and examining associations between various factors and management practices at a single point in time12,34.
Study setting
The study was conducted in two selected SHSs in the Effutu and Agona West Municipalities in the Central region of Ghana. The Effutu and Agona West municipalities are 2 of the 22 Municipal districts in the Central Region and serve as local government areas. There are a total of four SHSs in Efutu Municipality and eight SHSs in Agona West Municipality. For this study, one SHS from each municipality was purposively selected based on geographical accessibility, administrative willingness to collaborate, and having a sufficient female student population to meet the study’s sample size requirements. This purposive selection was done in consultation with the Municipal Education Offices and school authorities to ensure logistical feasibility and institutional support.
Study population and sampling techniques
The study population consisted of female adolescents in SHSs within the Effutu and Agona West Municipality of Ghana. The study included female students aged 13–19 years who were enrolled in the selected SHSs and were experiencing menstruation. The study excluded students who were diagnosed with gynecological disorders (e.g., endometriosis, polycystic ovary syndrome), those unable to provide informed consent (for participants ⩾18 years) or informed assent with consent from legally authorized representatives (for participants <18 years), and those with cognitive impairments that prevent them from understanding and completing the questionnaire. The identification of students with gynecological disorders was implemented through a self-reporting mechanism, where a section in the questionnaire requested participants to provide information about their previous medical diagnoses. Participants were asked to indicate if they had been formally diagnosed with conditions such as endometriosis, polycystic ovary syndrome, and uterine fibroids, and were instructed to discontinue participation in the study if any of these conditions were disclosed. The multistage sampling approach incorporated stratified random sampling to ensure appropriate representation of the adolescent population. Grade stratification was implemented to ensure representative distribution, with participants initially divided into three strata based on academic forms: Form 1, Form 2, and Form 3. Proportional allocation was used to determine the number of participants from each grade stratum. Within each grade stratum, simple random sampling was employed using complete class registers as the sampling frame. A manual lottery technique was instituted, where students’ names were written on separate pieces of paper, mixed, and randomly selected until the desired sample size for each grade was achieved. This technique also helped to prevent bias or prejudice on the part of the researcher. 35
Sample size calculation
The sample size was computed using Yamane’s formula, 36 which is suitable when dealing with large, finite populations where it is impractical to survey the entire population due to time, cost, or logistical constraints. The formula is expressed as follows:

n is the sample size
N is the estimated study population size
e is the level of precision.
For this study, the following assumptions were applied:
Margin of error (e): 0.05 (5%), representing a 95% confidence level.
Total population (N): 1340 female adolescent students across both schools.
Confidence level: 95%, corresponding to the standard precision level for cross-sectional studies.
Using proportional allocation, the sample size was calculated separately for each school based on their respective student populations.
For A.M.E Zion Girls Senior High School
Population of adolescent girls (N) = 523
Applying the formula:

n = 523/(1 + 523(0.0025)).
n = 523/(1 + 1.3075).
n = 523/2.3075.
n = 226.65 ≈ 227 participants.
For Swedru Senior High School
Population of adolescent girls (N) = 817.
Applying the formula:

n = 817/(1 + 817(0.0025)).
n = 817/(1 + 2.0425).
n = 817/3.0425.
n = 268.53 ≈ 269 participants.
The summation of the two sample sizes was 496 (227 + 269). Anticipating a potential attrition or nonresponse rate of 10%, the target sample was adjusted to 546 participants. However, 543 questionnaires were ultimately distributed, of which 490 were completed and returned, yielding a response rate of 90.2%. These 490 completed questionnaires were used for data analysis.
Design of instrument and data collection
Items in the study instrument were adapted following a comprehensive review of literature on pharmacological and nonpharmacological management practices among female adolescents and youth, which helped identify relevant items and scales from existing questionnaires. The final questionnaire was subsequently developed based on these related studies.37–39 Five experts with diverse expertise in adolescent reproductive health, research on menstrual disorders, adolescent health research, questionnaire design and validation, and statistical analysis of health research were consulted to assess the content and face validity of the questionnaire. These experts assisted in selecting the most appropriate questions from the adopted studies, ensuring the instrument’s comprehensiveness and relevance. Minor textual adjustments were made to suit the focus of this study, without any major changes to the study instrument. The first part of the questionnaire dealt with demographic characteristics, such as age group, program of study, age at menarche and level of study. The second part of the questionnaire (three items) dealt with knowledge and experiences of dysmenorrhea. The third and fourth sections each comprising seven items, encompassed questions relating to pharmacological and non-pharmacological practices with response options “Yes,” “No,” and “Don’t Know.” The complete study instrument is available in the Supplementary Material.
The questionnaire administration was facilitated by the author and two trained research assistants. Before this, institutional permission was obtained from the headmistress/headmasters and the educational directorate at the municipality. To minimize interference in their academic activities, students were approached while changing lessons or while waiting for the next course instructor. Further permission was sought from the course instructors. Explanation was provided to intact class groups for each selected grade (Form 1, Form 2, and Form 3). Each class group was briefed collectively during a designated time allocated by the school administration. Explanations were given during a single dedicated session within school hours. Research team members provided standardized verbal explanations covering study objectives, voluntary participation, confidentiality assurances, consent and assent procedures, and questionnaire completion instructions. Further clarification was provided to those who needed it. Those who satisfied the inclusion criteria were given the questionnaire to complete after appropriate consent procedures. For minor participants (aged <18 years), written informed consent was obtained from their legally authorized representatives (parents, legal guardians, or in loco parentis school authorities for boarding students), and written assent was obtained from the minor participants themselves. For adult participants (aged ⩾18 years), written informed consent was obtained directly from the participants. In the context of boarding schools where parents were not immediately accessible, school authorities (headmasters/headmistresses) served as legally authorized representatives in loco parentis, as recognized under Ghanaian educational law. All consent and assent procedures were completed before questionnaire administration.
The research team gave the respondents privacy to complete filling the questionnaire. The female adolescents were required to complete questionnaires independently in a single, supervised session with adequate spacing to ensure privacy. Those unable to finish within the initial time were provided alternative time slots on the same day, either in the original classroom or a designated quiet room, under continuous research team supervision. These measures were implemented to prevent peer influence and maintain the confidentiality and integrity of the respondents’ answers. Data collection lasted for a period of 3 months, between September and December 2023.
Study variables
Pharmacological management practices
This was a dependent variable, specifically addressing the utilization of medications or drug-based interventions in managing the condition of interest. The questionnaires sought information on the types of medications used, including opioid analgesics, NSAIDs, oral contraceptives, and muscle relaxants. The questionnaire also inquired about the use of over-the-counter medications, self-injections, and intravenous fluids. Responses were recorded using a scoring system, where “Yes” was assigned a value of 1, and both “No” and “Don’t know” were assigned a value of 0. The level of pharmacological practices was scored, graded out of 100% and categorized into least practiced, moderately practiced, and highly practiced.
Nonpharmacological management practices
This was also a dependent variable, encompassing nonpharmacological interventions used to manage the condition. The assessment of this variable involved determining the use of lifestyle modifications, including dietary changes, physical activity, and stress management techniques. Responses were scored using a system where “Yes” was assigned a value of 1, while both “No” and “Don’t know” were assigned a value of 0. The level of nonpharmacological practices was scored and categorized into least practiced, moderately practiced, and highly practiced.
Experiences of dysmenorrhea
To assess the independent variable—experiences of dysmenorrhea—the questionnaire captured information on its occurrence, frequency, and intensity among participants. A series of structured questions were used. First, participants were asked, “Do you experience dysmenorrhea?” with response options “Yes” or “No,” to determine the proportion of adolescents reporting menstrual pain. Second, participants were asked, “How often do you experience dysmenorrhea?” with response options “every menstrual period,” “every 2–3 months,” “every 4–6 months,” and “once a year,” to assess frequency. Finally, pain intensity was measured by asking participants to rate their pain on a numerical scale from 1 to 10, with scores of 1–3 indicating mild pain, 4–7 indicating moderate pain, and 8–10 indicating severe pain.
Validity and reliability of the instrument
A pretest was conducted using 40 questionnaires administered to randomly selected female students from Winneba Senior High School, a different institution within the municipality. The school has a total population of 850 female adolescents, and therefore, the 40 participants involved in the pretest represent approximately 4.7% of the target population. The purpose of the pretest was to evaluate the adequacy of the questionnaire and identify areas requiring adjustment, such as the addition or removal of items. The results indicated that the instrument was capable of generating sound, consistent, and relevant data to address the study objectives. To further strengthen validity, the questionnaire underwent expert review in addition to the pretest, which together established its face and content validity. These processes ensured that the items were clear, comprehensive, and aligned with the intended constructs of the study. The pilot sample was not included in the main study.
Data analysis
Data were entered, cleaned, and analyzed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). Each participant obtained a raw score ranging from 0 to 7 for their choice of pharmacological and nonpharmacological practices. To ensure ease of interpretation and uniform categorization, these scores were standardized into percentages using the formula: standardized score = (raw score ÷ 7) × 100. Based on the standardized scores, participants were classified into three groups: least practiced (0–39), moderately practiced (40–79), and highly practiced (80–100).
Descriptive statistics were used to summarize the results, with frequencies and percentages reported for categorical variables and means for continuous variables. To examine associations between dependent and independent variables, chi-square tests of independence were performed. Variables that showed an association were further analyzed using regression models to determine effect sizes, with statistical significance set at p < 0.05.
For multivariate analysis, an ordinal logistic regression model—also known as the proportional odds model (POM)—was fitted, given that the dependent variable (management practices) had three naturally ordered categories (least, moderate, and high). Independent variables with p-values ⩽0.50 in the bivariate analysis were included in the POM. The final results were presented using odds ratios (Exp(B)), standard errors, p-values, and 95% confidence intervals (CI). 40
Ethical considerations
Ethical approval was obtained from the Ghana Health Service Ethics Review Committee (GHS-ERC: 004/07/24). A formal letter of introduction from the University was also submitted to the management of the two selected SHSs to secure institutional permission prior to data collection. The study adhered strictly to the ethical principles outlined in the Declaration of Helsinki, including beneficence, protection from harm, and justice. A two-tiered consent process was implemented based on participants’ age. For minor participants (aged <18 years), written informed consent was obtained from their legally authorized representatives (parents, legal guardians, or school authorities acting in loco parentis for boarding students), and written assent was secured from the minor participants themselves. For adult participants (aged ⩾18 years), written informed consent was obtained directly from the participants. All participants were informed of their right to withdraw from the study at any time without penalty. Participation was entirely voluntary, and confidentiality was maintained throughout the study by using coded identifiers rather than personal identifying information. All consent and assent forms were reviewed and approved by the GHS-ERC prior to study implementation.
Results
Sociodemographic information of participants
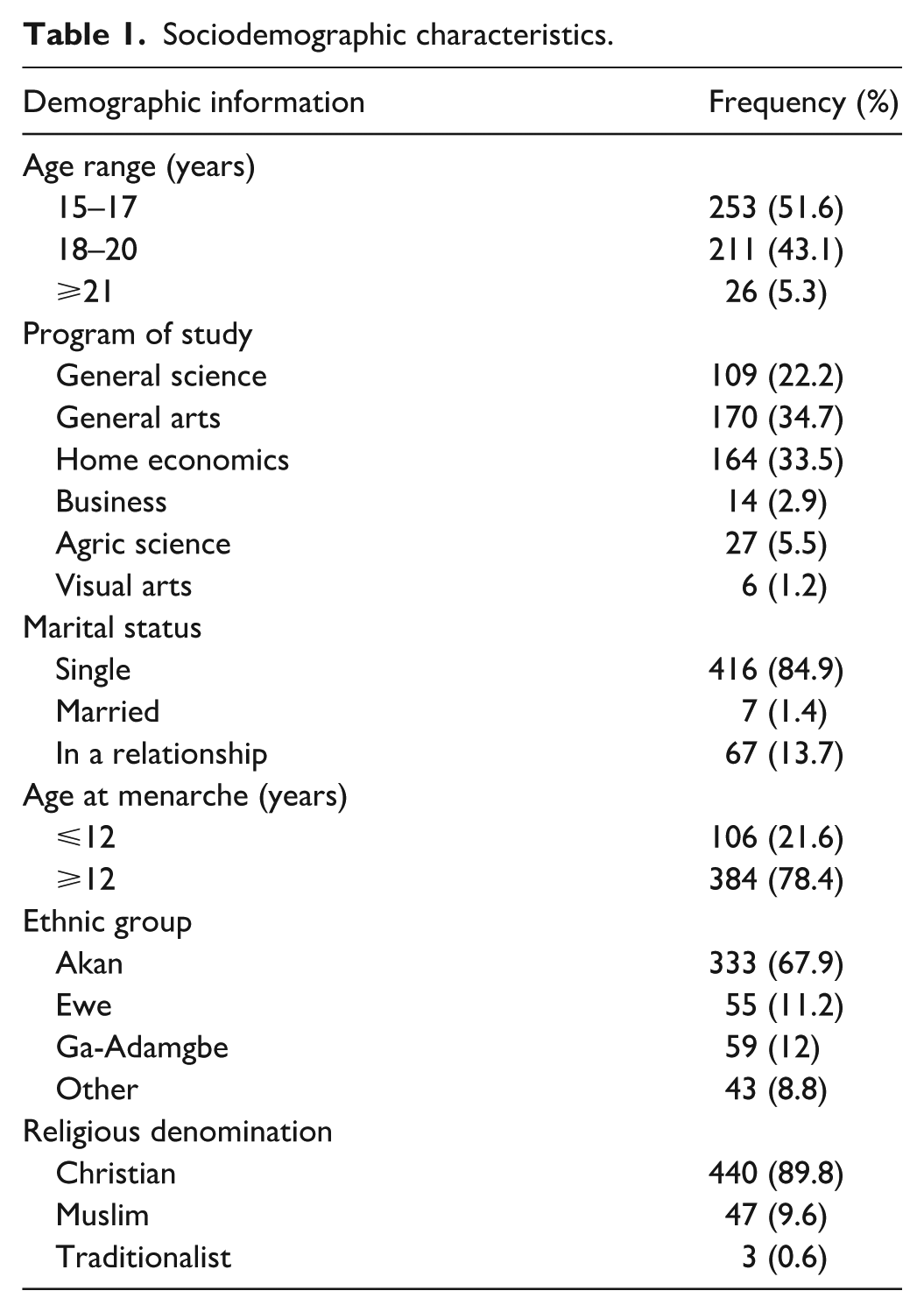
Of the 543 questionnaires distributed, 490 were completed and returned, yielding a response rate of 90.2%. The analyses were therefore based on 490 responses. Participants were predominantly aged 15–20 years (51.6%), with the majority enrolled in general arts (34.7%), home economics (33.5%), or general science (22.2%) programs. Most were single (84.9%), experienced menarche after age 12 (78.4%), and identified as Akan (67.9%) and Christian (89.8%). Full demographic characteristics of the participants are presented in Table 1.
Sociodemographic characteristics.
Experience of dysmenorrhea
The results presented in Table 2 show that overall, 82.4% of participants reported experiencing dysmenorrhea, while 17.6% did not. Among those affected, most (76.3%) experienced pain during every menstrual period, 13.3% reported it every 2–3 months, 4.7% every 4–6 months, and 5.2% only once a year. In terms of pain intensity, 31.7% rated their pain as mild (scores 1–3), 43.1% as moderate (4–7), and 25.2% as severe (8–10).
Experience of dysmenorrhea.

Pharmacological and nonpharmacological management practices of Dysmenorrhea
The study also examined participants’ use of pharmacological and nonpharmacological strategies in managing dysmenorrhea. Levels of practice were categorized as least, moderate, or high. For pharmacological management, 233 participants (57.7%) fell into the least practiced category, 157 (38.9%) were moderately practiced, and 14 (3.5%) were highly practiced, with a mean practice score of 35.68. In contrast, for nonpharmacological management, 155 participants (38.4%) were least practiced, 219 (54.2%) were moderately practiced, and 30 (7.4%) were highly practiced, with a higher mean practice score of 43.14. Detailed results are presented in Figure 1.

Management practices of dysmenorrhea. Note: 0–39 = least, 40–79 = moderately, 80–100 = highly.
Association between predictors and dysmenorrhea management practices
A Chi-square test of independence was conducted to examine associations between the predictor variables and management practices of dysmenorrhea, both pharmacological and nonpharmacological. Results presented in Table 3 indicate that the intensity of dysmenorrhea was significantly associated with pharmacological management practices (χ2 = 13.12, p = 0.001). Similarly, the frequency of dysmenorrhea showed a statistically significant association with pharmacological management (χ2 = 2.33, p = 0.03). For nonpharmacological management practices, only the program of study demonstrated a significant association (χ2 = 4.39, p = 0.001). Demographic factors such as age, marital status, and ethnicity were not significantly associated with either form of management (p > 0.05).
Association between predictor variables and management practices of dysmenorrhea (pharmacological and nonpharmacological management).

Factors influencing the management practices of dysmenorrhea
An ordinal logistic regression analysis was conducted to determine factors influencing the management practices of dysmenorrhea, both pharmacological and nonpharmacological practices. Two different models were fitted as there were two dependent variables (pharmacological management practices and nonpharmacological management practices). The two models were statistically significant as indicated by the final models’ chi-square test (χ2 = 31.92, p < 0.001) and (χ2 = 25.13, p < 0.001) for pharmacological and nonpharmacological practices, respectively. The odds ratios (exp(B)) for the final models were interpreted in the results. The results presented in Table 4 show that, for pharmacological management practices, age group comparisons revealed that participants aged ⩾20 years had 2.29 times higher odds of practicing pharmacological management compared to the reference group (15–17 years), though this association was not statistically significant (p = 0.13; 95% CI [0.79, 6.67]).
Factors influencing dysmenorrhea management practices (pharmacological and nonpharmacological).

Exp(B): exponentiated B coefficient; SE: standard error; CI: confidence intervals.
Regarding the program of study, business students demonstrated significantly higher odds of pharmacological management compared to general science students (Exp(B) = 3.78, p = 0.03; 95% CI [1.10, 13.05]), while visual arts students showed marginally nonsignificant increased odds (Exp(B) = 4.44, p = 0.10; 95% CI [0.75, 26.22]).
Frequency of dysmenorrhea experience was also significant; participants experiencing pain every 2–3 months were 57% less likely to undertake higher pharmacological management practices compared to those experiencing pain every menstrual period (Exp(B) = 0.47, p = 0.03; 95% CI [0.24, 0.94]). Pain intensity was a significant factor as well, with moderate pain increasing the odds of engaging in higher pharmacological management practices by 70% (Exp(B) = 1.70, p = 0.03; 95% CI [1.04, 2.88]) and severe pain further increasing the odds by 142% (Exp(B) = 2.42, p < 0.01; 95% CI [1.36, 4.31]) compared to mild pain. Other factors such as marital status and age groups (18–20 years) did not demonstrate statistically significant associations with either management (p > 0.05).
For nonpharmacological management practices, the program of study emerged as a significant factor for Agric Science students, who had significantly lower odds (0.25) of practicing higher non-pharmacological management compared to general science students (Exp(B) = 0.25, p < 0.01; 95% CI [0.09, 0.66]). Frequency of dysmenorrhea and pain intensity did not show any significant associations with nonpharmacological management practices (p > 0.05).
Discussion
The study found that a high percentage (82.4%) of participants experienced dysmenorrhea, which is consistent with previous research that has reported the prevalence of dysmenorrhea to be between 50% and 90% among women of reproductive age.41,42 This high prevalence underscores the significance of dysmenorrhea as a common gynecological condition that can significantly impact the quality of life for many women. The findings regarding the frequency and intensity of dysmenorrhea are also noteworthy. The majority of participants (76.3%) reported experiencing dysmenorrhea with every menstrual period, and a significant proportion (25.2%) rated their menstrual pain as severe (8–10 on a scale of 1–10). These findings are consistent with previous studies that have documented the debilitating nature of dysmenorrhea for many women.2,43 The analysis of management practices revealed that 61% of participants fell into the “low utilization” category for pharmacological interventions, having used one or fewer medication types for dysmenorrhea. In contrast, 51.6% of participants demonstrated “moderate utilization” of nonpharmacological approaches, typically employing two to three different pain management techniques such as heat therapy, rest, or herbal remedies. This suggests that women may be more inclined to explore nonpharmacological options, such as lifestyle modifications, complementary therapies, and pain management techniques, before resorting to pharmacological interventions, which is consistent with previous findings.44,45 Given the individual variability in the experience and management of dysmenorrhea, a personalized approach that considers each woman’s unique symptoms, preferences, and response to different interventions may be more effective in managing this condition. 2
Our study found no statistically significant association between age range and dysmenorrhea management practices, contrasting with Kamel et al. 46 and Wong and Khoo 47 but aligning with Banikarim et al., 48 suggesting management practices may be influenced more by factors such as pain severity or accessibility rather than age alone. Program of study showed no significant association with pharmacological management but was significantly associated with nonpharmacological management practices, partially supporting research by Armour et al. 12 and Titilayo et al., 15 which indicates educational content exposure may shape students’ approaches to pain management. Neither marital status, age at menarche, ethnicity, nor religious denomination showed significant associations with management practices, contrasting with some previous studies16,49 but suggesting these demographic factors may be less influential than previously thought in determining dysmenorrhea management practices among Ghanaian adolescents. These findings highlight the importance of providing comprehensive menstrual health education to all adolescents regardless of demographic characteristics, incorporating basic menstrual health education into school curricula across all programs, and focusing on evidence-based approaches while respecting cultural and religious sensitivities.
The results showed that adolescent girls who experience dysmenorrhea more frequently (every menstrual period) demonstrated a borderline association with higher levels of pharmacological management (p = 0.05), suggesting a trend that requires further investigation with larger sample sizes before definitive conclusions can be drawn. This finding is supported by previous studies, which show that women with frequent or more severe menstrual pain are more likely to use medications such as NSAIDs or oral contraceptives.25,26,30 Our study did not find a statistically significant association between the frequency of dysmenorrhea and the adoption of nonpharmacological management practices (p = 0.18). This suggests that the frequency with which adolescents experience menstrual pain may not be a determining factor in their choice to use nondrug interventions such as exercise, dietary adjustments, or other lifestyle modifications. These findings differ from expectations based on some previous literature, which had suggested potential relationships between pain frequency and management approach preferences. 50 The lack of association in our study population warrants further investigation, as it may reflect specific contextual factors related to our study setting or population characteristics. In contrast, those experiencing dysmenorrhea every 2–3 months did not show significant differences in either management practice. This suggests that the infrequent occurrence of dysmenorrhea in this group may not drive a strong need for consistent management strategies, a finding that has not been widely explored in previous research and warrants further investigation.
The intensity of dysmenorrhea was also a strong predictor of pharmacological management practices. Girls reporting moderate or severe pain were significantly more likely to engage in pharmacological practices, a finding in line with literature that suggests greater pain intensity leads to increased reliance on medications.42,51 Interestingly, intensity was not a significant predictor of nonpharmacological management practices, contradicting some studies that suggest severe menstrual pain often prompts individuals to seek alternative therapies alongside medications.52,53
Implications of the findings
These findings suggest that dysmenorrhea severity is a key factor influencing the choice of management strategies, particularly pharmacological ones. This has important implications for healthcare providers, as it underscores the need for targeted education on pain management tailored to the experiences of adolescent girls. For those with frequent and intense dysmenorrhea, access to appropriate pharmacological treatments should be emphasized, while for those with less-frequent symptoms, nonpharmacological options could be promoted. Furthermore, the lack of significant findings for nonpharmacological management practices based on dysmenorrhea intensity suggests a potential gap in knowledge or accessibility of alternative therapies. This highlights the need for better awareness and integration of nondrug approaches in menstrual health education programs. Schools and healthcare providers should offer educational sessions that address both pharmacological and nonpharmacological management practices, with a focus on providing resources and information for adolescent girls experiencing severe or frequent dysmenorrhea. Further research is needed to explore why nonpharmacological management practices are not significantly influenced by pain intensity and how best to promote these strategies in adolescent populations.
Limitations of the study
This study has number of limitations. The reliance on self-reported data may introduce recall or social desirability bias, as participants’ perceptions of dysmenorrhea and their management practices may not fully align with objective clinical assessments. The cross-sectional design limits the ability to establish causal relationships between dysmenorrhea and management practices, as data was collected at a single point in time. Additionally, the findings may lack generalizability, as the study was conducted in a specific geographic and cultural context Furthermore, while our study categorized management strategies into pharmacological and nonpharmacological approaches, future research might benefit from more granular sub-categorization within these broad groups, such as differentiating between evidence-based and nonevidence-based nonpharmacological approaches, or between over-the-counter and prescription medications.
Conclusion
This study revealed a high prevalence (82.4%) of dysmenorrhea among female adolescents in Ghana, with most experiencing it during every menstrual period. Pain intensity emerged as a significant predictor of pharmacological management, with those reporting moderate-to-severe pain more likely to use medications. Program of study significantly influenced nonpharmacological management practices, suggesting that educational exposure shapes pain management approaches. These results underscore the importance of a comprehensive, personalized approach that integrates both pharmacological and nonpharmacological interventions. Healthcare providers should tailor management plans based on individual experiences and promote awareness of nonpharmacological options, empowering women to actively manage their condition.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251409314 – Supplemental material for Pharmacological and nonpharmacological management of dysmenorrhea among senior high school girls in two districts in the Central Region of Ghana
Supplemental material, sj-docx-1-smo-10.1177_20503121251409314 for Pharmacological and nonpharmacological management of dysmenorrhea among senior high school girls in two districts in the Central Region of Ghana by Dorothy Serwaa Boakye, Vida Maame Kissiwaa Amoah, Beatrice Nyamekye Baidoo, Wisdom Kwaku Amuka Achiam and Emmanuel Kumah in SAGE Open Medicine
Footnotes
Acknowledgements
The author would like to express her sincere gratitude to the adolescent girls who participated in this study. Their openness and willingness to contribute to this research is greatly appreciated. The author also acknowledges the support and guidance provided by the school administration, and teachers who facilitated access to the study population and enabled the smooth conduct of this research.
Ethical considerations
All methods and research procedures were carried out per relevant ethical guidelines and regulations. Ethical approval was obtained from the Ghana Health Service Ethics Review Committee (GHS-ERC: 004/07/24).
Consent to participate
Written informed consent was obtained from all participants as follows: (1) for adult participants aged 18–24 years, written informed consent was obtained directly from the participants; (2) for minor participants aged 13–17 years, written informed consent was obtained from their legally authorized representatives (parents, legal guardians, or school authorities acting in loco parentis), and written assent was secured from the minor participants themselves. All consent and assent procedures were completed before enrollment in the study, and all participants were informed of their right to withdraw at any time without consequences.
Consent for publication
Not applicable.
Author contributions
D.S.B. conceptualized the study, designed the methodology, supervised data collection, drafted the initial manuscript. E.K. and V.M.K.A. contributed to the study design, assisted with data analysis, and critically reviewed the manuscript for important intellectual content. B.N.B. assisted with the literature review, and participated in data collection. W.K.A.A. provided technical guidance on statistical analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data set are available upon reasonable request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.