
Abstract
Title:
Traumatic brain injury outcomes and mortality predictors in Eastern India: A prospective observational cohort study
Objective:
To evaluate clinical outcomes and identify predictors of mortality in patients with traumatic brain injury treated at a tertiary trauma centre in Eastern India.
Methods:
This was a single-centre prospective observational cohort study conducted at AIIMS, Patna, Bihar, Eastern India, over 18 months (July 2023–January 2025). A total of 383 consecutive patients with traumatic brain injury were enrolled based on predefined inclusion and exclusion criteria. Demographic, clinical, radiological, and management variables were recorded. Functional outcomes were assessed at discharge, 3 months, 6 months months using the Glasgow Outcome Scale-Extended. Logistic regression was used to identify independent predictors of mortality and poor functional outcome.
Results:
The mean age was 34.4 ± 15.2 years, and most patients were male (68.9%). Road traffic accidents were the leading cause of injury (68.9%). Based on admission Glasgow Coma Scale, 53.3% had mild, 20.1% moderate, and 26.6% severe traumatic brain injury. Mortality was 23.5% at discharge and 24.5% at 6 months, with 95.7% of deaths occurring within the first month. Favourable outcomes (Glasgow Outcome Scale-Extended 6–8) were observed in 66.1% at 3 months and 70.8% at 6 months. Severe traumatic brain injury was significantly associated with 6-month mortality (p < 0.001) and poor outcomes (p < 0.001). Radiological features associated with mortality included intraventricular haemorrhage (p = 0.011), midline shift (p = 0.019), third ventricle obliteration (p = 0.023), sulcal effacement (p = 0.028), and cisternal collapse (p = 0.017). Multivariate analysis confirmed older age, lower Glasgow Coma Scale, abnormal pupillary reflex, intraventricular haemorrhage, and sulcal effacement as independent predictors of 6-month mortality. Among management strategies, burr-hole surgery yielded the best functional recovery (93.3%), while craniectomy was associated with the highest mortality (45.0%).
Conclusions:
Traumatic brain injury in Eastern India predominantly affects young males in road traffic accidents. While functional recovery appeared to improve between discharge and 6 months, severe injuries and specific radiological features may be associated with increased mortality. Burr-hole surgery and craniotomy may be linked to more favourable outcomes compared with craniectomy. Strengthening trauma systems and timely surgical interventions may help improve outcomes in resource-limited settings.
Keywords
Introduction
Traumatic brain injury (TBI), a form of acquired brain damage, is a significant global health concern and a leading cause of mortality, disability, and long-term socio-economic impact. 1 While TBI affects individuals across all age groups, young adult males are disproportionately affected, particularly in low- and middle-income countries (LMICs) such as India. 1 The burden is further amplified in regions experiencing rapid urbanisation, increased vehicular traffic, and industrial development, all of which contribute to a rising incidence of road traffic injuries and related trauma. 2
In India, the increasing frequency of road accidents, workplace injuries, and interpersonal violence has led to a steady rise in TBI cases. 2 Eastern states like Bihar face additional challenges due to limited trauma care infrastructure, delayed emergency response systems, and inadequate documentation of trauma epidemiology. 3 Despite the growing burden of TBI, there remains a lack of region-specific epidemiological data, and few studies have systematically evaluated the clinical outcomes or predictors of recovery and mortality in these populations. 3 The absence of trauma registries and standardised reporting systems further limits the ability to assess regional trends or optimise resource allocation. 3
Given these gaps, the present study was conducted at a level-1 trauma centre in Eastern India to evaluate the functional outcomes of TBI patients using Glasgow Outcome Scale-Extended (GOSE) and identifying clinical and radiological factors associated with mortality and recovery. This information is essential to inform clinical decision-making, improve trauma care protocols, and support health policy development in similar low-resource settings.
Materials and methods
This prospective observational study was conducted at a tertiary-level trauma centre in Eastern India after obtaining approval from the Institutional Research and Ethics Committee. The study enrolled patients diagnosed with TBI who were admitted to the trauma centre between July 2023 and January 2025. There were no age-related eligibility restrictions; patients of all ages presenting with TBI were considered for inclusion. TBI diagnosis was established using standardized clinical and radiological criteria, including a history of head trauma with any alteration of consciousness, loss of consciousness, post-traumatic amnesia, or neurological deficits, in conjunction with findings on non-contrast computed tomography (NCCT) head. The Glasgow Coma Scale (GCS) was used to grade severity but was not the sole diagnostic criterion. Patients whose predominant injuries involved anatomical regions other than the brain (as determined by the Abbreviated Injury Score), those with pre-existing bleeding or neurological disorders, and pregnant females were excluded.
Data collection included demographic variables (age, sex, time interval from injury to presentation, and mechanism of injury), clinical parameters (GCS score and pupillary reflex), radiological findings (NCCT of the head), and treatment modalities (operative and non-operative management, including external ventricular drainage, burr-hole surgery, craniotomy, and craniectomy). All patient data were de-identified at the time of entry to ensure anonymity and confidentiality. Follow-up assessments were performed at 3 and 6 months post-discharge through outpatient visits. For patients unable to attend follow-up in person, structured telephonic interviews with family members or Legally Authorized Representatives were conducted to ascertain survival status and functional outcome (including mortality). At least two repeat calls were attempted if initial contact was unsuccessful, to minimize missing follow-up data. The primary outcome was functional recovery, assessed using the GOSE at discharge, 3, and 6 months. The secondary outcome was in-hospital and post-discharge mortality.
The GCS 4 was used to assess the level of consciousness, with scores categorized as mild (13–15), moderate (9–12), and severe (⩽8), as shown in Table 1. The GOSE 5 was used to classify functional outcomes into poor (scores 3–5), good (6–8), and death (score 1), as presented in Table 2.
GCS.

Glasgow Outcome Scale-Extended.
Ethics
The study was conducted after obtaining approval from the Institutional Ethics Committee and the Institutional Research Board of All India Institute of Medical Sciences, Patna, with ethical approval number—AIIMS/Pat/IEC/PGTh/July22/18)/AIIMS/Pat/IEC/2022/123, dated 22 June 2023, All procedures performed involving human participants were in accordance with the ethical standards of the institutional committee and with the principles outlined in the Declaration of Helsinki (1975), as revised in 2024. Written informed consent was obtained from all participants or their legally authorized representatives prior to inclusion in the study. All patient records were anonymized, and no identifiable information (including names, initials or hospital numbers) was collected, stored or reported in this study. The study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 6
Statistical analysis
All data were collected prospectively and entered into a structured database with predefined mandatory fields to minimize missingness. The study included all consecutive patients with TBI who presented to the emergency department during the study period and met the inclusion criteria. Inclusion criteria were: (1) diagnosis of TBI confirmed by clinical assessment and neuroimaging; (2) presentation within 24 h of injury; and (3) availability of complete 6-month outcome data. Exclusion criteria were: (1) penetrating or missile head injuries; (2) patients with isolated facial, spinal, or peripheral injuries without intracranial involvement; (3) those with pre-existing severe neurological disorders (e.g. prior stroke, neurodegenerative disease) or significant psychiatric illness precluding outcome assessment; (4) patients transferred from another institution more than 24 h post-injury and (5) cases with incomplete or missing key clinical or radiological data despite verification. Missing data were identified at the point of entry and verified against source case records. The extent of missing data was minimal (<2% across all variables). For the analysis, missing data were handled using a complete-case approach, and no imputation techniques were applied. Quantitative variables were expressed as mean ± standard deviation for normally distributed data and as median with interquartile range for skewed distributions. Qualitative variables were presented as frequencies and percentages. The association between categorical variables and outcomes was analyzed using the chi-square (χ2) test. A p-value of less than 0.05 was considered statistically significant.
Univariate logistic regression analyses were performed separately for two primary outcomes: (1) mortality at 6 months post-injury and (2) functional outcome at 6 months, dichotomized as good (GOSE 6–8) versus poor (GOSE 3–5). A total of 21 variables were included in the univariate analysis, encompassing demographic factors (age, sex), clinical parameters (GCS, pupillary status), injury-related factors (mechanism of injury, time to presentation), radiological findings (extradural haemorrhage (EDH), subdural haemorrhage (SDH), brain contusion, subarachnoid haemorrhage (SAH), intraventricular haemorrhage (IVH), intraparenchymal bleed, midline shift, obliteration of third ventricle, sulcal effacement, cisternal collapse, skull/bony fracture), and management strategies (non-operative, burr-hole surgery, craniotomy, craniectomy). Variables with a p-value ⩽0.20 in univariate analysis were included in the multivariate logistic regression model to adjust for confounding factors, following recommended statistical guidelines. 7 Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) and p-values were reported for all independent predictors of mortality and poor functional outcome.
Although multiple univariate tests were performed, these analyses were exploratory in nature; therefore, no formal correction for multiple comparisons (e.g. Bonferroni or false discovery rate adjustment) was applied. Consequently, the univariate pvalues should be interpreted with caution and viewed as hypothesis-generating rather than confirmatory.
The subsequent multivariate logistic regression models were used to identify independent predictors while adjusting for potential confounding among included variables. The p values reported in these models reflect the adjusted association of each predictor with the outcome, but they do not represent correction for multiple testing. This two-step approach was intended to balance exploratory discovery with control for confounding in assessing predictors of mortality and functional outcome.
No formal a priori sample size calculation was performed, as this was an exploratory, observational study utilizing all eligible consecutive cases of TBI admitted during the study period. The sample size (n = 383) was therefore determined by the number of patients meeting the inclusion criteria within the study timeframe, which provided sufficient data to perform multivariate analyses with an adequate events-per-variable ratio for the outcomes of interest.
Model performance was assessed using overall accuracy, sensitivity, and specificity, which are reported in ‘Results’. The Hosmer–Lemeshow goodness-of-fit test was applied to check model calibration, and no significant lack of fit was observed (p > 0.05). Multicollinearity was assessed before including variables in the final model (no loss to follow-up occurred in this cohort (n = 0). For other study variables, missing data were minimal and handled by complete-case analysis; no imputation techniques were applied).
Additionally, sensitivity analyses were conducted excluding paediatric patients (⩽20 years) to assess the stability of predictors identified in the overall cohort. The detailed results of these analyses are provided in Table S1).
Bias mitigation
To reduce potential sources of selection and information bias, the study employed predefined inclusion and exclusion criteria, standardized data collection protocols, and validated outcome measures (the GCS (Teasdale and Jennett) and the GOSE (Wilson et al.)). Multivariate logistic regressions were used to adjust for potential confounding variables in the analysis. (However, this adjustment does not constitute correction for multiple testing, which was not applied given the exploratory nature of this prospective observational study.)
All analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 423 patients were assessed for eligibility for inclusion in the study. Of these, 40 patients were excluded: 28 patients met one or more exclusion criteria (e.g. penetrating head injury, delayed referral, or incomplete data), and 12 patients declined to participate (Figure 1). As a result, 383 patients were included in the final study prospective cohort. There was no loss to follow-up during the study period (n = 0), and all 383 patients were included in the final analysis. The included patients ranged in age from 1 to 80 years, reflecting the absence of age-related eligibility restrictions in this study. It is important to note that the findings are based on data from a single centre, which may limit external validity and generalizability, although the prospective design supports strong internal validity.

Flow diagram.
Demographic and clinical characteristics
The study included 383 patients with TBI. The mean age was 34.4 ± 15.2 years (range: 1–80 years). The majority were male (68.9%, n = 264/383). The largest age group was 21–40 years (38.4%, n = 147/383), followed by 1–20 years (29.8%, n = 114/383), and >40 years (31.8%, n = 122/383).
Road traffic accidents were the leading cause of injury (68.9%, n = 264/383), followed by falls (23.8%, n = 91/383) and other causes (7.3%, n = 28/383).
Based on GCS at admission, 53.3% (204/383) had mild, 20.1% (77/383) had moderate, and 26.6% (102/383) had severe TBI. Pupillary reflexes were normal in 74.7% (286/383) and abnormal in 25.3% (97/383). Detailed distributions of demographic and clinical variables are provided in Table 3.
Demographic and clinical presentations.

SD: standard deviation.
Radiological findings
On NCCT head, the most frequent abnormality was brain contusion (41.0%, 157/383), followed by skull fracture (32.1%, 123/383). Other findings included SDH (33.7%, 129/383), EDH (18.5%, 71/383), SAH (22.2%, 85/383), IVH (7.6%, 29/383), intraparenchymal haemorrhage (12.8%, 49/383), midline shift >5 mm (28.4%, 109/383), third ventricle obliteration (15.4%, 59/383), sulcal effacement (17.5%, 67/383), and cisternal collapse (12.3%, 47/383; Table 4).
CT findings and outcomes.

Note. Each row represents patients with the respective CT finding. Outcomes classified as: good, GOSE 5–8; poor, GOSE 2–4; death, GOSE 1 (at 6 months). p values represent the association of each CT finding with outcomes (good, poor, death).
Statistical significance (p < 0.05).
CT: computed tomography; EDH: extradural haematoma; GOSE: Glasgow Outcome Scale-Extended; IVH: intraventricular haemorrhage; SAH: subarachnoid haemorrhage; SDH: subdural haematoma.
Management
More than half of the patients were managed non-operatively (55.1%, 211/383). Among surgical interventions, decompressive craniectomy was most common (29.0%, 111/383), followed by craniotomy (21.1%, 81/383) and burr-hole surgery (14.1%, 54/383). A small subset underwent external ventricular drainage (EVD, 2.6%, 10/383). Treatment approaches are outlined in Table 5.
Management modalities.

Note. Table 5 shows the distribution of management types. Outcomes are classified according to GOSE at 6 months. The p values for outcome associations are reported in Table 4. Associated outcomes (across management types): good outcome: 272, poor outcome: 18, and deaths: 93.
GOSE: Glasgow Outcome Scale-Extended.
Outcomes
At discharge, the overall mortality rate was 23.5% (90/383), increasing slightly to 24.5% (94/383) at 6 months. By 3 months, 66.1% (253/383) of patients had achieved a favourable outcome (GOSE 6–8), which improved to 70.8% (271/383) by 6 months. Importantly, 95.7% (90/94) of deaths occurred within the first month of injury (Table 6). A sensitivity analysis excluding paediatric patients (⩽20 years) demonstrated similar patterns of associations in both univariate and multivariate logistic regression models for mortality and GOSE outcomes, confirming the robustness of our findings (see Table S1).
Outcomes at discharge, third, and sixth month (N = 383).

GOS: Glasgow Outcome Scale.
Association with outcomes
Chi-square analysis demonstrated that severe head injury was significantly associated with higher mortality at 6 months post-injury (47.5%, 47/99, χ2 p = 0.0004) and poor outcomes (χ2 p = 0.0012, Table 7). Among the radiological variables, IVH was associated with a mortality rate of 72.4% (21/29, p = 0.011). Patients with midline shift had a mortality rate of 52.3% (57/109, p = 0.019), while those with obliteration of the third ventricle had a mortality rate of 49.2% (29/59, p = 0.023). Sulcal effacement was strongly associated with mortality, occurring in 77.8% (52/67, p = 0.028) of deaths. Similarly, patients with cisternal collapse had a 42.4% (20/47, p = 0.017) mortality rate. Management type also correlated with outcomes. Burr-hole procedures showed the highest functional recovery at 6 months (GOSE 6–8: 93.3%, 50/54, p = 0.002), followed by craniotomy (GOSE 6–8: 82.2%, 67/81, p = 0.013). Non-operative management resulted in favourable outcomes in 74.1% (156/211, p = 0.041; Table 8).
Outcome details at 0, 3, and 6 months as compared with the severity of head injury according to the Glasgow Outcome Scale.

GCS: Glasgow Coma Scale.
Outcomes as compared with the management type.

Note. The p value represents the comparison of overall outcome distribution (good outcome, poor outcome, death) across the different management groups using GOSE.
GOSE: Glasgow Outcome Scale-Extended.
Predictors of mortality
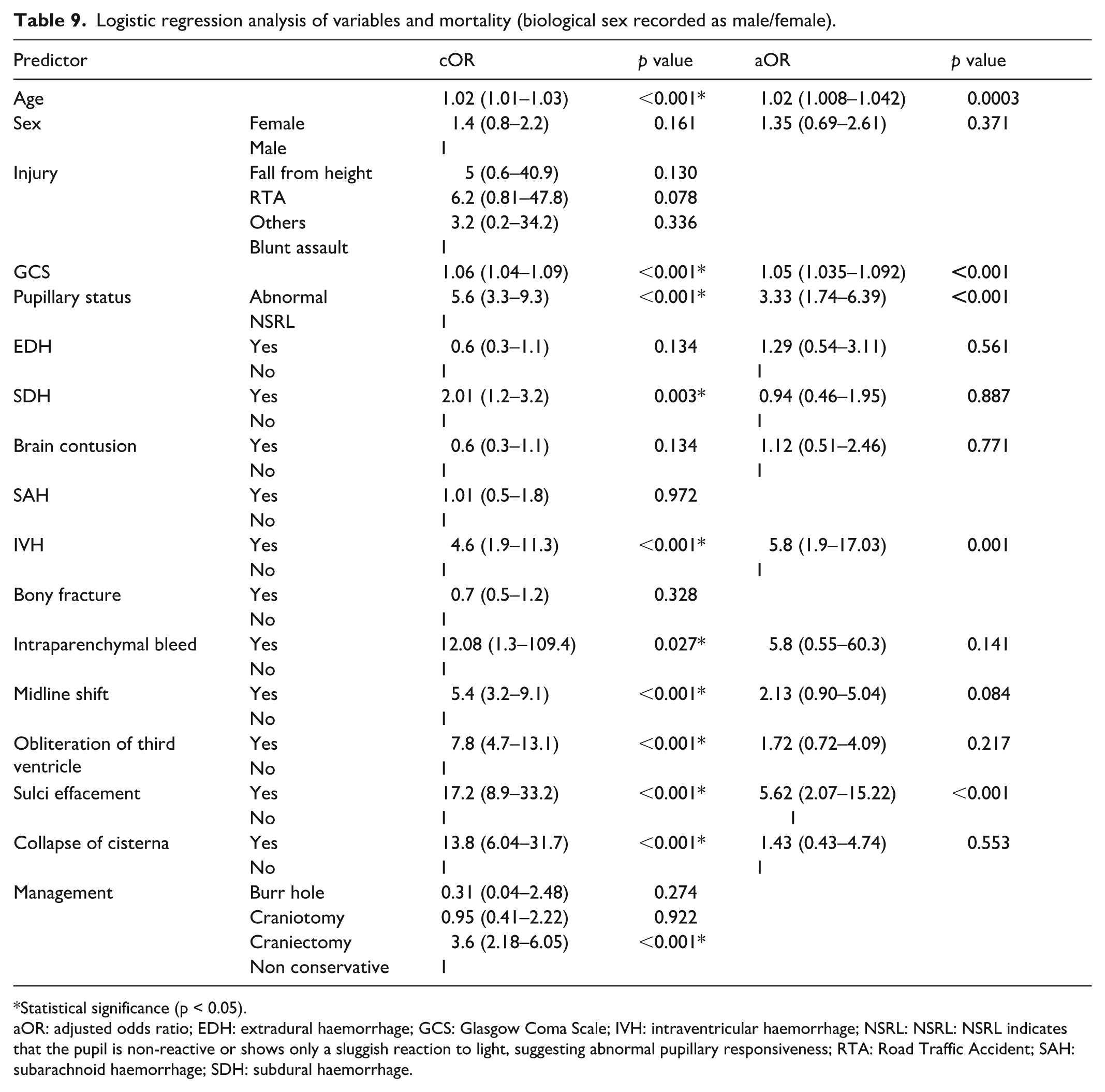
Univariate logistic regressions identified several predictors of mortality at 6 months post-injury. For transparency, the statistical information for all variables is presented in Table 9, and the narrative text focuses on those that remained statistically significant in the multivariate model. Covariates that did not meet the inclusion threshold of p < 0.20 in univariate analysis (e.g. SAH, bony fracture, management type: burr-hole/craniotomy, among others) were not entered into the multivariate model. Older age crude odds ratio ((cOR) 1.02 (95% CI: 1.01–1.03), p = 0.002), lower GCS scores (cOR 1.06 (95% CI: 1.04–1.09), p < 0.001), and abnormal pupillary status (cOR 5.6 (95% CI: 3.3–9.3), p < 0.001) were all significantly associated with higher mortality. On multivariate analysis, older age (aOR 1.02, p = 0.0003), lower GCS (aOR 1.05, p < 0.001), abnormal pupillary status (aOR 3.33, p < 0.001), IVH (aOR 5.8, p = 0.001), and sulcal effacement (aOR 5.62, p < 0.001) were identified as independent predictors of mortality at 6 months post-injury (Table 9). Sensitivity analyses excluding paediatric patients (⩽20 years) yielded comparable results, with no major change in the direction or significance of key predictors (Table S1).
Logistic regression analysis of variables and mortality (biological sex recorded as male/female).
Statistical significance (p < 0.05).
aOR: adjusted odds ratio; EDH: extradural haemorrhage; GCS: Glasgow Coma Scale; IVH: intraventricular haemorrhage; NSRL: NSRL: NSRL indicates that the pupil is non-reactive or shows only a sluggish reaction to light, suggesting abnormal pupillary responsiveness; RTA: Road Traffic Accident; SAH: subarachnoid haemorrhage; SDH: subdural haemorrhage.
On univariate analysis, several variables were significantly associated with poor functional outcome at 6 months (GOSE 3–5). These included increasing age (cOR 1.02, 95% CI: 1.01–1.03, p < 0.001), lower GCS at admission (cOR 1.06, 95% CI: 1.04–1.09, p < 0.001), abnormal pupillary status (cOR 5.6, 95% CI: 3.3–9.3, p < 0.001), presence of subdural haematoma (cOR 2.01, 95% CI: 1.2–3.2, p = 0.002), IVH (cOR 4.6, 95% CI: 1.9–11.3, p < 0.001), intraparenchymal bleed (cOR 12.08, 95% CI: 1.3–109.4, p = 0.029), midline shift (cOR 5.4, 95% CI: 3.2–9.1, p < 0.001), obliteration of the third ventricle (cOR 7.8, 95% CI: 4.7–13.1, p < 0.001), sulcal effacement (cOR 17.2, 95% CI: 8.9–33.2, p < 0.001), collapse of cisterns (cOR 13.8, 95% CI: 6.04–31.7, p < 0.001), and craniectomy as a management strategy (cOR 3.6, 95% CI: 2.18–6.05, p < 0.001).
When adjusted for potential confounders in the multivariate logistic regression model, independent predictors of poor functional outcome remained: increasing age (aOR 1.02, 95% CI: 1.007–1.041, p = 0.001), lower GCS at admission (aOR 1.05, 95% CI: 1.03–1.09, p < 0.001), abnormal pupillary status (aOR 3.28, 95% CI: 1.72–6.25, p < 0.001), IVH (aOR 5.5, 95% CI: 1.87–16.1, p < 0.001), and sulcal effacement (aOR 5.45, 95% CI: 2.01–14.8, p < 0.001). Other variables, although significant on univariate analysis, lost significance in the multivariate model. These findings are summarized in Table S1. Sensitivity analyses excluding patients aged ⩽20 years demonstrated consistent associations for these predictors of poor functional outcome, supporting the stability of the overall model (see Table S1).
The model demonstrated strong predictive accuracy (85.4%), with a specificity of 94.7% and a sensitivity of 58.2%. The goodness-of-fit was confirmed by the Hosmer–Lemeshow test (p = 0.61), indicating a robust identification of survivors but a moderate detection of non-survivors (Figure 2).

Predictive model accuracy: 85.4%, specificity: 94.7%, sensitivity: 58.2%.
A sensitivity analysis excluding paediatric patients (⩽20 years, n = 114) showed similar patterns of association, confirming the robustness of predictors (see Table S1).
Discussion
This prospective observational cohort study highlights the demographic and clinical characteristics, imaging findings, management strategies, and outcomes of TBI patients at a major trauma centre in eastern India. The prospective design is an important strength, as it allowed for systematic data collection and reduced recall bias, thereby providing a more accurate reflection of patient presentation, management, and outcomes in a high-burden, resource-limited setting.
A significant observation was the predominance of young adult males (68.9%, 264/383) involved in road traffic accidents (68.9%, 264/383), consistent with findings from other LMICs.1,8–14 This reflects the increased occupational and transportation-related exposure in this demographic and emphasizes the urgent need for targeted prevention strategies, including stronger road safety enforcement and public awareness initiatives.2,8
While previous studies from India and Africa have frequently reported falls as a major mechanism of injury,1,9,15 and road traffic accidents were the leading cause in our prospective cohort, likely due to high vehicular density2,8 and insufficient enforcement of traffic laws in the region.2,8,9 Furthermore, nearly one-third of patients (29.8%, 114/383) presented more than 24 h after injury, underscoring systemic barriers in emergency transport and referral pathways that contribute to delayed care and poorer outcomes.
These delays can often be explained by structural and socio-economic challenges that are common in LMICs. Limited availability of ambulances, long distances, and poorly maintained roads hinder timely hospital arrival, while financial constraints frequently delay decision-making and access to higher-level care.8,10 In addition, a lack of community awareness regarding the seriousness of head injuries contributes to delays in seeking treatment. 3 Addressing these barriers will require a multipronged approach, including investment in ambulance and referral networks, strengthening rural transport infrastructure, subsidizing emergency care costs for vulnerable populations, and community-level education to encourage early medical evaluation after trauma. This combination of factors may partly explain the late presentation observed in nearly one-third (n = 114) of our patients.
Our findings also reaffirm the prognostic value of early clinical indicators, with abnormal pupillary reflexes (25.3%, 97/383) and low GCS scores strongly associated with mortality (p = 0.0004) and poor outcomes (p = 0.0012) at 6 months.1,11,14 Radiologic features, particularly IVH (72.4% mortality, p = 0.011), sulcal effacement (77.8% mortality, p = 0.028), midline shift (52.3% mortality, p = 0.019), and cisternal collapse (42.4% mortality, p = 0.017), were linked to higher 6-month mortality and poorer functional recovery, consistent with prior reports.16–18 We additionally reported discharge and 3-month outcomes, which demonstrated a stepwise improvement in functional recovery over time, but the strongest prognostic associations remained evident at the 6-month follow-up.
Importantly, multivariate analysis demonstrated that older age (aOR 1.02, p = 0.003), lower GCS scores (aOR 1.05, p < 0.001), abnormal pupillary status (aOR 3.33, p = 0.001), IVH (aOR 5.8, p = 0.001), and sulcal effacement (aOR 5.62, p = 0.001) independently predicted mortality, supporting their use in prognostication and clinical decision-making in LMIC trauma settings.
Management was predominantly conservative (55.1%, 211/383), in line with practices in other resource-constrained centres.10,11 Surgical interventions were undertaken in cases of clinical deterioration or concerning imaging findings, with burr-hole procedures showing the highest functional recovery at 6 months (GOSE 6–8: 93.3%, 50/54, p = 0.002) and craniotomy also demonstrating favourable 6-month functional recovery (GOSE 6–8: 82.2%, 67/81, p = 0.013). These outcomes refer specifically to functional recovery rather than mortality. These results highlight the importance of careful patient selection for surgery and reinforce the role of conservative management in appropriately triaged patients.
The 6-month mortality rate (24.5%, 94/383) was comparable to reports from similar LMICs, though higher than figures from high-income countries.9,19–22 This discrepancy reflects multifactorial challenges, including delayed presentation, limited neurosurgical capacity, and restricted access to intensive care. Overall, the study underscores the urgent need to strengthen trauma systems in India—particularly prehospital care, timely imaging, and neurosurgical infrastructure—to improve outcomes for TBI patients.
Implications and limitations
The implications of this study are multifaceted. Firstly, the data provide a snapshot of TBI burden and outcomes in a high-volume Indian trauma centre, helping inform local clinical protocols and resource allocation. Secondly, it emphasizes the predictive value of clinical and imaging parameters that can be used even in settings with limited access to advanced neuromonitoring.
However, this study has several limitations. As a single-centre prospective observational cohort study, it may not capture regional variability or subtler clinical nuances. The lack of detailed follow-up data beyond 6 months and reliance on hospital records may have introduced some information bias. Functional outcomes were not stratified by specific neurocognitive or quality-of-life measures, which limits the granularity of recovery assessment. In addition, no formal sample size calculation was performed prior to study initiation; the analyses were based on all consecutive eligible patients, and as such, the study may have been underpowered to detect smaller effect sizes. Given the exploratory nature of the analyses, no formal correction for multiple comparisons was applied. As such, the results of univariate analyses should be interpreted with caution and considered hypothesis-generating rather than confirmatory. Finally, although multivariate logistic regression was used to adjust for potential confounding, residual confounding from unmeasured variables cannot be entirely excluded.
Future directions
Future research should focus on multi-centre prospective studies that incorporate long-term functional and cognitive outcomes. There is also a need to evaluate the impact of early rehabilitation, and prehospital interventions on TBI prognosis in LMICs. Additionally, development of context-specific prognostic models could enhance triage accuracy and inform decisions in overstretched emergency settings.
Conclusion
In this single-centre prospective observational cohort study, we provided a detailed assessment of TBI patterns and outcomes in a resource-limited setting. The findings suggest that young adult males are predominantly affected, with road traffic accidents being the leading mechanism of injury. Clinical severity at presentation and specific radiological findings such as IVH, sulcal effacement, midline shift, and cisternal collapse, and third ventricle obliteration may be important factors associated with mortality. Mortality remained high (23.5% at discharge, 24.5% at 6 months, with most deaths occurring in the first month). While conservative management was frequently employed, burr-hole surgery and craniotomy may be associated with more favourable functional recovery, whereas craniectomy appeared to carry the highest mortality. The observed improvement in GOS scores over 6 months may highlight the value of timely diagnosis, ongoing clinical monitoring, and structured follow-up. These results may indicate the need for strengthening trauma care systems, with particular attention to early intervention and standardized management protocols, which may enhance outcomes in similar healthcare environments.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251399149 – Supplemental material for Traumatic brain injury outcomes and mortality predictors in Eastern India: An observational study
Supplemental material, sj-docx-1-smo-10.1177_20503121251399149 for Traumatic brain injury outcomes and mortality predictors in Eastern India: An observational study by Harendra Kumar, Anil Kumar, Rachith Sridhar, Abdul Hakeem, Deepak Kumar, Abdul Vakil Khan, Anurag Kumar, Majid Anwer, Rekha Kumari and Sanjay Kumar in SAGE Open Medicine
Footnotes
Acknowledgements
The authors express their sincere appreciation to Dr. Abhishek Kumar, Dr. Shashikant, Dr. Jeeshan, Dr. Mayank, Dr. Anupam, Dr. Shaman, Dr. Karthik, Dr. Ankit, Dr. Shivangi, Dr. Aadil, Dr. Sayani, and Dr. Bhavya for their invaluable assistance in data collection and their dedicated support throughout the study.
ORCID iDs
Ethical considerations
The study was approved by the Institutional Ethics Committee and the Institutional Research Board of AIIMS Patna (ref no. AIIMS/Pat/IEC/PGTh/July22/18), dated June 22, 2023.
Consent to participate
Written informed consent was obtained from all participants or their legally authorized representatives prior to inclusion in the study.
Author contributions
Harendra Kumar contributed to conceptualization, study design, data curation, analysis, and drafting of the article. Anil Kumar assisted with methodology, data acquisition, and critical review. Rachith Sridhar supported data collection, validation, and article review. Abdul Hakeem performed statistical analysis and data interpretation. Deepak Kumar contributed to patient recruitment and investigation. Abdul Vakil Khan provided clinical supervision and article review. Anurag Kumar assisted with data curation, tables, and figures. Majid Anwer contributed critical revision, clinical insights, and supervision. Rekha Kumari conducted the literature review and proofreading. Sanjay Kumar provided project administration, overall supervision, and final approval of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.