
Abstract
Introduction:
Preeclampsia develops due to placental insufficiency and systemic proinflammatory and antiangiogenic mediator release, with ensuing systemic endothelial dysfunction. Nephrotic-range proteinuria appears to be associated with worse pregnancy outcomes. The relationship between differing degrees of proteinuria and the severity of placental alterations has not been studied.
Methods:
This is a single-centre retrospective comparison of 150 singleton pregnancies complicated by preeclampsia and varying degrees of proteinuria. Maternal demographic, obstetrical and fetal outcome data were obtained from chart review. The placental histologic evaluations were performed by a placental pathologist blinded to all other clinical information.
Results:
Preeclamptic women with massive proteinuria had evidence of more severe maternal vascular malperfusion lesions. The severity of the lesions was progressive through mild, moderate and massive proteinuria. Women with massive proteinuria had a higher incidence of renal dysfunction and severe hypertension, and had earlier preterm deliveries compared to preeclamptic women with mild and moderate proteinuria (p < 0.05).
Conclusion:
Preeclampsia with more severe proteinuria is associated with a higher prevalence of placental maternal vascular malperfusion.
Introduction
Preeclampsia, which affects 2%–8% of pregnancies, is a multisystemic disease that classically presents with new-onset hypertension and proteinuria after 20 weeks of gestation, but may affect many other organs including the fetoplacental unit.1,2 It is a leading cause of maternal and perinatal mortality and morbidity and has many long-term repercussions for both the mother and fetus . 1 The placenta is critical for the development of preeclampsia as exemplified by the higher risk of preeclampsia in molar pregnancies and fetal delivery as the only known cure.
Proteinuria is frequently observed in women with preeclampsia, while the incidence of acute kidney injury (AKI) in developed countries ranges from 0.76% to 16% with preeclampsia and from 7.7% to 60% with HELLP (haemolysis, elevated liver enzymes, and low platelets) syndrome.3–6
In preeclampsia, endotheliosis is commonly observed on kidney biopsy along with mesangial interposition, endocapillary foam cells and prominent podocytes with protein resorption droplets seen in severe cases of preeclampsia. 7 The podocytopathy is the result of antagonizing effects of circulating sFlt-1 on vascular endothelial growth factor (VEGF). Preventing VEGF from interacting with its transmembrane receptor on podocytes and endothelial cells leads to podocyte injury, loss of slit diaphragm integrity and ultimately podocyte detachment. 8 This podocytopathy may cause the nephrotic syndrome that sometimes accompanies preeclampsia.
Nephrotic range proteinuria appears to be associated with worse maternal, obstetric and fetal outcomes.9–11 Smaller amounts of proteinuria, 300–499 mg/24 h and over 499 mg/24 h of proteinuria, have been reported to cause a progressively higher incidence of adverse maternal and perinatal outcomes compared to controls. 12
Placental abnormalities are observed in preeclampsia. Their severity appears to follow maternal disease severity. 13 The abnormalities include smaller and fewer spiral arteries, placental infarctions, sclerotic villi, decidual arteriopathy, intervillous thromboses and an abnormal abundance of syncytial knots.14–16 An association has been observed between placental abnormalities and angiogenic imbalance.17–19 To date, few have studied the association between placental abnormalities and maternal, obstetric and fetal outcomes.
The aim of our study is to evaluate the relationships between severity of proteinuria, placental vascular abnormalities and maternal and fetal outcomes in preeclampsia. We hypothesized that more severe proteinuria would be associated with more severe placental alterations and that these would correlate with clinical outcomes.
Methods
We conducted a single centre retrospective pilot study, that looked at preeclamptic women having given birth in a tertiary hospital in Montreal, Quebec, Canada between 1 January 2017 and 30 June 2020. This study was approved by the hospital’s ethics committee (study number: 2021-2943).
Women with singleton pregnancies presenting with antepartum preeclampsia were included in this study. Preeclampsia was defined according to Canadian guidelines on hypertensive disorders of pregnancy, as a hospital systolic blood pressure (BP) ⩾140 mmHg and/or diastolic BP ⩾ 90 mmHg based on the average of two BP measurements within 15 min, and new onset of one of the following: proteinuria (protein/creatinine ratio (PCR) ⩾ 0.03 g/mmol) cardiorespiratory, haematological, renal, hepatic or fetoplacental injury/insufficiency. 20 We excluded women with multiple intra-uterine pregnancies, women with a history of thrombophilia, antiphospholipid antibody syndrome or kidney transplant, and women with pre-pregnancy or first trimester proteinuria (PCR ⩾ 0.03 g/mmol or albumin/creatinine ratio ⩾ 2 mg/mmol). The women were required to have a normal pre-pregnancy or first trimester baseline urinalysis.
Three groups of women were identified: preeclamptic women with mild proteinuria (PCR between 0.03 and 0.05 g/mmol inclusively), moderate proteinuria (PCR between 0.051 and 0.15 g/mmol inclusively) and massive proteinuria (PCR greater or equal to 0.5 g/mmol). The threshold used to distinguish mild from moderate proteinuria was based on a nested case-control study that observed more adverse outcomes among women with proteinuria over 499 mg/24 h versus 300–499 mg/24 h. 12 The PCR threshold for massive proteinuria was chosen based on previous studies observing more adverse outcomes among the women with a PCR ⩾ 0.5 g/mmol.9–11,21 The assignment of group was based on the maximum recorded level of gestational proteinuria. Preeclamptic women with massive proteinuria were matched to women with mild proteinuria based on their delivery date. The limited prevalence of preeclamptic women with moderate proteinuria rendered it impossible to similarly match them according to delivery date.
The following information was extracted from the medical chart: maternal demographic and past medical history including age at conception, obesity (pre-pregnancy body mass index ⩾ 30.0 kg/m2), hypertension, diabetes, chronic kidney disease (CKD) and previous preeclampsia; obstetric information including presence of gestational diabetes, early-onset preeclampsia (EOPE, defined as preeclampsia diagnosed prior to 34 weeks), severe hypertension (systolic BP ⩾ 160 mmHg or diastolic BP ⩾ to 110 mmHg), renal dysfunction (defined as a serum creatinine ⩾ 80 µmol/L), HELLP syndrome, pulmonary oedema, eclampsia, placental abruption, obstetric intensive care unit admission, use of magnesium sulphate, gestational age at diagnosis of preeclampsia onset and at delivery, and delivery mode; fetal complications including evidence of fetal growth restriction (FGR) on ultrasound, abnormal fetoplacental artery doppler waveform, small for gestational age (SGA) and perinatal mortality (death within the first 28 days of life). 22 Finally, highest antenatal serum alanine aminotransferase (ALT), uric acid, lactate dehydrogenase (LDH) and creatinine, and antenatal platelet count nadir were recorded.
Placenta shape and weight were determined by the pathology department at the time of delivery. Placental weight percentile was obtained using gestational age-specific placental weight charts. 23 Three representative full thickness sections of villous tissue avoiding placental margins but including both fetal and maternal surfaces and two cord fragments and membranes were submitted for histological analysis. When lesions were observed on the macroscopic examination, additional blocks of tissue from these areas were submitted for further analysis. The tissue sections were fixed in 10% neutral buffered formalin, paraffin-embedded and 3-μm-thick sections were subsequently stained with haematoxylin, eosin and saffron. For the purposes of this study, microscopic placental abnormalities were classified according to the Amsterdam Placental Workshop Group Consensus Statement.24–26 by a pathologist specialized in placental examination. A minimum of one placental lesion was required for the diagnosis of MVM. Other than for placental weight and gestational age for adequate maturity evaluation, the pathologist performing the analysis was blinded to all other maternal and fetal information.
Statistical analysis
As this was a pilot study, power analysis for sample size was not calculated. A sample of convenience of 50 women with preeclampsia per proteinuria threshold was chosen.
Data are presented as percentages for dichotomous variables, as mean ± standard deviation for normally distributed continuous variables or as median with its interquartile range for non-parametric continuous variables. Comparison of categorical variables were analysed using a Chi-square test. Student’s t-test and ANOVA test were used for normally distributed continuous variables while the Kruskal–Wallis test was used for non-parametric continuous variables. For multiple comparisons, the Bonferroni correction for multiple tests was used to determine the adjusted p-value. All analyses were done using SPSS software (version 26, IBM Corp., Armonk, NY). Binary logistic regression models were used to evaluate the association between placental alterations and proteinuria, while adjusting for pre-pregnancy obesity and gestational age at delivery below 34 weeks. A p-value < 0.05 was considered statistically significant.
Results
Maternal characteristics of the 150 women included in the study are presented in Table 1. Demographic data between women in the three groups were not statistically different (Table 1).
Patient characteristics.

ASA: acetylsalicylic acid; BMI: body mass index; BP: blood pressure; CKD: chronic kidney disease; IQR: interquartile range; LMWH: low-molecular weight heparin; NS: not significant; SGA: small for gestational age.
Median and interquartile range.
Obstetric and fetal outcomes are presented in Tables 2 and 3, respectively. Eclampsia was not observed among any of the women. The incidences of HELLP (p = 0.036) and placental abruption (p = 0.014) were statistically different between the groups. Massive proteinuria was associated with an earlier diagnosis of PE, a significantly greater rate of renal dysfunction, severe hypertension, and more frequent admission to the obstetric intensive care unit to receive magnesium sulphate (all adjusted p < 0.05). Moreover, preeclamptic women with massive proteinuria delivered earlier and more frequently required caesarean section than women with either mild or moderate proteinuria (both adjusted p < 0.05, Table 2). Higher maximum creatinine, uric acid, LDH and ALT levels were observed among women with preeclampsia and massive proteinuria compared to preeclamptic women with either mild or moderate proteinuria (all adjusted p < 0.05, Table 2).
Obstetric outcomes by level of proteinuria.

AKI: acute kidney injury defined as serum creatinine ⩾ 80 µmol/L; ALT: alanine aminotransferase; C/S: caesarean section; EOPE: early-onset preeclampsia; FGR: fetal growth restriction; HELLP: haemolysis elevated liver enzymes and low platelets; IQR: interquartile range; LDH: lactate dehydrogenase; NS: not significant; ICU: intensive care unit; VD: vaginal delivery.
Median and interquartile range.
Adjusted p < 0.05, statistically different than preeclampsia with massive proteinuria.
Fetal outcomes by level of proteinuria.
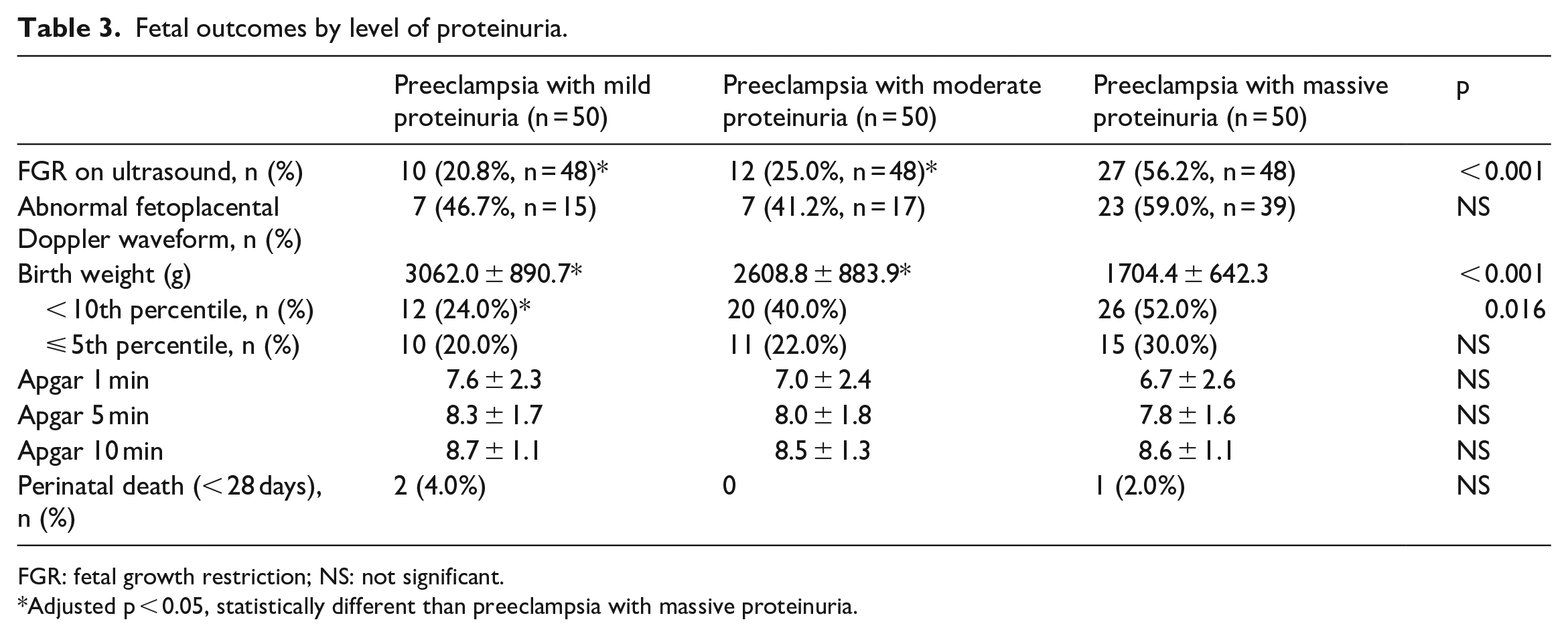
FGR: fetal growth restriction; NS: not significant.
Adjusted p < 0.05, statistically different than preeclampsia with massive proteinuria.
Fetal growth restriction on third trimester ultrasound was more frequently observed among preeclamptic women with massive proteinuria, while detection of abnormal doppler finding during third trimester imaging did not differ between groups. Concomitantly, there was a difference in the incidence of SGA below the 10th percentile between groups (p = 0.016, Table 3), with significantly more SGA among preeclamptic women with massive compared to mild proteinuria. No difference in perinatal mortality was observed.
On placental evaluation, 70% of women with massive proteinuria had signs of maternal vascular malperfusion (MVM) while these were observed in 22% and 36% of those with mild and moderate proteinuria, respectively (p < 0.001, Table 4). A positive association between the severity of proteinuria and MVM persisted even when MVM diagnosis required a minimum of two placental features (p = 0.040; data not shown). The association between MVM and proteinuria persisted after adjusting for gestational age below 34 weeks at delivery and pre-pregnancy obesity (OR = 2.30, 95% CI = 1.37–3.85; p = 0.002). Infarction and accelerated villous maturity were observed more frequently among women with massive proteinuria compared to those with mild or moderate proteinuria (both adjusted p < 0.05). Decidual arteriopathy was another frequent finding, although it was not associated with the level of proteinuria threshold. No difference in signs of fetal vascular malperfusion, maternal and fetal inflammatory responses were observed.
Comparison of placental findings by level of proteinuria.
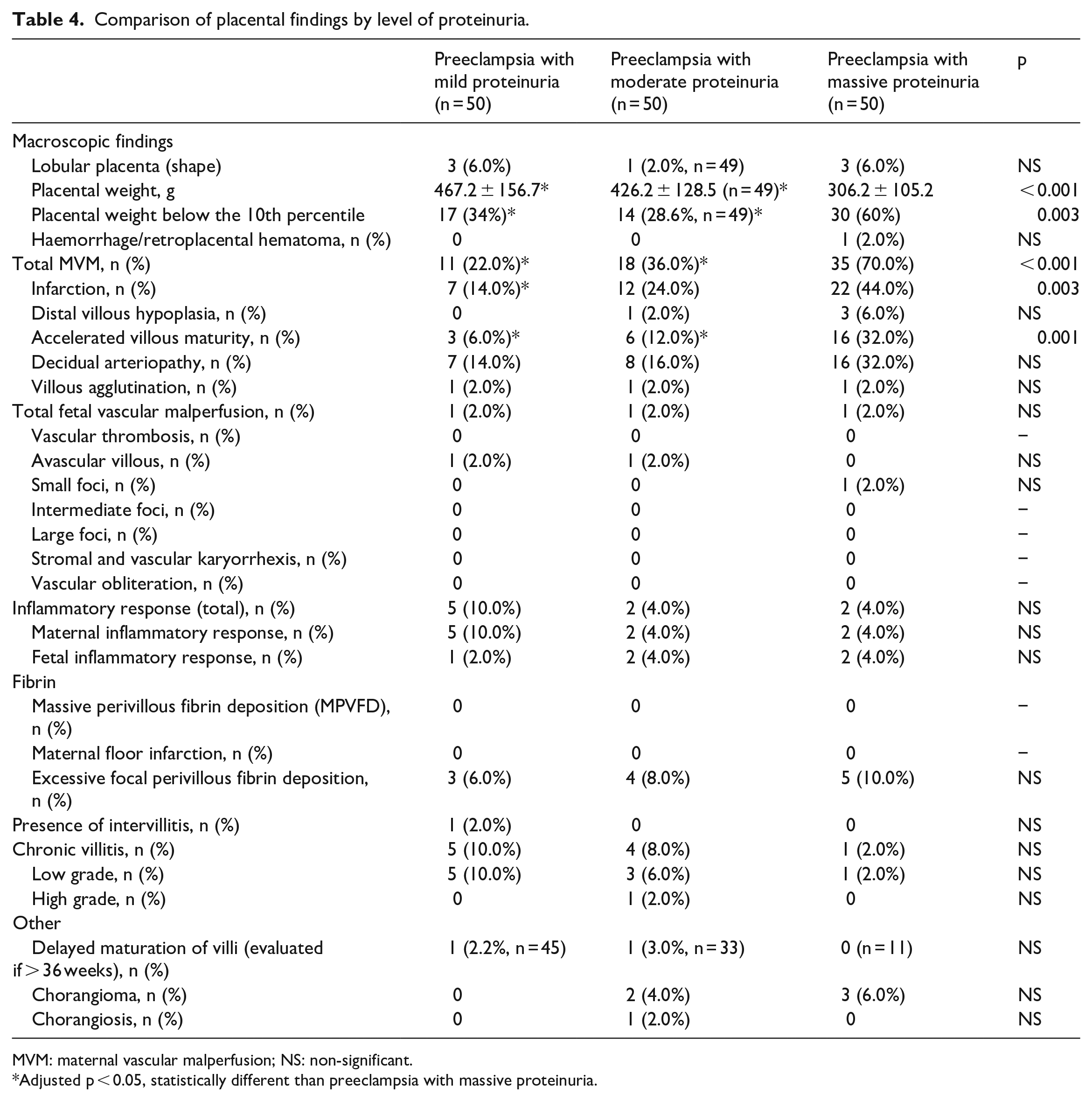
MVM: maternal vascular malperfusion; NS: non-significant.
Adjusted p < 0.05, statistically different than preeclampsia with massive proteinuria.
Uric acid levels were significantly higher in women with MVM compared to those without (399 ± 76 vs 337 ± 81 µmol/L, p < 0.001; Figure 1(a)). Upon stratifying women according to proteinuria, there was a progressive rise in uric acid as proteinuria worsened in those with and those without MVM (both p < 0.005, Figure 1(b)). No difference was observed in uric acid between preeclamptic women with or without signs of MVM for each proteinuria threshold.

Maximum uric acid prior to delivery in women without (white) or with (black) MVM. (a). According to MVM irrespective of proteinuria severity; (b). According to MVM and proteinuria thresholds. Student’s t-test was used to compare serum uric acid in the presence or absence of MVM while the ANOVA test was used when comparing uric acid levels in the presence or absence of MVM according to proteinuria threshold. Uric acid levels increased with progressive proteinuria among preeclamptic women without or with MVM (both p-trend < 0.005).
Discussion
This study investigated the association between proteinuria and placental pathology, and obstetric and fetal outcomes among women with preeclampsia. We found that preeclamptic women with more severe proteinuria received their diagnosis of preeclampsia earlier, delivered earlier, and had more severe hypertension, renal dysfunction, HELLP and placental abruption. The incidence of SGA and placental weights below the 10th percentile increased as gestational proteinuria worsened. Other maternal and fetal outcomes did not differ between groups, although the study was likely underpowered. On placental examination, women with preeclampsia and massive proteinuria had significantly more signs of MVM than women with mild or moderate proteinuria, even after adjusting for gestational age below 34 weeks at birth and pre-gestational obesity. There was a positive association between proteinuria severity and the incidence of infarcts and accelerated villous maturity.
MVM are evidence of placental insufficiency, and are observed in hypertensive disorders of pregnancy, spontaneous preterm birth (SPTB), preterm premature rupture of membranes (PPROM) and fetal growth restriction.27–29 Chisholm and colleagues compared placental findings among different causes of preterm birth using the Amsterdam Placental Workshop Group Consensus Statement and found that preeclampsia placentas had more infarcts, distal villous hypoplasia, accelerated villous maturation and decidual arteriopathy compared to those observed in other causes of preterm delivery. 30 They did not observe any evidence of maternal and fetal placental inflammatory responses among women with preeclampsia. These results are consistent with our findings and suggest that the MVM observed in our women are a result of their preeclampsia. Moreover, none of the women included in our study suffered from PPROM or SPTB.
In this study, women were stratified solely according to maximal gestational proteinuria. In doing so, we inadvertently created groups with different underlying preeclampsia phenotypes. Indeed, two phenotypically distinct antenatal preeclampsia entities are frequently described in the literature. EOPE presents prior to 34 weeks and results from defective spiral artery remodelling, uteroplacental malperfusion and subsequent systemic inflammation, endothelial dysfunction and microangiopathy. 31 Conversely, late-onset preeclampsia (LOPE) presents after 37 weeks, and is hypothesized to arise due to a mismatch between maternal supply and placental demands, combined with a maternal genetic predisposition to metabolic and cardiovascular diseases. 32 Distinguishing these entities has important prognostic value, as women who develop EOPE have a higher risk of pregnancy-related maternal and fetal adverse events, and future cardiovascular disease, compared to those with LOPE.33–35 Studies report histological differences between EOPE and LOPE placentas. MVM are more frequent in EOPE, supporting the earlier development of uteroplacental underperfusion. 36 Among the types of MVM, placental infarcts, villous hypermaturation, distal villous hypoplasia and decidual vasculopathy are those most frequently reported in EOPE.36–39 In LOPE, MVM are still observed, yet appear to be less frequent than in EOPE. This is compatible with the belief that LOPE arises from delayed onset malperfusion. The incidence of MVM in our preeclamptic women with mild and moderate proteinuria, who more frequently delivered after 37 weeks, are consistent with others who observed MVM in 25-30% of term PE.37,40 Abnormal uterine artery doppler waveform and angiogenic imbalance (increased sFlt-1/PlGF ratio) are also positively associated with MVM and are predictive of EOPE.17,41,42
Maternal inflammation is strongly associated with adverse pregnancy outcomes in preeclampsia with enhanced activation of the NF-κB signalling pathway and circulating damaged-associated molecular patterns (DAMPs).43–45 Uric acid, a DAMP possibly secreted by the placenta, was proposed to be involved in the pathogenesis of hypertensive disorders of pregnancy.46–49 In this study, we observed higher levels of uric acid among women with signs of MVM, and greater levels of uric acid as proteinuria worsened. This is consistent with in vitro and in vivo studies demonstrating placental inflammatory responses following higher uric acid exposure and those observing an association between serum uric acid and adverse pregnancy outcomes.50–53 Surprisingly, although uric acid has been implicated as an inflammatory mediator, inflammation on placental histology is not necessarily observed. 54 Inflammation, along with antiangiogenic mediators, are likely the link between preeclampsia and placental pathology, while proteinuria is but a marker of more severe disease.
The methodology chosen warrants further comment. This is single-centre study. All cases are recent, between 2017 and 2020, and received comparable preeclampsia management. We chose to compare preeclamptic women with varying degrees of proteinuria to specifically evaluate the association between proteinuria and outcomes. Drastically different thresholds of proteinuria were purposefully chosen to explore this association. Comparing these women to those with uncomplicated pregnancies would have introduced additional confounding.
When evaluating the association between MVM and proteinuria, we adjusted for gestational age below 34 weeks at delivery, and pre-gestational obesity as there is evidence of an association between obesity and placental abnormalities. 55 The impact of other maternal comorbidities on MVM has not been established. 56
The association between severe proteinuria and unfavourable obstetric and fetal outcomes has been previously described.9–11 Our findings corroborate previous studies that observe more AKI, HELLP syndrome, placental abruption, FGR, and prematurity with worsening proteinuria.9,11
To our knowledge, this is the first study to evaluate the association between severity of proteinuria and placental alterations. To limit the potential for subjective placental evaluation, placental analyses were performed according to the Amsterdam Consensus framework by a single placental expert pathologist within a short time frame. The pathologist was blinded to maternal and fetal information, with the exception of placental weight and gestational age for adequate evaluation of maturity. Our findings are based on MVM diagnosis requiring at least one anomaly among infarction, distal villous hypoplasia, accelerated villous maturity, decidual arteriopathy and villous agglutination. However, we persistently observed a positive association between MVM and severity of proteinuria even if MVM diagnosis required two or more placental features.
Limitations in the study design must be highlighted. This is a retrospective pilot study in which power analysis for sample size calculation was not performed; we ultimately decided on a sample size of 150 preeclamptic women grouping these into 3 groups characterized by mild, moderate and massive proteinuria. We were not able to include a group of women with moderate to severe proteinuria (PCR between 0.15 and 0.5 g/mmol) due to under representation. The small sample size hindered the ability to observe an association between the severity of proteinuria and several of the pregnancy outcomes, or to identify an independent association between MVM and uric acid levels among women with different proteinuria thresholds. There was no comparative control group of uncomplicated pregnancies. MVM can be observed in 25%–36% of placentas from uncomplicated pregnancies.57,58 These findings are comparable to what we observed in our cohorts with mild and moderate proteinuria. Again, due to the retrospective nature of the data, we were limited to studying the placental sections and histological analyses done at the time. Levels of pathogenic inflammatory and antiangiogenic markers were not available, as these were not currently supported by our provincial healthcare system.
Conclusion
In summary, this study shows that increased proteinuria in women with preeclampsia is associated with more prevalent MVM findings, even after adjusting for gestational age below 34 weeks at delivery and pre-pregnancy obesity. It is also associated with a higher incidence of HELLP, renal dysfunction, severe hypertension and placental abruption. Future studies are required to further evaluate the association between MVM and different degrees of proteinuria.
Footnotes
Author contributions
D.S.G. and E.R. researched the literature and conceived the study. E.R. was involved in gaining ethical approval. All authors were involved in protocol development and data analysis. D.D.S. performed placental analyses. D.S.G. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript prior to submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This study was approved by the Centre Hospitalier Universitaire Sainte-Justine institutional review board (study number: 2021-2943).
Informed consent
Informed consent was not required due to the retrospective nature of the study. The need for consent was waived by the Institutional Review Board.
Guarantor
E.R. is the guarantor of the present work.
Trial registration
Trial registration was not required due to the retrospective nature of the study.