
Abstract
Background:
Clinical empathy is a crucial skill for healthcare professionals, enhancing patient outcomes, and satisfaction. However, existing scales, such as the Jefferson Scale of Empathy, focus primarily on cognitive empathy, overlooking the affective component. This gap highlights the need for a validated tool that measures both cognitive and affective empathy in healthcare professionals. This study developed and validated a multidimensional scale—the Multidimensional Clinical Empathy Scale—for assessing both cognitive and affective empathy in healthcare professionals and students.
Methods:
This three-phase study involved item generation, reduction, and validation, using literature reviews, qualitative studies, and survey methodologies. Exploratory factor analysis and confirmatory factor analysis were applied to test the scale’s validity. The Multidimensional Clinical Empathy Scale was constructed using a five-domain theoretical model: Empathetic Connections, Valuing Empathy, Empathetic Behaviours, Genuine Concern, and Perspective Taking. After content validation and exploratory factor analysis, the scale was reduced to 26 items with high internal consistency (Cronbach alpha of 0.94).
Results:
There were a total of 977 participants, comprising doctors, medical students, nurses, and nursing students from acute hospitals, community hospitals, medical schools, and nursing schools. The final 26-item Multidimensional Clinical Empathy Scale demonstrated strong psychometric properties, with factor loadings confirming the multidimensionality of clinical empathy. Confirmatory factor analysis confirmed the scale’s four-factor structure, and the scale was validated across diverse healthcare settings with robust reliability and Content Validity Index (0.90).
Conclusions:
The Multidimensional Clinical Empathy Scale provides a comprehensive, validated tool for measuring both cognitive and affective empathy in healthcare professionals and students. Its multidimensional structure offers potential for broader applications in clinical education and research.
Keywords
Introduction
Clinical empathy (CE) is a vital and multifaceted quality 1 required for healthcare professionals. It improves patient compliance, outcomes,2–4 and contributes to patient 5 and healthcare professional satisfaction 6 and wellbeing. 7 Current-ly, the Jefferson Scale of Empathy (JSE) 8 is the predominant tool for assessing CE in healthcare professionals and students. 9 Although a meta-analysis reported moderate reliability (around 0.80) 10 for the JSE, it primarily measures cognitive empathy, missing the full spectrum of empathy, including affective empathy. 11 Conversely, the International Reactivity Index (IRI) measures both cognitive and affective empathy, but caters primarily to the general population. 12 Therefore, there is a need for a multidimensional tool tailored for healthcare professionals and students to measure the full spectrum of CE.
Measuring CE is essential not only to recognise its presence but to support its intentional development in clinical education and practice. By transforming empathy into a measurable construct, these tools enable the evaluation of training programmes, 13 inform individualised feedback 14 and ensure that empathy remains a core clinical competency rather than an abstract ideal. Objective measurement also allows empathy to be incorporated into broader quality improvement efforts in healthcare.
Our study builds on a previous qualitative study and defines CE as ‘a sense of connection between the healthcare worker and the patient as a result of perspective taking arising from imaginative, affective and cognitive processes, which are expressed through behaviours and good communication skills that convey genuine concern’. 15 Unlike previous definitions of CE which were promulgated by experts evaluating the literature, our definition was curated from the perspective of healthcare professionals, healthcare students and patients.
This study aims to develop and validate the Multidimensional Clinical Empathy Scale (M-CES) to measure the multidimensional construct of CE among healthcare professionals and students.
Methods
This was a multiphase, mixed-methods instrument development and validation study conducted from January 2021 to December 2023. This study consisted of three phases: item generation and theoretical analysis, item reduction, and validation of the final scale.
While formal sample size calculations are not typically used in scale development, our sample sizes align with established methodological guidelines for scale development. For cognitive interviews, a total of 11 clinicians and educators participated in two rounds of content validation, which is consistent with the recommended range of 5–15 participants for cognitive pretesting. 16 For exploratory factor analysis (EFA), 143 participants were recruited, above the minimum thresholds of at least 100 participants. 17 For confirmatory factor analysis (CFA), 977 responses were analysed, far exceeding the recommended minimum of 300, and falling within the ‘excellent’ range for CFA sample adequacy. 18 These sample sizes reflect the rigour and validity of our study design.
Participants were eligible if they were (1) currently practising as doctors or nurses or (2) enrolled as medical or nursing students. Participants were also required to have sufficient English proficiency to complete the survey.
Responses were excluded if they (1) completed the survey in under 4 min (to account for inattentive or speed responding), (2) failed to complete all M-CES items, or (3) demonstrated extreme disengagement (e.g. selecting the same option across all items without variation).
A summary of the overall scale development process is shown in Figure 1. This flowchart visually presents the key steps undertaken across the three phases of the study—from item generation and content validation to psychometric testing using exploratory and confirmatory factor analyses—providing a comprehensive overview of the methodology used in the development of the M-CES.
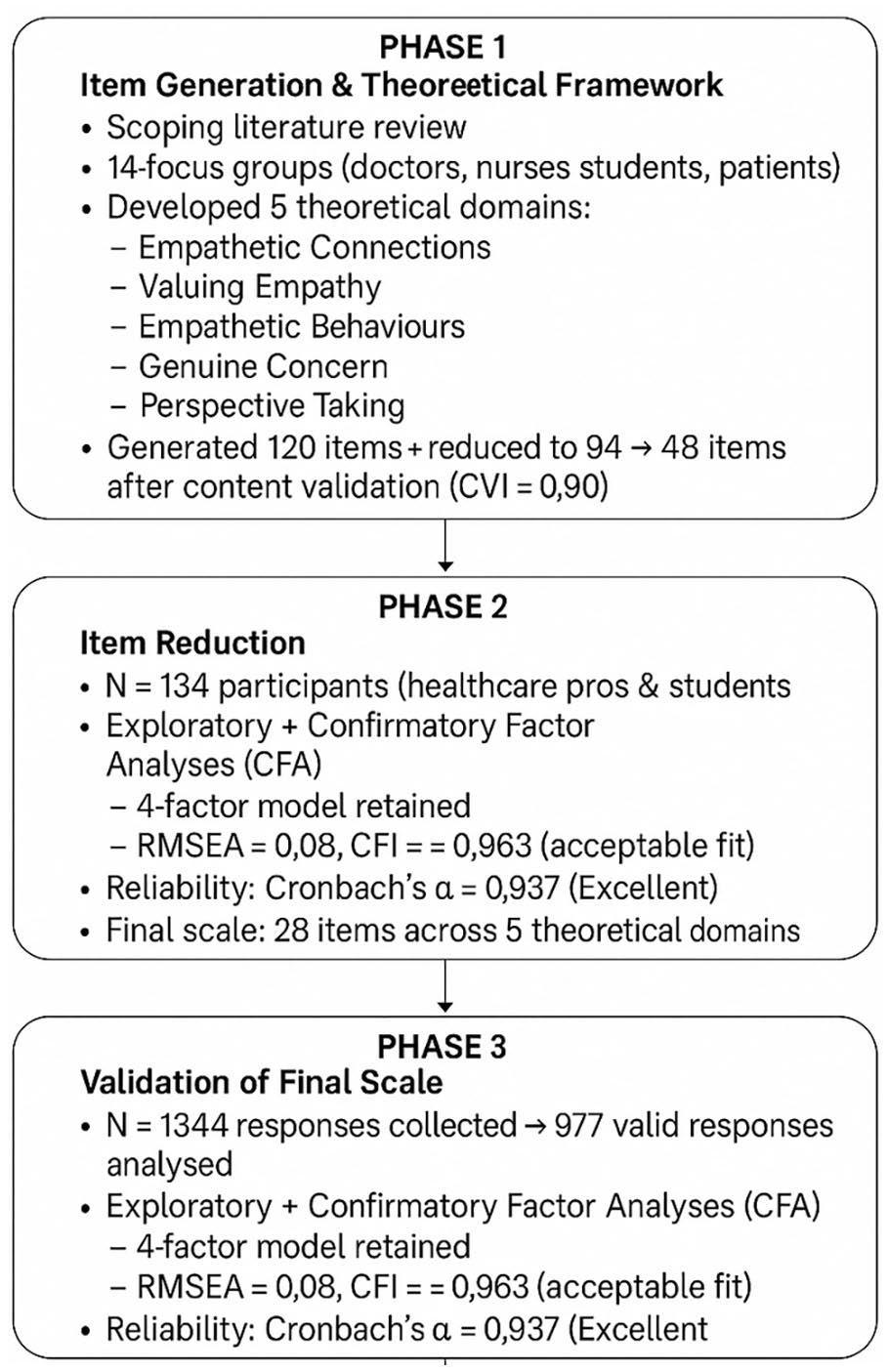
Overview of the M-CES development process.
Phase 1: Conceptual framework and preliminary item development
The process began with a scoping review of existing empathy scales and theoretical frameworks. The theories were tested and conceptualised through 14 focus groups comprising 69 participants, including doctors, nurses, medical and nursing students, and patients. The findings were published separately. 15 These sessions helped define the five key domains of CE:
Empathetic connections: The sense of connection with patients, that is, felt by the healthcare professional or the student.
Valuing empathy: The level of importance placed on CE by the healthcare professional or student.
Empathetic behaviours: The use of body language or behavioural cues to express empathy.
Genuine concern: The feeling of genuine concern for patients.
Perspective taking: The adoption of the patient’s perspective from a psychological and emotional aspect. This can be further subdivided primarily into three subdomains: cognitive, affective, and imaginative.
A multidisciplinary team of clinicians, educators, and researcher (Table 1) used both deductive (from literature) and inductive (from focus group discussions) methods 19 to create an initial 120-item scale. Item lengths were kept below 15 words, and the language used was made simple to understand and pitched at GCE (British General Certificate of Education) O-level English (approximately grade 10). This was subsequently reviewed for clarity and understanding by two medical students who are not part of the research team, leading to a reduction to 94 items.
Specialisation of scale creation and validation team.

Content validity via cognitive interviews
Cognitive interviews 20 were conducted in two rounds, involving 11 clinicians and educators familiar with and likely to have higher levels of CE.21,22 Participants rated the scale for item clarity and relevance to CE on a Likert scale 23 of 1–5. Ratings of 4 and above were considered essential to the construction of the scale. Table 2 shows the Item-level Content Validity Index (CVI) values, 24 which measure the proportion of experts who rated the items as essential were calculated. Items with item-CVI of more than 0.78 were retained. 25 The average CVI of the eventual 48-item scale was high at 0.90. 26
Content validity ratings from cognitive interviews: item-to-total correlations, inter-item averages and Cronbach’s alpha for the 26-item draft M-CES.

M-CES: Multidimensional Clinical Empathy Scale.
Phase 2: Item reduction and creation of the final scale
The 48-item scale (Supplemental Annex 1) was formulated as a survey. The survey was hosted on Qualtrics XM (Qualtrics, Provo, UT, USA) and snowball sampling 27 was used to recruit 143 participants, comprising 77 healthcare professionals and 66 healthcare students. EFA 28 with Promax rotation was conducted using Stata version 14.0 (STATA Corp LLC, TX, USA).
EFA was employed to unveil the underlying factors within the set of observed variables. 29 Promax rotation helped account for potential correlations between factors, providing for a more realistic representation of the latter in the CE scale’s underlying structure. 30 A scree plot (Figure 2) showed 13 factors above the eigenvalue of 1 and a change in plot gradient 31 at the fifth factor, resulting in a retention of five factors. The Kaiser–Meyer–Olkin value of 0.832 indicated the adequacy of the sample size for conducting the EFA. 32 The Bartlett Test of Sphericity 33 yielded a significant result (p < 0.05), indicating that the correlations between variables are sufficiently different from zero to allow for proceeding with factor analysis. The scale was reduced from 48 items to 26 items across the five theoretical domains: Empathetic Behaviours, Empathetic Connection, Valuing Empathy, Genuine Concern, and Perspective Taking.
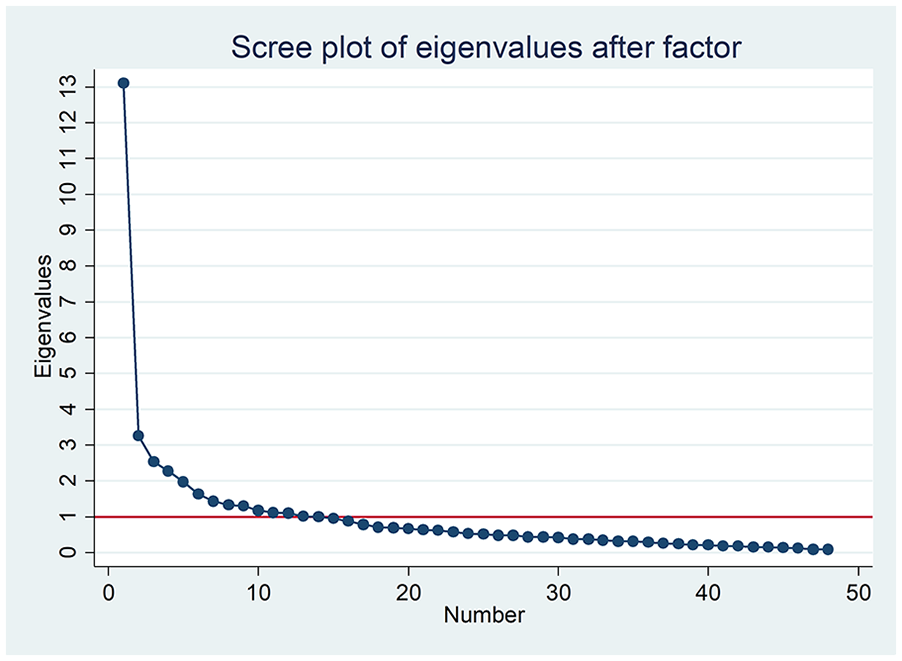
Scree plot of exploratory factor analysis for the initial scale with 48 items.
Phase 3: Testing of the final scale
The final 26-item M-CES (Supplemental Annex 2) were incorporated into a Qualtrics survey that included questions on demographics and the JSE. Snowball sampling was employed to recruit healthcare professionals and students, resulting in 1344 responses. After excluding responses for speed recording, extreme recording, and incomplete responses (Table 3), 977 responses were analysed. The final M-CES score was calculated by adding the individual scores for all 26 questions and dividing by 26, giving a final M-CES score of between 1 and 5, with 5 being the highest score for CE.
Data cleaning process of responses for the final scale.

EFA and CFA on the final scale
EFA with Promax rotation was conducted on the final scale to re-explore underlying factors. The scree plot and parallel analysis (Supplemental Annex 3) suggested that four to five factors should be retained in the model. As such, we conducted an EFA with both four and five factor analysis. The analysis indicated stronger loadings and a closer fit to the four-factor structure.
A CFA on the same dataset was conducted to examine the covariances between factors. The same dataset was used to conduct a CFA on the final scale with four factors. The analysis of the data was done using the lavaan package in R. (v0.6-7; Rosseel 37 ).
Reliability testing
We evaluated the reliability 38 of the scale by calculating the item-to-scale correlation and a Cronbach’s alpha (α), which measures internal consistency. An alpha value exceeding 0.70 was considered adequate for our purposes. 39
Results
Phase 2 results: Reasoning and outcome item reduction with EFA of the initial 48-item scale
EFA with Promax 5’s factor loadings (Supplemental Annex 4) indicated strong associations with four of the five theoretical domains: Empathetic Behaviours, Empathetic Connections, Valuing Empathy, and Genuine Concern. Negatively worded questions formed a separate factor. Perspective Taking didn’t significantly load into any factor.
Items selected for the final scale were indicated, and the reasoning is explained in Supplemental Annex 5. Questions with factor loading of more than 0.6 were included. Selected questions with lower factor loading were retained for their theoretical importance. Negatively worded items were excluded early in the item reduction process due to concerns about respondent misinterpretation and measurement distortion. Studies have shown that reverse-worded items can introduce confusion, particularly among respondents with lower literacy or non-native language proficiency, leading to inconsistent or unreliable responses. 40 These items tended to load onto a separate factor, suggesting that the direction of wording—not the underlying construct of empathy 41 —was influencing responses. Excluding them improved the scale’s clarity and internal consistency. EM44 (‘believes that empathy is something that can be nurtured and developed’) was retained as it was considered important in assessing attitudes towards empathy education.
The ‘Perspective Taking’ domain (EM18–EM25) showed weaker loadings during EFA and did not significantly load into any single factor. However, as this domain is a cornerstone of CE in both theoretical frameworks 42 and widely used scales such as the JSE 43 and IRI, 44 we chose to retain these items for further testing. Eight of the perspective-taking questions were retained in our final scale for further evaluation. The final scale consisted of 26 questions.
Phase 3 results: Factor analysis and reliability testing of final scale
A total of 1344 responses were collected, with 977 responses analysed after excluding 332 for speed recording, 1 for extreme responding style, and 34 for incomplete responses. The demographic breakdown of participants is shown in Table 4. The sample included 36.3% healthcare professionals and 62.5% healthcare students.
Demographic characteristics of participants included in final scale validation (n = 977).

This table presents the demographic distribution of participants across six categories: (1) occupation/profession, (2) age group, (3) sex, (4) ethnicity, (5) education Level, and (6) clinical experience. Participants included medical students, nursing students, doctors, nurses, and others.
The mean M-CES score of participants was 4.17 (95% CI: 4.14–4.20). Healthcare students had a higher mean empathy score (4.22; 95% CI: 4.18–4.25) compared to healthcare professionals (4.1; 95% CI: 4.06–4.14). More students responded positively on the scale compared to professionals (Figure 3).
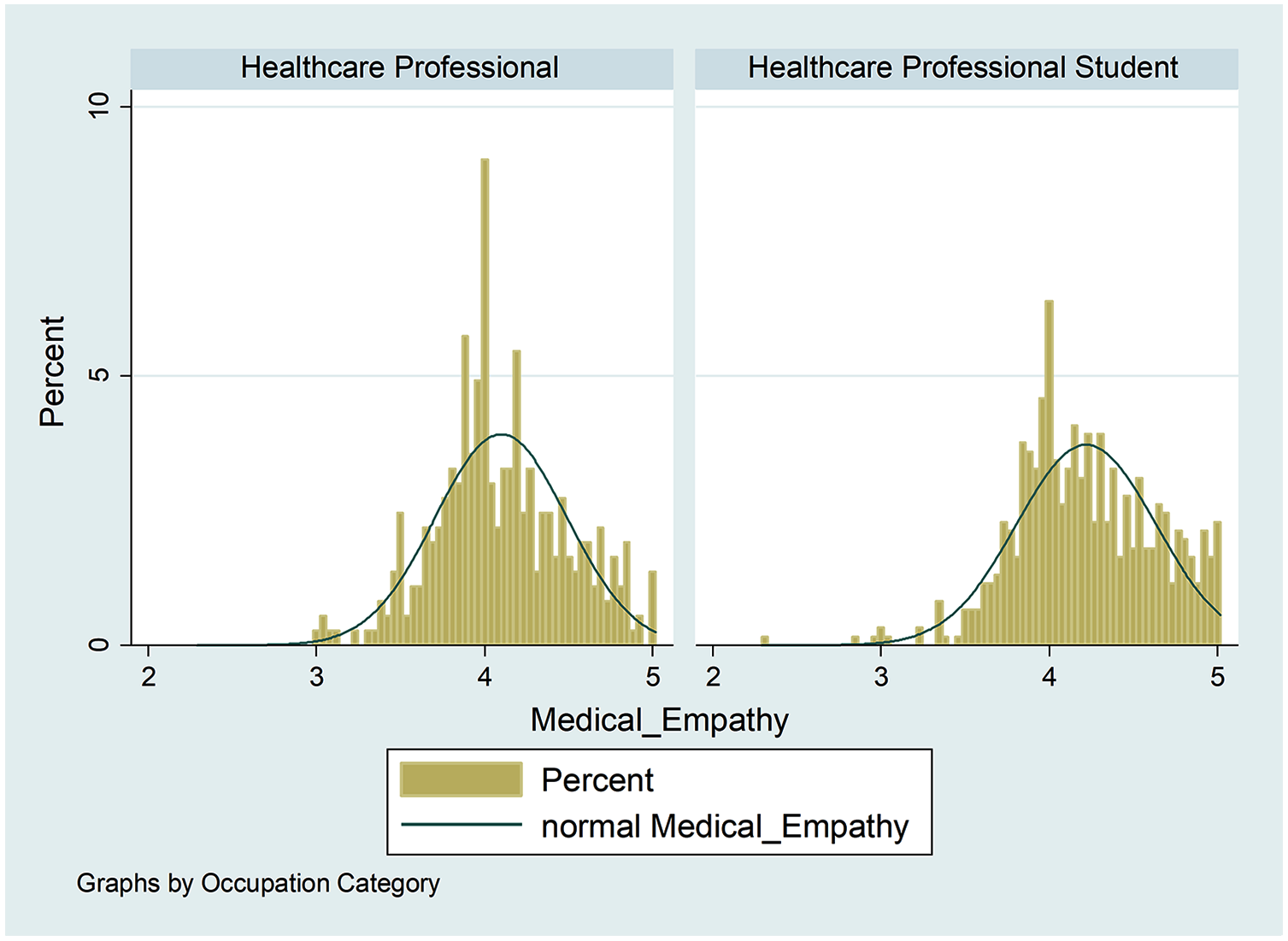
Distribution of mean M-CES scores by participant type (healthcare professionals versus students).
The results of the EFA on the final scale are shown in Supplemental Annex 6. Empathetic Connections, Valuing Empathy and Perspective Taking loaded well into a three-factor model, while Empathetic Behaviours and Genuine Concern combined loaded well into a one factor model. Item 18 (‘feels what my patients are feeling’), initially part of Perspective Taking, was reclassified under Genuine Concern/Empathetic Behaviours.
The CFA results (Supplemental Annex 7) showed a root mean square error of approximation value of 0.80 with a Comparative Fit Index of 0.963, which suggested an acceptable to good fit. The path diagram indicating the factor structure is shown in Figure 4. The highest covariance was between Empathetic Connections and Perspective Taking (0.788), while the lowest covariance was between Empathetic Connections and Valuing Empathy (0.430).

CFA path diagram illustrating the final four-factor model of the M-CES.
The reliability testing results are summarised in Table 5. The average inter-item correlation, which was 0.3723, represented the average pairwise correlation between all items. This is considered appropriate as a correlation of 0.2 suggests poor internal consistency while a correlation of more than 0.5 may suggest that the items are too correlated that they approach redundancy. The Cronbach’s alpha coefficient, computed at 0.9368, demonstrated a high level of internal consistency. A Cronbach’s alpha above 0.9 is considered excellent. 45 These results affirmed the robustness of the scale and its suitability for assessing the target construct.
Final reliability metrics for the 26-item M-CES: item-to-total correlations, inter-item averages and Cronbach’s alpha.

Note. Values reported are based on the full sample of 977 healthcare professionals and students in the final validation phase.
M-CES: Multidimensional Clinical Empathy Scale.
Discussion
The development and validation of the M-CES is a significant advancement in measuring the multidimensional aspects of CE among healthcare professionals and students. This study addressed the limitations of existing scales by incorporating both cognitive and affective dimensions of empathy and employing a rigorous methodological approach.
The development of the M-CES presented in this study distinguishes itself from pre-existing CE scales in four ways: the grounded approach to constructing the theoretical model of the scale, the avoidance of negatively worded items, the inclusion of ‘affective empathy’ as an integral domain of the scale and the scale being validated contextually in healthcare professionals and students, in whom CE matters most.
The study employed a comprehensive process that combined both deductive and inductive methods, based on qualitative insights from healthcare professionals, students and patients. 15 The five domains of the M-CES—Empathetic Connections, Valuing Empathy, Empathetic Behaviours, Genuine Concern and Perspective Taking—were validated through a rigorous process of item reduction, EFA, and CFA. While Perspective Taking showed lower loadings in the EFA, it was retained due to its foundational role in empathy theory and consistent presence in existing validated instruments such as the JSE and IRI. Notably, our CFA affirmed its place within the final four-factor model, supporting its structural validity. Including Perspective Taking enhances the construct validity of the M-CES by explicitly representing the cognitive processes underlying empathic engagement—ensuring the scale comprehensively assesses both cognitive and affective dimensions integral to CE. Our qualitative data also revealed that many healthcare professionals and students equated empathy with the ability to ‘step into the patient’s shoes’, reinforcing the clinical relevance of this domain. The scale’s reliability, with a high Cronbach’s alpha, confirms its suitability for use in healthcare settings.
Our scale utilised positively worded questions, eliminating the cognitive complexity for respondents 46 and the need for reverse scoring during analysis. This approach enhanced reliability 47 and reduced respondent fatigue. 48 Since empathy is a positive trait, it was logical to avoid negatively worded items, which are better suited for measuring negative traits like anxiety. 49
Comparison with existing scales
The domains of the IRI encompass Perspective Taking, Fantasy, Empathetic Concern and Personal Distress. 50 The JSE focusses on three specific domains: Perspective Taking, Compassionate Care and Standing in the Patient’s Shoes. 9 The domains in M-CES in comparison to JSE and IRI are as follows:
Genuine concern: This domain focusses on measuring the authenticity and sincerity of an individual’s concern and care for others. While the IRI and JSE assess certain aspects of concern and compassion, our scale focusses on the genuineness or nature of these feelings and emotions.
Empathetic behaviours: This domain likely evaluates an individual’s observable actions and behaviours that demonstrate empathy. It aligns with the idea of empathetic concern and compassionate care measured in the JSE.
Perspective taking: Perspective taking is a domain in the IRI that assesses an individual’s ability to understand and consider another person’s point of view. It is a key component of empathy. JSE’s ‘standing in patient’s shoes’ corresponds to this domain.
Valuing empathy: This domain assesses the importance or priority an individual places on empathy. It is recognising and valuing the role of empathy in one’s personal and professional life, which is not a domain directly measured in the IRI or JSE.
Empathetic connections: This domain, which is fundamental to empathy, measures an individual’s ability to connect emotionally with others. This measure corresponds to an item in the JSE that refers to ‘establishing a connection with patients’.
M-CES is comprehensive, including domains like Genuine Concern and Valuing Empathy which are not measured by the IRI or JSE. While some scholars argue that affective empathy may hinder clinical decision-making, 51 our grounded perspective 15 and other scholars52,53 suggest that affective empathy does not reduce professionalism or the clinical effectiveness of healthcare professionals. Studies involving both healthcare professionals and patients have highlighted the importance of the emotional aspect of CE and54,55 our factor analysis demonstrated that affective items such as ‘feels what my patients are feeling’ aligned more closely with the domain of Genuine Concern. Empathy must be genuine 56 and empathy, that is, ‘put on’ can be detrimental to the patient-healthcare professional interaction. 57 This underpins the importance of employing both cognitive and affective tools to assess for CE. 58
Implications for healthcare education and practice
M-CES provides educators with a holistic tool to ascertain and monitor the development of CE in practising and prospective healthcare professionals. Since empathy is multidimensional and personalised, 59 having scores for four different domains would allow for a personalised pedagogy 60 to be administered during training. Healthcare professionals and students can identify areas (domains) for improvement and work towards fostering more empathetic patient-provider relationships. For example, individuals who score highly in Genuine Concern but lower in Perspective Taking may benefit from role-playing 61 or narrative teaching 62 that simulate complex emotional contexts. Conversely, someone who excels in aspects such as Perspective Taking but scores lower in Empathetic Behaviours may benefit from training that focusses on verbal and non-verbal communication skills, such as active listening and compassionate body listening. 63 For those who score lower in Valuing Empathy, interventions may include modules that discuss the ethical foundations of empathy, highlight patient testimonials or include mentorship programmes with clinicians who model empathetic practice. This domain-specific insight allows clinical educators and trainers to shift away from one-size-fits-all empathy curricula towards more targeted, competency-based interventions that address individual developmental needs.
The M-CES serves as a tool for research on the barriers, enablers, drivers and impact of the multidimensional construct of CE. An example would be to study the association between empathy and burnout. The results of correlational studies between empathy and burnout have been mixed. 64 Some scholars have suggested that affective rather than cognitive empathy contributes to the causation of burnout in healthcare workers. 65 The latter would be difficult to prove with the current scales such as JSE. Currently available studies did not differentiate between the components of empathy and their relationship with burnout, 66 likely due to the lack of clear domains embedded within the scale. The M-CES, with its multidimensional approach, could help clarify the role of different empathy components in burnout, leading to better management strategies for healthcare workers.
Limitations and future research directions
While our CFA was conducted on a large sample of 977 participants—exceeding the commonly recommended minimum of 500 for robust CFA models 18 —the EFA was performed on a smaller sample of 143 participants. Conventional guidelines 67 typically suggest a minimum of 5–10 participants per item, or at least 200 participants in total, to ensure factor stability in EFA. Given the initial pool of 48 items, our EFA sample fell short of these thresholds. This may have limited the stability and generalizability of the factor solution derived from the EFA. Nonetheless, the CFA findings on a larger, independent sample provided stronger evidence to support the final factor structure.
As snowball sampling was employed, there is a potential for sampling bias. This may have resulted in an over-representation of individuals within certain professional or institutional networks, which could limit the generalizability of our findings to healthcare professionals and students outside these circles. Given the cultural nuances 68 in how empathy is perceived and expressed, future research should focus on cross-cultural validation of the M-CES. While the current study included participants from Singapore’s multicultural society, it is important to assess the scale’s applicability in other cultural contexts. Potential regions for validation include East Asia (e.g. Japan, China), South Asia (e.g. India, Sri Lanka), the Middle East, and Western countries (e.g. the United States, the UK). Such studies would ensure the tool’s adaptability and validity across healthcare systems with different norms and communication practices. In this study, we reported on internal consistency, convergent validity, and construct validity but did not assess criterion validity, predictive validity, or test-retest reliability. To advance the validation of the M-CES, a structured psychometric evaluation framework is recommended. First, test-retest reliability should be assessed over a 3- to 6-month interval to evaluate score stability. Second, predictive validity can be explored by correlating M-CES scores with relevant clinical outcomes, such as patient satisfaction, communication ratings or empathy-related behaviours observed in practice. Third, responsiveness should be assessed through pre- and post-intervention studies to determine the scale’s sensitivity to empathy training or educational programmes. Collectively, these steps would provide a robust roadmap to support the scale’s future use in both research and routine training settings.
While the M-CES is a valuable tool for measuring the multidimensional aspects of CE, existing tools like the IRI and JSE remain relevant for scholars who focus on cognitive empathy or apply them in non-healthcare settings.
Conclusion
The M-CES represents a significant advancement in the measurement of CE, offering a comprehensive and multidimensional tool tailored to healthcare professionals and students. Its rigorous development process, inclusion of affective empathy and avoidance of negatively worded items set it apart from existing scales. The M-ACES has the potential to enhance empathy training, improve patient care and contribute to research on empathy and its impacts in healthcare.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251365011 – Supplemental material for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students
Supplemental material, sj-docx-1-smo-10.1177_20503121251365011 for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students by Laurence Tan, Chou Chuen Yu, Robin Choo, Mai Khanh Le, Reuben Ng, Tanya Tierney, Evelyn Lim, Daphne Lim, Sok Ying Liaw, Gurpreet Hansra, Yun Ying Ho, Colin Ngeow, Siew Chin Chia and James Alvin Low in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121251365011 – Supplemental material for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students
Supplemental material, sj-docx-2-smo-10.1177_20503121251365011 for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students by Laurence Tan, Chou Chuen Yu, Robin Choo, Mai Khanh Le, Reuben Ng, Tanya Tierney, Evelyn Lim, Daphne Lim, Sok Ying Liaw, Gurpreet Hansra, Yun Ying Ho, Colin Ngeow, Siew Chin Chia and James Alvin Low in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121251365011 – Supplemental material for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students
Supplemental material, sj-docx-3-smo-10.1177_20503121251365011 for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students by Laurence Tan, Chou Chuen Yu, Robin Choo, Mai Khanh Le, Reuben Ng, Tanya Tierney, Evelyn Lim, Daphne Lim, Sok Ying Liaw, Gurpreet Hansra, Yun Ying Ho, Colin Ngeow, Siew Chin Chia and James Alvin Low in SAGE Open Medicine
Supplemental Material
sj-docx-4-smo-10.1177_20503121251365011 – Supplemental material for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students
Supplemental material, sj-docx-4-smo-10.1177_20503121251365011 for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students by Laurence Tan, Chou Chuen Yu, Robin Choo, Mai Khanh Le, Reuben Ng, Tanya Tierney, Evelyn Lim, Daphne Lim, Sok Ying Liaw, Gurpreet Hansra, Yun Ying Ho, Colin Ngeow, Siew Chin Chia and James Alvin Low in SAGE Open Medicine
Supplemental Material
sj-docx-5-smo-10.1177_20503121251365011 – Supplemental material for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students
Supplemental material, sj-docx-5-smo-10.1177_20503121251365011 for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students by Laurence Tan, Chou Chuen Yu, Robin Choo, Mai Khanh Le, Reuben Ng, Tanya Tierney, Evelyn Lim, Daphne Lim, Sok Ying Liaw, Gurpreet Hansra, Yun Ying Ho, Colin Ngeow, Siew Chin Chia and James Alvin Low in SAGE Open Medicine
Supplemental Material
sj-docx-6-smo-10.1177_20503121251365011 – Supplemental material for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students
Supplemental material, sj-docx-6-smo-10.1177_20503121251365011 for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students by Laurence Tan, Chou Chuen Yu, Robin Choo, Mai Khanh Le, Reuben Ng, Tanya Tierney, Evelyn Lim, Daphne Lim, Sok Ying Liaw, Gurpreet Hansra, Yun Ying Ho, Colin Ngeow, Siew Chin Chia and James Alvin Low in SAGE Open Medicine
Supplemental Material
sj-docx-7-smo-10.1177_20503121251365011 – Supplemental material for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students
Supplemental material, sj-docx-7-smo-10.1177_20503121251365011 for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students by Laurence Tan, Chou Chuen Yu, Robin Choo, Mai Khanh Le, Reuben Ng, Tanya Tierney, Evelyn Lim, Daphne Lim, Sok Ying Liaw, Gurpreet Hansra, Yun Ying Ho, Colin Ngeow, Siew Chin Chia and James Alvin Low in SAGE Open Medicine
Supplemental Material
sj-docx-8-smo-10.1177_20503121251365011 – Supplemental material for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students
Supplemental material, sj-docx-8-smo-10.1177_20503121251365011 for Development and validation of the Multidimensional Clinical Empathy Scale for healthcare professionals and students by Laurence Tan, Chou Chuen Yu, Robin Choo, Mai Khanh Le, Reuben Ng, Tanya Tierney, Evelyn Lim, Daphne Lim, Sok Ying Liaw, Gurpreet Hansra, Yun Ying Ho, Colin Ngeow, Siew Chin Chia and James Alvin Low in SAGE Open Medicine
Footnotes
Acknowledgements
We are indebted to Apphia Tan Jia Qi for reviewing the article.
ORCID iDs
Ethical considerations
Ethics approval for this study was granted by the National Health Group Domain Specific Review Board (DSRB), reference 2019/00458. All procedures followed the ethical standards and guidelines specified by the institutional review board.
Consent to participate
As this was an anonymous survey, explicit written informed consent was not required by the DSRB. Instead, implied consent was obtained from all participants, who indicated their consent by voluntarily agreeing to participate after reviewing the participant information sheet provided at the beginning of the online survey.
Author contributions
Drs. Laurence Tan and Chou Chuen Yu had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Laurence Tan, James Alvin Low, Chou Chuen Yu, Robin Choo, Mai Khanh Le, Reuben Ng. Acquisition, analysis and interpretation of data: Laurence Tan, Chou Chuen Yu, Robin Choo, James Alvin Low, Mai Khanh Le, Reuben Ng, Tanya Tierney, Evelyn Lim, Daphne Lim, Sok Ying Liaw, Gurpreet Hansra, Yun Ying Ho, Colin Ngeow. Drafting of the article: Laurence Tan and Yu Chou Chuen, and Robin Choo. Critical revision of the article for important intellectual content: Laurence Tan, James Alvin Low, Chou Chuen Yu, Robin Choo, Mai Khanh Le, Reuben Ng, Tanya Tierney, Evelyn Lim, Daphne Lim, Sok Ying Liaw, Gurpreet Hansra, Yun Ying Ho, Colin Ngeow. Statistical analysis: Robin Choo, Chou Chuen Yu, Laurence Tan. Obtained funding: Laurence Tan, James Alvin Low. Study supervision: Tan, James Alvin Low, Chou Chuen Yu.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Geriatric Education and Research Institute’s intramural fund (reference number GERI/1616).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.