
Abstract
Background:
Evidence-based practice is defined as using the best available research and clinical evidence by incorporating patients’ values and preferences for their health needs. The use of evidence-based intrapartum care practices is an essential tool to improve the quality of obstetrics care.
Objective:
The primary objective of this study was to determine the prevalence of evidence-based intrapartum care and associated factors among obstetrics care providers in Ethiopia.
Method:
Important articles were retrieved from universally accepted and used databases, including Cochran, PubMed, HINARI, Google Scholar, Web of Science, African OnLine, and repositories of Ethiopian Universities. We extracted articles by using a standard JOANNA Briggs Institute data extraction sheet. To determine the existence of heterogeneity in studies, I2 statistics and Cochran Q tests were used. The publication bias of the included studies was checked using Egger’s test and a Funnel plot.
Result:
A total of 2035 obstetrics care providers were involved in this systematic review and meta-analysis. The estimated overall rate of evidence-based intrapartum care practice in Ethiopia was 54.45% (95% CI: 43.06, 65.83); I2 = 96.6%, p < 0.001). The studies with a sample size greater than 300 count for 47.25% (95% CI: 36.14, 65.83). Whereas obstetrics care providers have a decent knowledge of intrapartum care evidence 3.31 times, a positive attitude toward evidence 3.34 times, training 2.21 times, and work experience ⩾5 years 3.31 times associated with the practice of evidence-based intrapartum care.
Conclusion:
The overall practice of evidence-based intrapartum care among obstetrics workers in Ethiopia is estimated to be low. Therefore, there should be a focused effort on training and disseminating protocols and guidelines to enhance knowledge and foster a positive attitude among obstetrics care providers. Additionally, the Ethiopian government should prioritize the implementation of the 2021 to 2025 National Health Equity Strategic Plan to achieve its objective of improving the quality of health services.
Introduction
Evidence-based practice (EBP) is the use of available research and clinical evidence to incorporate patients’ values and improve their health needs. 1 It includes companionship and continuous follow-up throughout labor, oral rehydration during the first stage of labor, ambulation during the first stage, restriction of practice of routine episiotomy, active management of the third stage of labor, vaginal examination every 4 h, encouraging mobility of the women, immediate postnatal assessment, frequent monitoring of the fetal heart rate, delayed cord clamping, and immediate newborn assessment and care.2,3 Its package in obstetrics care services helps advance the quality of obstetrics care, increases institutional delivery, and enhances women’s acceptance and satisfaction with services. 4
Nearly 95% of maternal deaths occur in low and middle-income countries, with Sub-Saharan Africa and Southern Asia accounting for about 87% of global maternal deaths. Despite the region’s high Maternal Mortality Ratio (MMR), Sub-Saharan Africa achieved a notable 33% reduction in MMR between 2000 and 2020. 5 During the period of labor and delivery, a large number of healthy pregnant women require and experience at least one clinical intervention for better maternal and fetal outcomes, such as operative vaginal birth, labor induction, augmentation, cesarean section, or episiotomy.6,7
However, mothers in normal labor and delivery continue to be exposed to non-evidence-based intrapartum practices.8,9 In Sub-Saharan African countries, the prevalence of operative vaginal delivery is approximately 7.98%. 10 According to a systematic review and meta-analysis (SRMA), the practice of episiotomy in Ethiopia stands at 45.11%. 11 Non-evidence-based intrapartum practices lead to maternal complications such as injury to the anal sphincter, increased cesarean section rate, postpartum infection, fundal pressure, episiotomy, and others. In addition, non-evidence-based intrapartum care practice can cause neonatal complications including birth trauma, episiotomy-related injuries, fundal pressure-related risks, and long-term health implications.11,12
The World Health Organization (WHO) stresses the importance of replacing ineffective and harmful clinical intrapartum interventions with EBPs to enhance positive birth outcomes and experiences, ultimately reducing maternal and child mortality and morbidity. 13 To achieve this, obstetrics care providers (OCPs) need to be educated, mentored, and trained in the necessary skills for managing pregnancies, childbirth, and postnatal care. This includes early recognition and management of complications to ensure the delivery of high-quality care.14,15 The attempt to change the OCP’s routine ineffective and harmful obstetrics interventions with current best and recommended intrapartum EBPs is challenging and requires time and process. The behavioral change of the healthcare provider is a complex course and the change of the problem may vary in groups of healthcare providers, clinical environments, or clinical practices.16,17
Moreover, there are initiatives and interventions to increase pregnant women’s institutional delivery to keep the well-being of the women and children through skilled care providers and on-time referral of obstetrics complications in the last couple of decades. However, accessing labor and delivery care services in a healthcare facility may not pledge evidence-based or good quality obstetrics care.17,18 Despite an increase in institutional delivery in Ethiopia from 16.8% in 2010 to 28% in 2016, only 38.2% of the care is supported by evidence of intrapartum care practice.19,20 Generally, unsafe intrapartum care practices and poor quality obstetrics care endure despite best practice activities.21,22 Therefore, this SRM was designed to evaluate the prevalence of evidence-based intrapartum care among OCPs and associated factors in Ethiopia.
Research questions
What is the proportion of OCPs practicing evidence-based care (EBC) during the intrapartum period in Ethiopia?
What are the factors associated with the practice of EBC during the intrapartum period in Ethiopia?
Methods
This study is an SRMA performed in accordance with the guidelines specified in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). Since our study did not involve human or animal trials, ethical board approval was not required. This study was conducted from September to December 2024.
Study setting
We incorporated only studies done in Ethiopia.
Search strategy
The search for appropriate articles was conducted on the practice of EBC during the intrapartum period, we used acceptable international databases including PubMed, HINARI, Google Scholar, Cochran, Web of Science, African OnLine, and repositories of Universities in Ethiopia. The keywords and MeSH terms used while searching the relevant articles include EBP, intrapartum care, parthograph use, obstetric care provider, midwifery, nurse, obstetrician, gynecologist, health extension workers, and Ethiopia and other connected terms. The Boolean Operator “AND” and “OR” are used for a combination of the above Keywords and MeSH terms.
Inclusion and exclusion criteria
The selected articles provided an overview of the prevalence of evidence-based intrapartum care (EBIPC) practice and its determinants among OCPs in Ethiopia. Subsequently, we assessed the quality and relevance of these articles using the updated PRISMA (2020) standard guideline for reporting systematic reviews. 23 Then the articles with low risk according to the standard rating were included in the final report of the findings. In addition, the articles and literature in the English language were encompassed. Furthermore, those articles with incomplete abstracts that conveyed their findings other than the outcome of interest were excluded.
Quality assessment
Following identifying pertinent articles for our study, we proceeded with the critical steps of quality assessment for our SRMA. To this end, we employed the Joan Briggs Institute (JBI) checklist for an analytic cross-sectional study. 24 Two authors (ZF and AGZ) autonomously conducted the evaluation of individual articles and literature. Any disagreements that arose between their independent reviews were resolved by a third author (AA). A consensus was reached after resolving disagreements and the quality of articles and literature was identified. We included all items of the analytic cross-sectional studies as outlined in the JBI checklist, which serves as the foundation for identifying quality articles. The primary item assessed the presence or absence of clear inclusion criteria. The second item evaluated the availability of an appropriate description of the study subject and setting. The third item focused on the validity and reliability of measurements. The fourth item assessed whether the objectives and standards were adequately described. Identification of confounders during data analysis constituted the fifth item on the checklist. The sixth item pertained to the use of a suitable approach to control confounders. The seventh item evaluated the reliability and validity of outcome measurements. Lastly, the appropriateness of the statistical analysis method was assessed. Articles meeting at least 50% of the standard JBI checklist criteria for independent articles were considered low-risk and included in the review.
Data extraction
For the data exportation, we used Endnote version X8 software. Next to that the exported data was entered into a Microsoft Excel spreadsheet for the removal of the duplication. The data was independently extracted by the first and second authors (ZF, AGZ) in a standardized JBI data format.
Measurement of outcome
According to this study, there are two important outcome variables for measurement. The primary outcome variable was the magnitude of the OCPs practicing EBC during the intrapartum period and the second measurement outcome variable was the determinants of practicing EBC during the intrapartum period among OCPs.
Evidence-based intrapartum practice
Defined as adhering to WHO recommendations, evidence-based intrapartum practice encompasses utilizing specified interventions at different stages of labor. This includes employing the partograph and encouraging mobility during the first stage, allowing women to choose their birth position during the second stage, administering prophylactic antibiotics in the third stage, and implementing newborn care practices such as immediate covering, delayed umbilical cord clamping, initiating skin-to-skin contact, and early breastfeeding. Additionally, it involves permitting labor companions and ensuring respectful maternity care.25,26
Factors associated with the practice of EBC during the intrapartum period
These were defined as the factors that result in the poor practice of EBIPC practice among OCPs including age, sex, educational level, training, year of experience, shift, patient flow, knowledge, attitude availability of internet connection, availability of the guidelines, and protocols.
Data analysis
To assess publication bias, we employed a Funnel plot and Eggers regression test. 27 The heterogeneity of the studies was examined to gauge the impact of individual study results on the overall findings, using tests such as I-squared statistics and Cochrane Q-test. We utilized a weighted inverse variance random-effects model to estimate the overall pooled analysis. 28 The choice between fixed-effect or random-effect models for analyzing factors associated with EBIPC practices depended on the presence or absence of study heterogeneity. Statistical analysis was conducted using Stata v.16 software (statacorp, College Station, TX, USA). Results were presented using forest plots, text, and tables. Finally, the overall pooled point prevalence of EBIPC practice during intrapartum care, along with a 95% confidence interval (CI), was reported.
Results
The features of the incorporated studies
After a rigorous search for the relevant articles using reputable and accepted international databases including PubMed, HINARI, Google Scholar, Cochran, Web of Science, African OnLine, and repositories of Universities in Ethiopia, a total of 469 articles published on the practice of EBC during the intrapartum period and associated factors in Africa were identified and retrieved. Next, after removing the duplications by Microsoft Excel software, 305 articles were left for assessment of the titles and abstracts. Then those articles underwent the evaluation of their titles and abstracts, and after that, 153 articles that have direct relations with EBIPC practice were selected. By keeping track of the PRISMA flow chart to obtain the best quality articles on EBIPC practice, out of the remaining 78 articles, they underwent full-text assessment for their quality to be included for final review. Therefore, a total of seven articles conducted in Ethiopia on the practice of EBC during the intrapartum period were included in the final SRMA (Figure 1 and Table 1).

PRISMA flow chart of study selection for systematic review and meta-analysis of evidence-based intrapartum care practice and associated factors in Ethiopia.
The features of the studies involved in a meta-analysis of the practice of evidence-based care during the intrapartum period in Ethiopia.

The practice of EBC during intrapartum period in Ethiopia
We used forest plots to present the overall pooled practice of EBC during the intrapartum period in Ethiopia (Figure 2). Therefore, according to this SRMA, the overall pooled estimated practice of EBIPC among OCPs in Ethiopia was 54.45 (95% CI; 43.06, 65.83); I2 = 96.6%, p < 0.001).
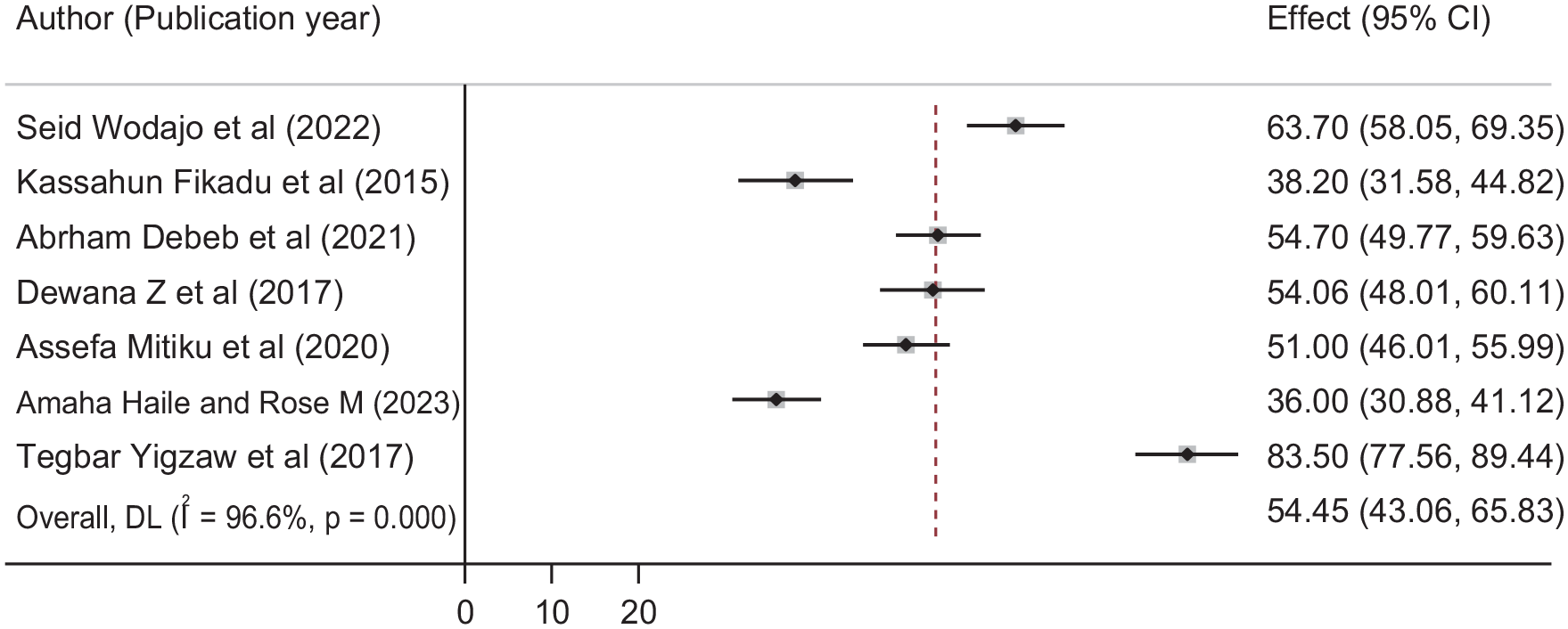
Forest plot of the magnitude of the obstetrics care providers practicing EBIPC with corresponding 95% CIs of 10 studies.
Publication bias
We carried out the check of publication bias using a funnel plot to determine the asymmetric distribution of the practice of EBC during the intrapartum period through visual inspection (Figure 3). According to Egger’s regression test, a p-value was 0.707 which indicated no publication bias.
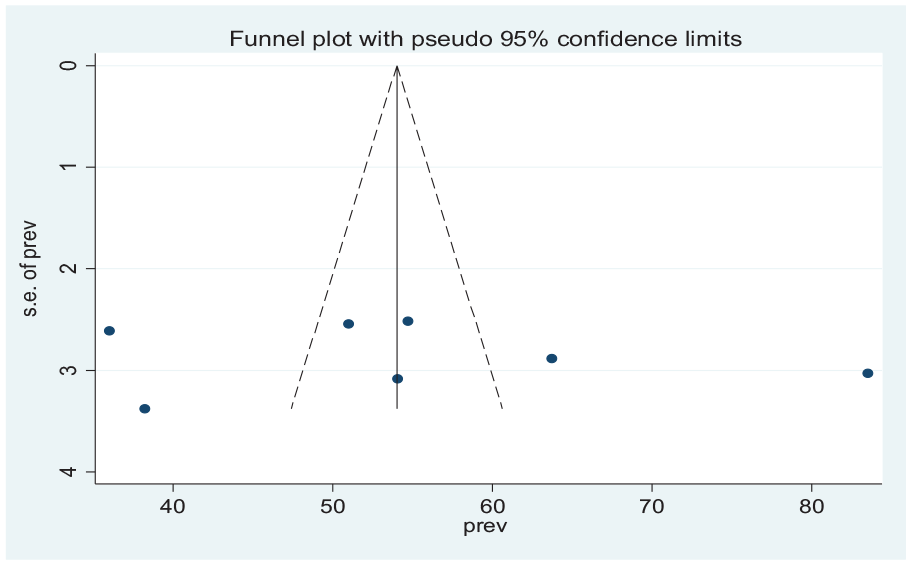
Funnel plot for test of the publication bias for evidence-based intrapartum care practice.
Subgroup analysis
The subgroup analysis was conducted based on the sample size of the studies using the analysis method of random effect size. We computed the subgroup because of the Cochrane I2 statistic (= 96.6%, p < 0.001) which shows the presence of marked heterogeneities within studies. So, the practice of EBIPC with a sample size of less than 300 becomes 59.9% (95% CI: 41.87, 77.93) whereas the studies with a sample size greater than 300 become 47.25% (95% CI: 36.14, 65.83) (Figure 4).

Forest plot of the subgroup analysis based on sample size of the studies.
Factors associated with EBIPC practice
We found four important factors, including having good knowledge, a positive attitude, training, and work experience greater than 5 years are associated with the practice of EBC during the intrapartum period.
Association between good knowledge and EBIPC practice
Three studies showed an association between EBIPC practice and OCP’s knowledge of evidence.25,29,30,32 The odds of the health care provider having good knowledge of evidence are 3.31 (odds ratio (OR): 3.31, 95% CI: 2.62, 4.19) time more practicing EBIPC than that obstetric worker with poor knowledge of the evidence. There is no evidence of the heterogeneity (I2 = 0.0%, p = 0.685). So fixed-effect model analysis was computed (Figure 5).

Forest plot showing the association between evidence-based intrapartum care practice and obstetrics care provider’s good knowledge of evidence.
OCP’s positive attitude on EBIPC practice
Three studies fall under this category.25,29,32 Accordingly, the possibility of practicing EBIPC among obstetric providers having a positive attitude was 3.34 (OR: 3.34, 95% CI: 2.05, 5.11) times higher than obstetric providers having a negative attitude toward EBIPC. As a result of the presence of heterogeneity in the studies (I2 = 57.9%, p = 0.093), we preferred to use the random effect model in this meta-analysis (Figure 6).
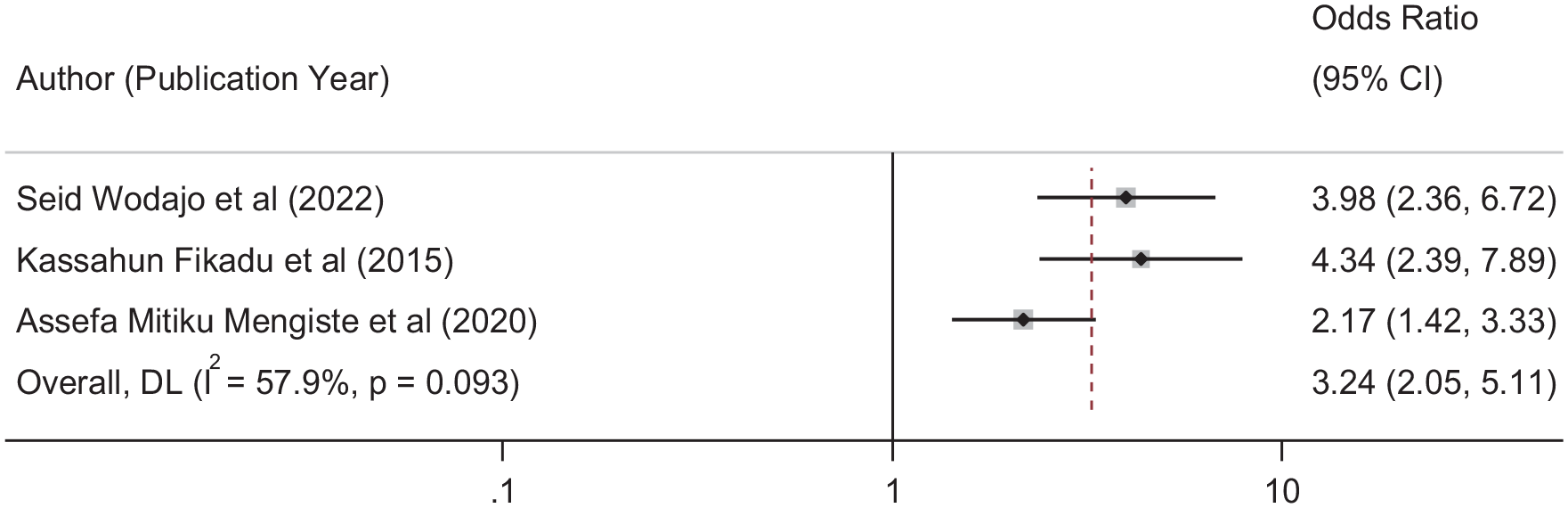
Forest plot showing the association between evidence-based intrapartum care practice and obstetrics care providers’ positive attitude toward evidence.
Association between training and EBIPC practice
Three studies are associated with this.29,30,32 The likelihood of practicing the EBIPC by OCPs having on and off obstetrics and new-born-related training on the care evidence is 2.21 times (OR; 2.21, 95% CI: 1.46, 3.37) than those OCPs. This meta-analysis has heterogeneity in the studies (I2 = 60.2%, p = 0.081). Therefore, we used the weights from the random effect model (Figure 7).

Forest plot showing the association between evidence-based intrapartum care practice and obstetrics care provider’s training.
Association between work experience and EBIPC practice
We found two studies to be included here.25,30 The obstetrics worker with work experience of more than 5 years practices EBIPC 3.31 (OR: 3.31, 95% CI: 2.26, 4.39) times higher than obstetric care providers with work experience of less than 5 years. There is no heterogeneity of the (I2 = 0.0%, p = 0.373) we applied the fixed-effect model.
Discussion
Ethiopia has made notable progress in lowering maternal and child mortality and morbidity rates. Despite this, there remains a challenge in ensuring that deliveries occur in healthcare facilities under the care of skilled attendants. Enhancing the quality of obstetric and newborn care to increase institutional deliveries and maternal contentment is a key focus for both the WHO and the Ethiopian Ministry of Health. To further decrease maternal and child mortality rates, it is imperative to implement improved EBPs during the intrapartum period within obstetric care services.
As per the current SRMA, the overall aggregated practice of EBIPC among obstetrics practitioners was found to be 54.45 (95% CI: 43.06, 65.83), with a high level of heterogeneity (I2 = 96.6%, p < 0.001). This indicates that roughly half of obstetric care providers adhere to the best practices recommended by the WHO for intrapartum care. There are no other studies reporting a similar rate of EBIPC practice among obstetrics workers. However, other studies have reported higher rates of EBIPC practice compared to the current findings, such as in Kenya 62%, 35 Benin 70.1%, Ecuador 77.6%, Jamaica 81.1%, Rwanda 65.0%, 36 studies in Arab countries found that 82% in Lebanon, 60% in Egypt, and 73% in Syria, 37 California USA (74.4%), 38 and Iran 78%. 39 Discrepancies in findings may stem from variations in study population, sample size, methodology, data collection tools, and the quality of healthcare institutions. Additionally, the ratio of laboring women to OCPs may pose challenges in consistently applying intrapartum care elements to each woman. Conversely, the observed rate is higher than that reported in studies conducted in Cameroon 3.8% 40 and Sweden 22.7%, 41 possibly due to differences in data collection methods, study populations, and tools.
The probability of obstetrics workers practicing EBIPC is 3.31 times higher among those with good knowledge of WHO-recommended intrapartum care evidence compared to those with poor knowledge. This finding is supported by studies conducted in Kenya, 35 Cameroon, 40 Iran, 16 and the USA. 42 This result was strengthened by studies done in Kenya, 35 Cameroon, 40 Iran, 18 and the USA. 42 Adequate information and understanding of optimal obstetric practices likely enable workers to enhance their skills and effectively implement EBIPC protocols.
In our research, we discovered that obstetric care providers who hold a positive attitude toward practicing EBIPC are 3.34 times more likely to implement intrapartum care compared to those with a negative attitude toward the evidence. This finding is corroborated by studies conducted in Iran, 16 and the USA. 38 Our finding is supported by a study conducted in Iran, 18 and the USA. 38 The rationale behind this could be that care providers with positive attitudes toward the evidence are inclined to develop the essential skills and motivation required to fulfill their professional responsibilities effectively.
Conversely, obstetric care providers who have undergone training are 2.21 times more likely to practice EBIPC compared to those without training. This finding is consistent with studies conducted in Cameroon, 40 Iran, 16 and Sweden. 41 The rationale behind this association could be that training enhances their understanding of the components of WHO EBP recommendations and their significance in reducing maternal and newborn morbidity and mortality.
The likelihood of obstetrics care workers practicing EBIPC increases by 3.31 times among those with over 5 years of work experience compared to their counterparts with less than 5 years of experience. This finding is supported by studies conducted in Cameroon, 40 the Netherlands, 43 Iran, 16 and Iceland. 44 The rationale behind this observation may lie in the fact that obstetrics workers with greater clinical experience tend to develop advanced skills in service delivery. Additionally, with more years of service, they are exposed to various discussions and training sessions on obstetric care, which further enhances their ability to provide comprehensive and accepted practices of intrapartum care, ultimately improving the quality of care for women and newborns. The heterogeneity observed in this SRMA could be attributed to differences in study design, settings, and sample sizes across the studies included.
Limitations of the study
Comparing the rate of obstetric care providers’ practice of EBIPC to that of larger obstetric care providers is challenging. The national representativeness of the data may be questioned due to its limitation to only four regions of Ethiopia.
Conclusion
The overall practice of EBIPC among obstetric care providers in Ethiopia was found to be low. However, those with good knowledge, a positive attitude, training, and more than 5 years of work experience demonstrated higher odds of practicing EBIPC. This lower practice highlights the poor quality of obstetric care provided to women in Ethiopia, leading to maternal and neonatal complications and reduced satisfaction with services. Therefore, there should be a concerted effort to prioritize training and disseminating protocols and guidelines to enhance the knowledge and foster a positive attitude among obstetric care providers. This would ultimately improve the quality of care provided to women during childbirth and positively impact maternal and neonatal health outcomes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241261210 – Supplemental material for Evidence-based intrapartum care practice and associated factors among obstetrics workers in Ethiopia, systematic review and meta-analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121241261210 for Evidence-based intrapartum care practice and associated factors among obstetrics workers in Ethiopia, systematic review and meta-analysis by Zerihun Figa, Addisu Getinet Zemeskel, Asrat Alemu and Mesfin Abebe in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241261210 – Supplemental material for Evidence-based intrapartum care practice and associated factors among obstetrics workers in Ethiopia, systematic review and meta-analysis
Supplemental material, sj-docx-2-smo-10.1177_20503121241261210 for Evidence-based intrapartum care practice and associated factors among obstetrics workers in Ethiopia, systematic review and meta-analysis by Zerihun Figa, Addisu Getinet Zemeskel, Asrat Alemu and Mesfin Abebe in SAGE Open Medicine
Footnotes
Acknowledgements
None.
Author contributions
ZF and AGZ: Conceived and designed the method, analyzed and interpreted the data. AA and MA: materials, analysis tools, or data and wrote the article.
Availability of data and materials
All related data has been presented within the article. The dataset supporting the conclusions of this article is available from the authors on request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.