
Abstract
Objective:
This systematic review and meta-analysis will investigate the pooled knowledge level of obstetric danger signs and related factors among African women.
Design:
Systematic review and meta-analysis incorporating cross-sectional, case–control, and cohort study designs.
Methods:
Studies published with full texts in English language from the beginning to the present will be searched in the PubMed/MEDLINE, Cumulative Index to Nursing & Allied Health Literature, African Journals Online, and Google Scholar databases. Checklists from the Joanna Briggs Institute will be used to assess the quality of the studies’ methodology. Data extraction, critical appraisal, and screening of all retrieved articles will be conducted by two independent reviewers. Statistical analysis will be performed using the STATA-14 and Review Manager 5.3 (RevMan 5.3) software packages. A random effect will be employed to demonstrate pooled estimates of knowledge among women. For determinants of knowledge, an effect size with a 95% confidence interval will be analyzed.
Protocol Registration:
This systematic review and meta-analysis protocol was registered in PROSPERO with the registration ID and link as follows: CRD42022379085; CRD register@york.ac.ukhttps://www.york.ac.uk/inst/crd
Discussion:
Women who are more knowledgeable about obstetric danger signs are more likely to seek emergency care on time, closely attend antenatal care, and be better prepared for labor and any complications, which reduces both maternal and child mortality. This analysis will provide evidence of the pooled prevalence of knowledge of obstetric danger signs among African women, as well as contributing factors.
Introduction
Obstetric danger signs are those symptoms and signs that may indicate danger to pregnant mothers throughout pregnancy, childbirth, or after childbirth, and if not managed early, lead to obstetric complications and maternal death.1–3 Excessive vaginal bleeding, hand or face swelling, severe abdominal pain, persistent backache, persistent nausea and vomiting, decreased fetal movements, blurred vision, and convulsions are danger signs during pregnancy4–7 whereas excessive vaginal bleeding, extended labor (more than 12 h), retained placenta (more than 1 h), premature rupture of membrane, fetal malposition, and convulsions are danger signs during labor and delivery.4,8,9 Danger signs during the postpartum period include severe vaginal bleeding following childbirth. In addition, foul-smelling discharge from the vagina, difficulty breathing, urinary incontinence, loss of consciousness after childbirth, depression within 42 days of birth, intense lower abdomen pain, and high-grade fever are the main danger signs during the postpartum period.10–14
Obstetric complications and mortality remain a significant burden in low- and middle-income nations. According to estimates, 10.7 million mothers worldwide died between 1990 and 2015 due to obstetric danger signs or complications. 15 About 99% of these deaths took place in developing nations, and in 2020, sub-Saharan Africa accounted for 70% of all maternal deaths globally.16–18 Sub-Saharan Africa had 545 maternal deaths per 100,000 live births in 2020, compared with four in Australia and New Zealand. 18 Almost 800 women die worldwide every day from complications during pregnancy and childbirth, which is one every 2 min,18–20 and 130,000 maternal deaths occurred in 2017 due to obstetric complications or danger signs. 16 According to a recent study, postpartum hemorrhage (27%), hypertensive disorders (14%), and sepsis (11%) account for half of all maternal deaths worldwide.3,21
Many risk factors influence women’s awareness of obstetric danger signs and symptoms, which causes delays in seeking urgent medical treatment. Several studies indicate that socioeconomic and cultural factors,22–24 having a working radio or other informational media, distance from the facility and women’s autonomy, 25 ignorance of obstetric danger signs,14,26–28 lack of knowledge about the availability of emergency obstetric care (EmOC),29–32 attendance at antenatal care (ANC), 33 women informed of risk/complication during ANC,34,35 educational level,6,36 living in a rural area, 37 occupation, 33 and place of deliveries12,38 were factors that cause a delay in seeking timely obstetric care.
Previous studies in developing countries have revealed that women’s awareness of obstetric danger signs affects how they seek health care. A study found that 39 women who lack a basic understanding of pregnancy complications are less likely to seek healthcare attention while experiencing pregnancy danger signs. Similarly, another study 40 showed that women who were unable to recognize danger signs during pregnancy faced delays in receiving medical care due to their inability to recognize danger signs. Also, several studies have shown that women who lack a basic understanding of obstetric danger signs are less likely to be better prepared for birth and more prepared for complications, and as a result, they frequently delay receiving necessary medical care.14,41–44
Since 1990, there has been a discernible decline in the maternal mortality ratio (MMR) worldwide, mostly due to the provision of effective and high-quality EmOC.34,45 Basic EmOC (BEmOC) and comprehensive EmOC (CEmOC) facilities are components included in these EmOC services. 46 BEmOC provides six essential labor and delivery services, called “signal functions,” which include provision of parenteral antibiotics, parenteral anticonvulsants, and parenteral uterotonics; removal of retained products; manual removal of the placenta; and aided vaginal delivery. In addition to performing the six signal duties of a BEmOC facility, a CEmOC facility offers blood transfusions and caesarean sections. 47
Nevertheless, research in underdeveloped countries has found that women with obstetric complications do not use EmOC to its full potential. Only 28% of women who experienced obstetric complications acquired EmOC, according to a study done in nine sub-Saharan African nations. 48 According to a study done in Tanzania, 22% 49 of the country’s women had their EmOC needs addressed, compared with 20.7% 50 and 27% 51 for Malawian and Zambian women, respectively. Thus, there was a significant regional variation in timely use of EmOC and MMRs due to lack of understanding of obstetric complications in developing countries, particularly in sub-Saharan Africa. 52
To achieve this goal, the Sustainable Development Goals (SDGs), set up by the United Nations, aim to lower the global MMR to 70 per 100,000 live births by 2030. 53 This goal cannot be met until the effective provision of high-quality EmOC and a basic understanding of women’s knowledge of obstetric danger signs are improved, particularly in sub-Saharan Africa, where the MMR is now 546 per 100,000 live births.52,54 There is no published systematic review and meta-analysis that shows the associated factors and pooled level of knowledge of obstetric danger signs among women in Africa to generate updated information to decrease maternal death despite the fact that different epidemiological studies were conducted and reported wide variation in the assessment of knowledge of obstetrical danger signs and associated factors among women in African countries.
As a result, the findings may assist the SDG3 in identifying gaps and deciding how to meet the 2030 target of reducing maternal mortality to less than 70 per 100,000 births.55,56 Therefore, this systematic review and meta-analysis will determine the pooled level of knowledge regarding obstetric danger signs and associated factors among women in Africa.
Objectives and questions for review
This investigation aims to:
(1) Determine a cumulative level of understanding regarding obstetric danger signs among African women and
(2) Synthesize data on the contributing factors to this knowledge.
The following review questions provide a framework for this systematic review and meta-analysis:
(1) What is the aggregate level of knowledge among African women regarding obstetric danger signs?
(2) What are the contributing factors to African women’s knowledge of obstetric danger signs?
Methods
Reporting the results of the review
As part of the protocol development process, Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA)-P guidelines were followed. 57 The results will be reported using the PRISMA-2020 standard. 57 In preparation for the submission of this article, a preliminary database search is being conducted as well as a data extraction sheet being developed. The reporting flowchart is presented in Figure 1.

PRISMA flowchart.
Inclusion criteria
Cross-sectional, cohort, and case–control study designs will all be included in this review. Although the search will not be language specific, it will only return results for articles written in English. The knowledge level of obstetric danger signs and associated factors among women will be reported in peer-reviewed and unpublished studies; findings from countries or national surveys and studies conducted in Africa will all be considered in this review. Studies published from inception until April 30, 2023 will be included in the review. To ensure that all papers reporting on women’s knowledge of obstetric danger sign from the start to the present will be considered for the review.
Articles that evaluated women’s knowledge of obstetric danger signs based on the percentage of women who spontaneously mentioned at least two 58 and at least three 59 primary obstetric danger signs will be included. The analysis of both categories (knowledge of at least two and at least three danger signs) will be carried out separately. For each stage, a subgroup analysis will be done on studies that reported on women’s awareness of obstetric danger signs and related factors during pregnancy, labor, and the postpartum period.
Severe vaginal bleeding, hand or face swelling, intense abdominal pain, persistent backache, persistent nausea and vomiting, decreased fetal movements, blurred vision, and convulsions are danger signs during pregnancy.4,60 Severe vaginal bleeding, extended labor (more than 12 h), retained placenta (more than 1 h), premature membrane rupture, fetal malposition, and convulsions are danger signs during labor and delivery.8,14 During the postpartum period, excessive vaginal bleeding following childbirth, foul-smelling discharge from the vagina, difficulty breathing, urinary incontinence, loss of consciousness after childbirth, depression within 42 days of birth, intense lower abdomen pain, and high-grade fever are the main danger signs.6,10,11,61
Exclusion criteria
Studies that do not provide information on the level of knowledge and associated factors, or those for which it is impossible to obtain the necessary information after contacting the authors, will be excluded from investigations into awareness of obstetric danger signs among African women. The following items will also be excluded: articles not published in the English language, conference proceedings, qualitative studies, commentary, editorial letters, case reports, case series, and monthly and annual police reports. Studies that did not meet the quality requirements for this review (danger signs throughout pregnancy, labor, and postpartum) will not be included.
CoCoP and PEO search guide
Outcome/condition: Pooled levels of knowledge
Exposure: All predictors/associated factors of knowledge of obstetric danger signs.
Population: Women
Context/setting: Africa
Search strategy and sources of information
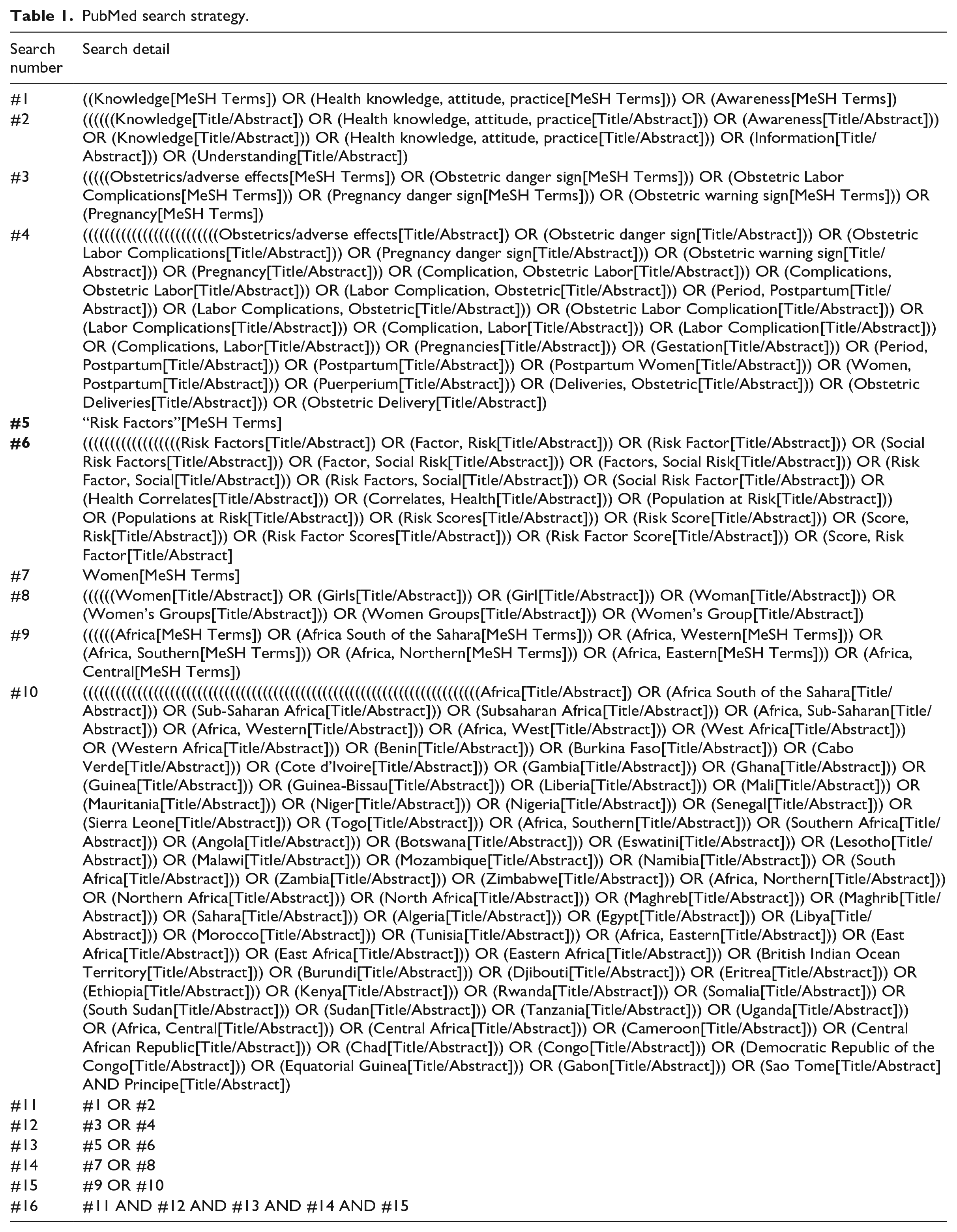
The review used published studies on African women’s knowledge of obstetric danger signs and related factors. In the following electronic databases, studies published from the start until April 30, 2023 are systematically searched and identified: PubMed/MEDLINE, Cumulative Index to Nursing & Allied Health Literature, African Journals Online, and Google Scholar databases. Medical Subject Headings, keywords, and free-text search terms are all employed in PubMed advanced searching (Table 1). Knowledge, Obstetric Danger Signs, Related Factors, Women, and Africa will be utilized as substitute terms and merged using Boolean operators as search phrases.
PubMed search strategy.
We will consult with an experienced librarian to ensure the comprehensiveness of the studies. The references to the publications will be screened using snowballing to find other additional studies that may be relevant. Moreover, experts, researchers, and pertinent organizations will be approached for recommendations on other existing studies. Finally, reference management software (EndnoteTM) imports electronic database search results and eliminates duplicates.
Selection of studies
Based on the inclusion and exclusion criteria, two authors (AHM and TUW) will review the studies to determine which ones to include. The following methods will be used as a guide for the review. The titles of the articles retrieved through the search will first be evaluated. Second, an abstract screening of their eligibility will be done based on predetermined inclusion and exclusion criteria. Lastly, these chosen titles’ abstracts will be incorporated into the final full-text screening round. Using Microsoft ExcelTM, the data charting and screening procedure will be carried out. Only studies approved by both authors will be included in the full article review. Any differences between the authors will be settled by conversation or consultation with a third reviewer (RM and MK). A final list of articles for data extraction will be created after all eliminated studies have given their justifications for exclusion.
Data extraction and management
To collect relevant data, the Joanna Briggs Institute (JBI) data extraction form for experimental/observational studies62,63 will be used. The data will be individually extracted by the two reviewers (AHM and RMI) and exported to an Excel spreadsheet. The initial author’s last name, the year of publication, the nation, region, study design, study period, setting, sampling technique, sample size, method of data collection, spontaneous response or mention of at least two or three obstetric danger signs, proportions of women’s knowledge during pregnancy, child birth and postpartum, and related factors, effect size of risk factors (odds ratio) will all be noted for each included article. Disagreements between data extractors will be handled throughout extraction to reach a consensus. If a consensus cannot be achieved, the authors will consult with a third reviewer (TUW and MKH).
Quality assessment
A critical evaluation of the listed studies will be performed independently by two authors (AHM and TUW). Studies’ qualities will be evaluated using the JBI checklists64,65 for prevalence or proportion studies. The tool has nine parameters: (1) an appropriate sampling frame, (2) an appropriate sampling technique, (3) an adequate sample size, (4) a description of the study subject and setting, (5) adequate data analysis, (6) the use of valid methods for the identified conditions, (7) valid measurement for all participants, (8) the use of appropriate statistical analysis, and (9) an adequate response rate. 66
The tools include options like yes, no, not applicable, and unknown. The score will be one for yes responses and zero for unclear, not applicable, and no answers. In the end, a study that obtains a score of 5 or higher will be considered high quality and added to the final study.65,67 The other two authors (RMI and MKH) will be crucial in resolving any discrepancies between the two raters during the critical evaluation.
Statistical analysis
Data will be presented in graphs and tables based on the findings of the selected study. Due to its adaptation to the Metan program, STATA-14 software packages will be utilized for data entry and analysis. By taking into account the significant variation between study techniques, the random effect model will be used to demonstrate the cumulative knowledge level of obstetric danger signs among women. Because the pooled effect is estimated using the random-effect model, which accounts for between-study variance. 68
To analyze the random effect, the Review Manager V.5.3 software package will be utilized. Measuring heterogeneity will be done using the I2 statistic and a chi-squared test by Cochran’s Q statistic with a 5% significance level. 69 I2 values of 25%, 50%, and 75% are considered indicative of low, moderate, and high heterogeneity, respectively. 70 Sensitivity analysis, subgroup analysis, and meta-regression will all be used to explore heterogeneity sources when I2 is larger than 50%.
The effect size will be used to estimate whether there is a relationship between the related factors and obstetric danger signs. When the p value is less than 0.05, the statistical significance level for effect size is determined.
Publication bias
Egger’s test 71 and funnel plots will be used to analyze the potential risk of publication bias and small study effects. When the p value is statistically significant (p < 0.10), publication bias is declared. The trim-and-fill method suggested by Duval and Tweedie will be applied if publication bias is proven. 72
Ethical considerations
As this study is a protocol for a systematic review and meta-analysis that mainly uses published data and excludes the participation of patients, ethical approval and informed consent are not necessary.
Discussion
This protocol for a systematic review and meta-analysis intends to aggregate data on the prevalence of women’s knowledge of obstetrical danger signs and related factors among African women. Women who are more aware of key obstetric danger signs are more likely to seek emergency care immediately, closely attend ANC, be more prepared for birth, and avoid potential complications. This lowers maternal and infant mortality.12,40,41,73,74
Poor awareness of danger signs causes delays in seeking obstetric treatment, which contributes to high maternal mortality and morbidity globally. 75 According to estimates, obstetric complications or danger signs caused 10.7 million deaths among women globally between 1990 and 2015. 15 Ninety nine percent of these deaths occurred in underdeveloped countries, with 66% of them primarily in sub-Saharan African countries.16,17
Early care-seeking behaviors and prompt access to high-quality EmOC can avoid maternal deaths.46,47 Delays in deciding to seek care, getting to care promptly, and receiving proper care are the three main causes of EmOC access. Lack of awareness and understanding about obstetric danger signs and the consequences of not receiving care among women and the community are the main reasons for these causes.76,77
Findings from this review will therefore provide up-to-date evidence for understanding the pooled prevalence and contributing factors to obstetric danger signs knowledge in Africa. This analysis also indicates the direction in which health policies should be directed to increase women’s awareness of obstetric danger signs in Africa. This will reduce maternal mortality.
As a limitation, heterogeneity is expected in this systematic review and meta-analysis. This is because we will consider various study designs from various geographic regions of the nation. EMBASE and Web of Sciences databases will not be included in the search technique because Ethiopia does not have access to these databases. The search technique can only be used for articles published in English; however, there may be articles published in other languages. Only observational studies are considered in this systematic review; gold-standard randomized clinical trials and quasi-experimental studies are not included.
Conclusion
The burden of obstetric complications and mortality remains a major public health concern in low- and middle-income countries in Africa. According to the World Health Organization, there were 545 women’s deaths per 100,000 live births in sub-Saharan Africa in 2020, compared with four in Australia and New Zealand. Several factors contributed to the development of obstetric danger signs in Africa. These factors included distance from the facility and women’s autonomy. They also included ignorance of obstetric danger signs, inadequate knowledge of emergency maternal care, attendance at ANC, educational level, and place of delivery. Educating women about obstetric danger signs and providing high-quality emergency maternal care should be given primary attention to address the alarming rise in obstetric complications in Africa. As a result, this protocol will provide a pooled level of women’s knowledge of obstetric danger signs and related factors in Africa.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231178102 – Supplemental material for A systematic review and meta-analysis protocol on knowledge of obstetric danger signs and associated factors among women in Africa
Supplemental material, sj-docx-1-smo-10.1177_20503121231178102 for A systematic review and meta-analysis protocol on knowledge of obstetric danger signs and associated factors among women in Africa by Abdulkerim Hassen Moloro, Tejo Ushu Waritu, Mustefa Kasim Haso and Roda Mehadi Ibrahim in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121231178102 – Supplemental material for A systematic review and meta-analysis protocol on knowledge of obstetric danger signs and associated factors among women in Africa
Supplemental material, sj-docx-2-smo-10.1177_20503121231178102 for A systematic review and meta-analysis protocol on knowledge of obstetric danger signs and associated factors among women in Africa by Abdulkerim Hassen Moloro, Tejo Ushu Waritu, Mustefa Kasim Haso and Roda Mehadi Ibrahim in SAGE Open Medicine
Footnotes
Acknowledgements
We thank Samara University for providing free internet and library access.
Authors’ contributions
The study topic was established by Abdulkerim Hassen Moloro and Tejo Ushu Waritu. They also wrote the first draft, developed the search plan, created the data extraction form, and edited and approved the final article.
Mustefa Kasim Haso and Roda Mehadi Ibrahim improved the database search method and data extraction form and edited and approved the final draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.