
Abstract
Background:
Diabetes self-management education supports healthy dietary behaviors but often lacks food skill-building education to plan, budget for, select, and prepare (cook) healthier food.
Objectives:
This study examined the relationship between food skills, diabetes self-management, and stress with medically underinsured patients with type-2 diabetes mellitus within the Fresh Start Food is Medicine (FIM) program. A secondary objective was to examine the impact on diet quality and clinical outcomes.
Methods:
Adults (n = 150) with type-2 diabetes mellitus participated in the 20-week Fresh Start FIM intervention, which included nine group education classes, a produce prescription, and telephone-based health coaching. Group education and skill-building centered around food skills and diabetes self-management. Measures included surveys (e.g., food skills confidence, diet quality, and stress) and clinical measures (e.g., weight, HbA1c, and blood pressure). Data analysis included paired t-tests, Wilcoxon signed-rank tests, and linear regression.
Results:
Significant improvements were observed in food skills confidence (p < 0.001), diet quality (e.g., fruit p = 0.03; vegetable p < 0.001; whole grain p < 0.001 consumption), diabetes self-management (p < 0.001), and perceived stress (p = 0.01). Food skills confidence and diabetes self-management were significant predictors of perceived stress (p = 0.05 and 0.009, respectively). Blood pressure significantly declined (systolic: −6.7 mmHg, p = 0.007; diastolic, p = 0.02).
Conclusion:
Integrating food skills education and individualized behavioral support within an FIM intervention improved food skills confidence, diabetes self-management, and diet quality while reducing perceived stress among medically underinsured patients with type-2 diabetes mellitus. Enhanced self-efficacy in diabetes management and food skills were key contributors to stress reduction, emphasizing the importance of skill-oriented education within diabetes self-management education. These findings underscore the critical role of food skills in building capacity to improve dietary behaviors and health with resource-limited populations.
Introduction
Diabetes affects 38.4 million Americans and accounts for $413 billion in annual healthcare expenditures.1,2 Type-2 diabetes mellitus (T2DM) is the most prevalent form and constitutes 90%–95% of all diagnosed cases in adults. 1 Complications associated with poorly controlled diabetes are costly—both economically and in quality of life—and include blindness, renal failure, stroke, and lower limb amputations.3,4 Prevention of complications requires effective long-term diabetes self-management behaviors, including taking prescribed medications, monitoring blood glucose levels, maintaining a healthy diet, and engaging in regular physical activity.5,6
Diabetes self-management education (DSME) plays a vital role in supporting these behaviors and preventing complications. 7 Despite the established benefits of DSME, these services remain significantly underutilized, for example, a 2022 study from 43 states found that only 52% of individuals with diabetes had ever participated in DSME. 8 Participation was also lowest among Hispanic individuals, the uninsured, residents of rural areas, and those with less than a high school education. 8 These populations are not only less likely to participate in or receive DSME, but they also experience greater barriers to self-management, including poverty, lower educational status, and less access to healthcare.9–12 Additionally, with fewer resources, these groups experience higher levels of psychological stress, which further hinder self-management, self-efficacy, and glycemic control.13,14
The combination of poverty, less education, and access to healthcare also contributes to reduced health literacy, lower food literacy, and food insecurity, making it even more challenging to succeed in self-management and glycemic control.15–17 Low health literacy has been linked to worse glycemic control, higher rates of retinopathy, and diabetes-related complications. 18 Food literacy, a subcomponent of health literacy, includes the nutrition and food knowledge, skills, and self-efficacy to budget, shop, select (e.g., use food labels), and prepare healthy food, with food skills in particular being predictive of diet quality.19,20 Practical food knowledge and skills support individuals to optimize the use of limited food resources to better adhere to a healthy diet needed for glycemic control, overall health, and stress.6,14–23 Furthermore, lowering stress and improving diet are also critical for reducing hypertension, and 50%–80% of individuals with T2DM have elevated blood pressure.24,25
An emerging approach to improve both health and dietary outcomes are Food is Medicine (FIM) programs. Food is Medicine programs provide healthy food to patients to aid in preventing or managing clinical conditions and typically focus on underserved communities. 26 One prevalent FIM model—a produce prescription (PRx) most typically includes a prescription for fresh fruits and vegetables provided by a healthcare provider to be redeemed at a grocery store or farmers market. 25 Produce prescription FIM models have shown promise in improving food security, diet quality, and cardiometabolic health (e.g., HbA1c).27,28 Previous FIM PRx programs typically include some nutrition education (e.g., health benefits of fruits and vegetables, MyPlate), limited behavioral counseling or support, with some offering food-centered education and support (e.g., food literacy education and/or cooking/taste testing).27–29 While food access is critical, dietary and health behaviors are complex. Examination of more comprehensive approaches that integrate multiple strategies to optimize dietary and health behaviors is warranted to address additional barriers to healthy eating and living, such as food and health literacy, skills, and self-efficacy to make behavioral changes. Additionally, few, if any, FIM programs complement dietary changes with exercise as medicine, despite being a “free” treatment with a multitude of established cardiometabolic health benefits and the increased risks associated with a sedentary lifestyle.30–32
Expanding evidence-based behavioral support, counseling, and strategies to address barriers to healthy eating (e.g., low food literacy, taste preferences, and lack of cooking skills), along with clinically focused education such as DSME, and physical activity promotion to optimize cardiometabolic health are warranted. To improve both diet quality and health, FIM programs need to examine approaches to build capacity for sustainable changes around essential health behaviors through improved food skills, health literacy, and physical activity self-efficacy. Moreover, there is growing national interest in identifying optimal education and behavioral support approaches for FIM programs, as evidence-based guidelines are lacking. This need is highlighted by recent funding opportunities from the American Heart Association and The Rockefeller Foundation aimed at addressing gaps within FIM approaches to better promote health and disease management. 33
Therefore, to fill these gaps in research and practice, the Fresh Start (FS) FIM intervention included healthy food access through a PRx, group education, and individualized behavioral support emphasizing DSME and food skills constructs of food literacy (e.g., hands on learning activities—budgeting, planning, food labels/selecting food and cooking demonstrations with taste testing) and physical activity promotion. The primary objective of this study was to investigate the potential impact and relationship between enhanced food knowledge and skills (e.g., literacy), diabetes self-management, and perceived stress in a diverse, rural, medically under-insured/lower income group of patients within this comprehensive FIM model. A secondary objective was to examine the impact of the FS intervention on behavioral (diet quality) and clinical outcomes (i.e., HbA1c, blood pressure, and weight).
Methods
Study design
This 20-week intervention used a single-group, pre–post design, and was implemented from January through May 2023. The FS FIM intervention included nine group culinary and lifestyle medicine classes focused on promoting health/food skills and diabetes self-management, a produce prescription (3–5 lbs./class), and telephone-based health coaching to set individualized goals. Inclusion criteria for the study included being a patient at one of the participating safety net clinics, being an adult (18–64 years of age), lacking health insurance, having a medical diagnosis of pre-diabetes or type-2 diabetes, and being able to provide informed consent. Exclusion criteria included being over 64 years of age, lacking a medical diagnosis of prediabetes or diabetes, having medical insurance, and/or not speaking English or Spanish. We did not include any specific comorbidities as exclusion criteria.
Setting
The study was carried out in partnership with the North Carolina Association of Free and Charitable Clinics network, which consists of over 70 free and charitable clinics across North Carolina. 34 This study took place in rural, eastern North Carolina a region disproportionately affected by socioeconomic challenges including higher poverty, food insecurity, percentage of uninsured adults, and a prevalence of diabetes Table 1.35,36 The four intervention sites in this study included the Hope Clinic in Bayboro (Pamlico County), the Albemarle Hospital Foundation Community Care Clinic in Elizabeth City (Pasquotank County), the WATCH Healthcare Program in Goldsboro (Wayne County), and the MERCI Clinic in New Bern (Craven County).37–40
Income, poverty, uninsured adults, food insecurity, and diabetes prevalence across counties of Eastern North Carolina.

Procedures
Purposive sampling was used to identify eligible patients, who were recruited via healthcare provider referrals, distribution of flyers, and telephone calls to potentially eligible patients. Providers identified eligible patients and referred them to the study team, who then contacted these individuals via phone to discuss the program. The study team also set up informational tables within the clinic’s front lobbies weekly (typically once a week), and clinics also identified eligible patients during routine visits for direct contact (phone calls) to discuss the program. The majority of patients were recruited through direct outreach by the study team rather than through medical provider referrals. Patients (n = 140) were recruited via telephone and scheduled for in-person enrollment appointments, while clinical staff referred an additional 10 patients during usual care. A total sample of 150 patients were enrolled in the FS program from August through December 2022. During enrollment appointments at the clinics, all patients provided written informed consent. The intervention and all materials were approved after a full review by the University and Medical Center Institutional Review Board at East Carolina University (UMCIRB: #21-001619).
Upon obtaining written informed consent, clinical staff measured the patient’s blood pressure, height, weight, and point of care HbA1c. Research team members then orally collected a survey and recorded responses on iPads to ensure consistent data collection with a lower-literacy patient population. To examine the relationship between enhanced food skills, diet quality, diabetes self-management, and stress, several validated questionnaires were integrated into the pre-/postintervention survey. The survey included self-reported sociodemographic information, the Perceived Stress Scale (PSS-10), the Perceived Diabetes Self-Management Scale (PDSMS), an adapted version of the Rapid Eating and Activity Assessment for Participants (REAP-S) for self-reported diet quality, and a validated food skills confidence tool examining several constructs within food literacy.41–44
Group classes lasted 1.5 h and were provided every other week. Classes included (1) diabetes/food-skills focused education, (2) cooking and physical activity demonstrations, (3) taste testing of medically tailored recipes prioritizing nonstarchy vegetables, and (4) distribution of the PRx. The nine group class topics included diabetes self-management, carbohydrates/whole grains, fruit and vegetables, shopping/budgeting, meal planning/prepping, physical activity, weight management, mental health/stress/social support, and heart health. The FS FIM had a program goal for patients to attend at least one group class, with a target of three group classes. A total of nine group classes were provided to support as many opportunities to meet the goal of three and attend class as much as possible due to our experience working with a rural, lower-income patient population with high transportation and schedule barriers. Each lesson was created and led by a registered dietitian nutritionist. Three activities were created for each class and focused on hands-on skill building/application of the lesson materials to best support building health literacy and food skills and patients’ diabetes self-management (e.g., using a supermarket advertisement to create a meal plan for the week and reading a food label). The recipes and culinary approach have been described in a previous article and promote a carb-controlled, nutrient-dense DASH dietary pattern.6,45–48 The DASH diet emphasizes a nutrient-dense dietary pattern high in fiber with double the daily servings of fruits and vegetables compared to general guidelines for health, as well as an emphasis on consuming whole grains, nuts, and seeds.46–48 Produce was donated from local farms and a local food bank. All materials for the study were translated into Spanish by a bilingual member of the research team. This same bilingual research team member and several other bilingual research assistants assisted in interpreting the lessons to the Spanish-speaking patients who attended the classes and provided telephone-based health coaching.
Trained student health coaches provided individualized telephone-based goal setting and support. Goal setting focused on increasing nutrient-dense food (e.g., fruits, vegetables, whole grains) and total minutes of physical activity each week while decreasing high-calorie and heavily processed foods and beverages (i.e., sugar-sweetened beverages, sweets, salty snacks, and fast food). 6 Program goals included a minimum of one initial assessment and follow-up with a target of one assessment and three follow-ups or a total of four contacts due to our previously identified evidence of four encounters being a threshold for behavior change and observed clinical impact. 49 After completion of the program, clinical staff scheduled appointments to collect postintervention blood pressure, weight, and HbA1c. Patients completed a postintervention survey over the phone that included the PSS-10, the PDSMS, an adapted version of the REAP-S, and a validated food skills confidence tool that examines components of food literacy.41–44 Postintervention measures occurred between May 15th and June 30th, 2023. A timeline with further intervention and data collection details can be found in Figure 1.

2023 fresh start (FS) food is medicine (FIM) intervention recruitment, data collection, and implementation timeline.
Measures
To examine the relationship between enhanced food skills, diet quality, diabetes self-management, and stress, several validated tools were utilized.41–44 A validated food skills confidence tool was utilized and prioritized domains 1 and 2 of food literacy as defined by Vidgen and Gallegos, 19 which focused on the “ability to” (1) Plan and Manage, (2) Select, (3) Prepare, and (4) Eat.19,41–44 The food skills section of the tool by Lavelle et al., 44 emphasizes planning and managing food resources—including a construct of “resourcefulness” (e.g., ability to repurpose ingredients or utilize what you have on hand) which are also particularly relevant for the rural patient population with lower income and less access to food resources in this study as resourcefulness, budgeting, planning have been demonstrated to be even more essential food literacy skills for the food insecure. 23 The food skills confidence measure was validated in a study with adults (n = 1049) aged 20–60 years from the United Kingdom and showed strong internal consistency with Cronbach’s alpha values ranging from 0.85 to 0.94 and temporal stability (r = 0.872, p < 0.001). 44 Food skills confidence scores were calculated based on the 19 food skill-specific questions which break into individual food skill constructs of Meal Planning and Preparing (n = 3), Shopping (n = 3), Budgeting (n = 4), Resourcefulness (n = 5), and Label Reading/Consumer Awareness (n = 4). Each of these subsections examined perceived self-efficacy, and all questions were scored from 1 to 7 (1 = very poor, 7 = very good). 44 All 19 questions were then summed to provide a total food skills score (19 questions × 7 = 133 maximum score). 44
Building on the enhancement of food skills, we also evaluated self-reported diet quality with an adapted version of the REAP-S. 43 Questions were adapted to align with the 2020–2025 Dietary Guidelines for Americans recommendations for daily food group consumption and provide further stratify frequency of consumption options. The original tool included three frequency response options: “always,” “sometimes,” “never,” and the adapted tool stratified frequencies to four categories: “rarely/never”, “1–2 times per week,” “3–4 times per week,” and “5–7 times per week.” Additionally, the data collected focused on three categories of food specifically promoted within the program (both education and individual goal setting), which included fruits, vegetables, and whole grains.
Due to the emphasis on improving dietary intake within DSME and overall glycemic control, in addition to diet quality, we included the PDSMS. This validated tool measures a patient’s diabetes self-management and can be used as an outcome measurement for interventions seeking to improve diabetes self-management skills. 42 A previous validation study of the PDSMS among patients with type-1 (n = 57) and type-2 diabetes (n = 341) reported a Cronbach’s alpha of 0.83, indicating internal consistency. 42 The PDSMS consists of eight questions, and responses range from 1 = Strongly Disagree to 5 = Strongly Agree. Four of the questions (#s 1, 2, 6, and 7) are worded so that high agreement would signify lower diabetes self-management; therefore, they are scored in reverse and then added to the score of the other items. 42 The total PDSMS score can range from 8 to 40, where higher scores indicate higher self-efficacy in self-managing one’s diabetes. 42
Lastly, we anticipated that building food skills would correlate with improved dietary intake and perceived capacity to self-manage diabetes, therefore, reducing potential overall perceived stress. We utilized the PSS-10, which has been validated in adult populations and has been shown to be reliable with English and Spanish-language speakers.41,50 The PSS-10 has demonstrated acceptable internal consistency across varying populations with Cronbach’s alpha values of 0.78–0.82.41,50 The PSS-10 assesses the degree to which an individual has perceived life as unpredictable, uncontrollable, and/or overwhelming over the previous month.41,50 Answers are scored from 0 to 4 where 0 = Never, 1 = Almost Never, 2 = Sometimes, 3 = Fairly Often, and 4 = Very Often for questions 1, 2, 3, 6, 9, and 10. Questions 4, 5, 7, and 8 include positive statements and, therefore, are scored in reverse, where 0 = Very Often, 1 = Fairly Often, 2 = Sometimes, 3 = Almost Never, and 4 = Never. 41 The scores for all 10 questions are then summed, and scores range from 0 to 40; higher scores indicate higher levels of perceived stress. The summed scores are then categorized as 0–13 = low stress, 14–26 = moderate stress, and 27–40 = high perceived stress. 41
Statistical analysis
Descriptive statistics (percentages and frequencies for categorical variables; means and standard deviations (SD) for continuous variables) were used to summarize sociodemographic characteristics. Bivariate analyses were performed to compare program completers (patients with full pre- and postintervention data) versus noncompleters (patients with only preintervention data) across sociodemographic and baseline variables. Pearson’s Chi-square test was used for categorical variables (i.e., employment status, food assistance participation, food security status, race/ethnicity, and sex) and independent samples t-tests were used for continuous variables (i.e., age, preintervention blood pressure, diabetes self-management, HbA1c, perceived stress, total food skills confidence, and weight). These comparisons assessed potential baseline differences that might influence the study outcomes.
Paired sample t-tests were also used to evaluate pre- to postintervention changes in perceived stress, diabetes self-management, food skills confidence scores, HbA1c, weight, and blood pressure among program completers. Wilcoxon signed-rank tests were used to examine categorical changes in self-reported diet quality. Multivariate linear regression was used to determine if there was an association between the dependent variable, perceived stress change, and the independent predictor variables’ diabetes self-management change and food skills confidence scores changed after controlling for demographic variables (i.e., age, race/ethnicity, sex). Perceived stress change, diabetes self-management change, and food skills confidence score change were calculated by subtracting postintervention survey scores from preintervention survey scores. A post hoc power analysis for the linear regression indicated that with a sample size of 64, 6 predictors, and an observed effect size (f² = 0.307), the analysis achieved a power of 0.904, suggesting a high likelihood of detecting a true effect if one exists. Missing data were addressed using complete-case analysis, which included only patients with complete data across all variables in the analysis. Only participants who actively participated in the program (⩾1 group class attended, ⩾4 health coach contacts, or a combination of both). All data were analyzed using IBM SPSS 28.0 (SPSS version 28.0, SPS Inc., Armonk, NY, USA). Statistical significance was set at p ⩽ 0.05.
Results
Patient characteristics
Patients (n = 150) were enrolled in the FS intervention and were predominately non-Hispanic (68.7%), female (62.7%), unemployed (50.7%), and African American/Black (36.0%) or White (32.7%), with a mean age of 53 years (SD = 9) Table 2. Less than half of the patients (46.0%) screened as food insecure and received food assistance within the last 12 months (41.4%) preintervention. Patients primarily enrolled in the program to improve their health (98.0%), enhance their blood sugar control (96.7%), for the nutrition information (96.0%), and the cooking information/class (89.4%). Ninety patients (60.0%) attended the group classes at least one time, and attendance is further highlighted in Figure 2. Twenty-three patients (15.3%) didn’t attend any group classes but participated in telephone-based health coaching (⩾4 health coaching phone calls). Fifty-eight patients participated in both the group classes and health coaching. Of the patients who participated in health coaching (n = 81), they completed an average of 4.12 (SD = 5.31) phone calls.
Sociodemographic characteristics from the rural, under-insured, low-income patients with type-2 diabetes from the 2023 fresh start (FS) food is medicine (FIM) intervention (n = 150).

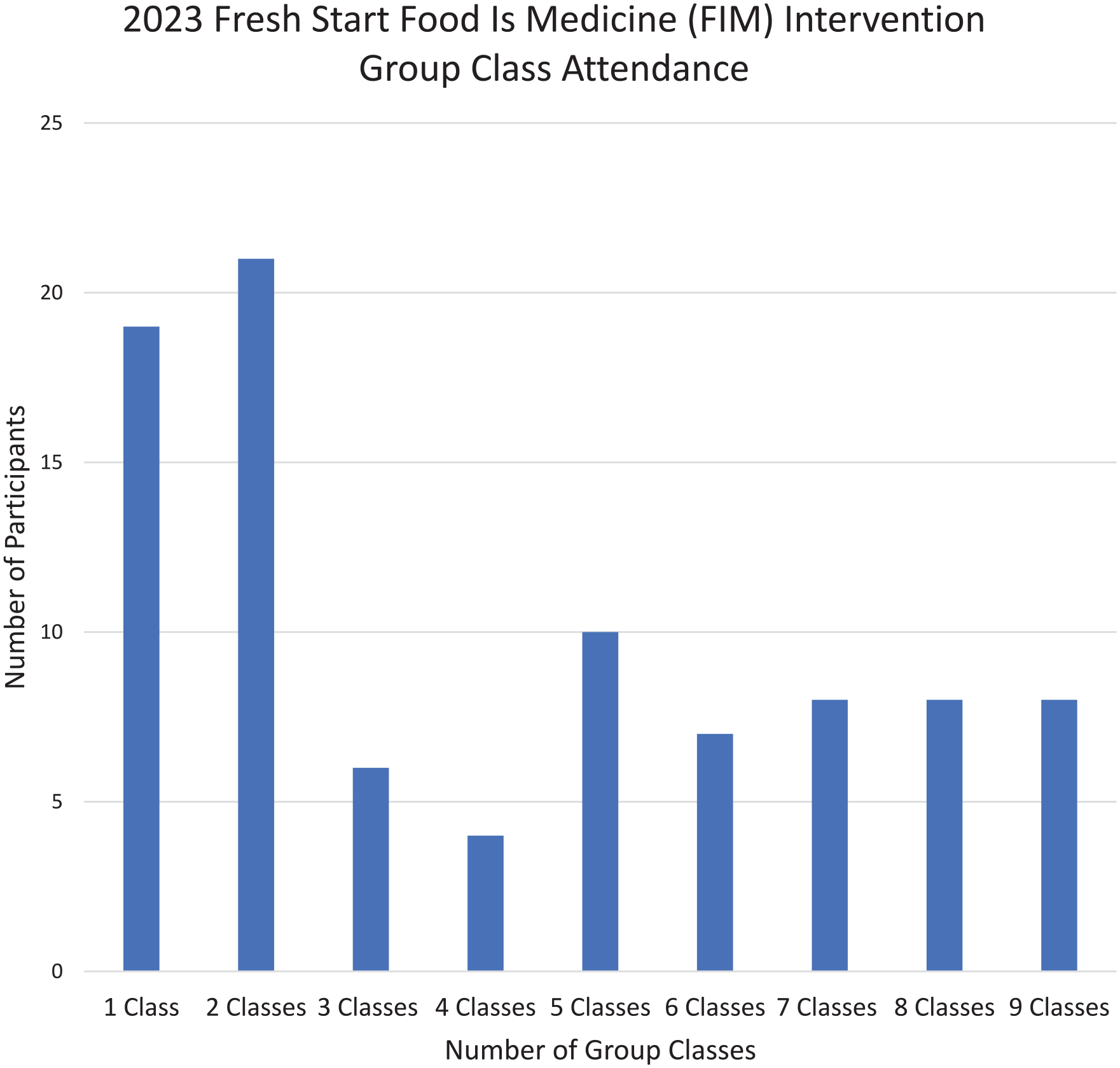
2023 fresh start (FS) food is medicine (FIM) intervention group class attendance (n = 90).
In examining the differences between patients who completed both pre- and postintervention surveys (completers) and those who did not (noncompleters), results indicated a significant difference in preintervention food skills confidence scores. Noncompleters had significantly lower preintervention food skills confidence scores (78.2, SD = 23.6) compared to completers (89.1, SD = 19.5; p = 0.003, t = −2.956). Additionally, Chi-squared tests showed significant differences in sex between groups (χ2(1) = 6.543, p = 0.01), with females being more likely to complete the program than males.
Food skills confidence, diabetes self-management, stress, and clinical outcomes
HbA1c and blood pressure measurements were collected from 82 patients (54.7%), weight were collected from 76 (50.7%) patients, and a full set of pre- and postintervention data were collected from 64 (42.7%) patients. Table 3 summarizes changes in food skills confidence, diabetes self-management, and perceived stress. Total food skills confidence scores increased by an average of 11.8 points, which was statistically significant (p < 0.001, t = −5.64). Diabetes self-management scores increased by an average of 4.2 points, which was also statistically significant (p < 0.001, t = −5.09). Additionally, there was a statistically significant decrease in perceived stress with postintervention scores averaging 2.3 points lower than preintervention scores (p = 0.01, t = 2.66). There were also significant increases in self-reported fruit (p = 0.03, z = 2.21), vegetable (p < 0.001, z = 3.49), and whole-grain consumption (p < 0.001, z = 3.516).
Behavioral outcomes of rural, uninsured, low-income patients with type-2 diabetes from the 2023 fresh start (FS) food is medicine (FIM) intervention (n = 64).

Participants experienced moderate improvements in several clinical outcomes. There was an average decline of 6.7 mmHg in systolic blood pressure and 5.1 mmHg in diastolic blood pressure, and these changes were statistically significant (p = 0.007, t = 2.786; p = 0.02, t = 2.486, respectively). There was also an average decline of 0.19% in HbA1c, and weight loss of 2.76 kg, though neither change was statistically significant (p = 0.24, t = 1.198; p = 0.82, t = 1.761, respectively).
A multiple linear regression was calculated to predict changes in perceived stress based on changes in diabetes self-management and food skills confidence as shown in Table 4. A significant regression equation was found (F(6, 57) = 2.917, p = 0.015), with an R2 = 0.235. The patient’s predicted change in perceived stress is equal to 6.280–0.324 (Change in Diabetes Self-Management)—0.245 (Change in food skills confidence). Perceived stress decreased by 0.324 for each unit increase in diabetes self-management change and by 0.245 unit increase in food skills confidence change. Both changes in diabetes self-management and food skill confidence were significant predictors of changes in perceived stress after controlling for demographic factors (p = 0.009 and 0.05, respectively).
Linear regression results for perceived stress predictors with rural, under-insured low-income patients with type-2 diabetes who participated in the 2023 fresh start (FS) food is medicine (FIM) intervention (n = 64).*
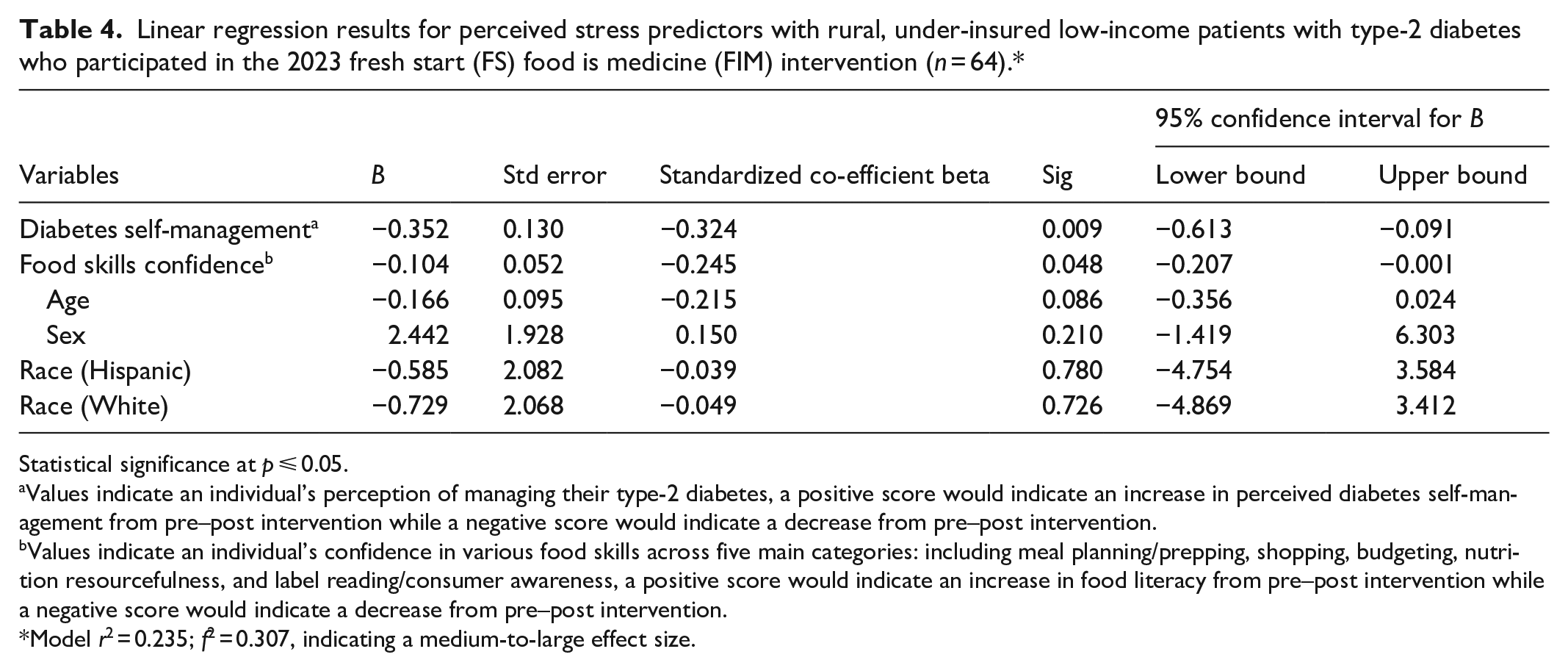
Statistical significance at p ⩽ 0.05.
Values indicate an individual’s perception of managing their type-2 diabetes, a positive score would indicate an increase in perceived diabetes self-management from pre–post intervention while a negative score would indicate a decrease from pre–post intervention.
Values indicate an individual’s confidence in various food skills across five main categories: including meal planning/prepping, shopping, budgeting, nutrition resourcefulness, and label reading/consumer awareness, a positive score would indicate an increase in food literacy from pre–post intervention while a negative score would indicate a decrease from pre–post intervention.
Model r2 = 0.235; f2 = 0.307, indicating a medium-to-large effect size.
Discussion
The primary objective of this study was to investigate the potential relationship between self-efficacy (e.g., diabetes self-management, food skills confidence) and perceived stress in a diverse, rural, medically underserved group of patients with T2DM within a comprehensive FIM model. A secondary objective was to examine the impact of the FS intervention on behavioral (diet quality) and clinical outcomes (HbA1c, blood pressure). Findings from this study fill both gaps in diabetes care and FIM research and demonstrate significant improvements in diabetes self-management, food skills confidence, and reduction in stress within a particularly vulnerable patient group. Diet quality, as well as systolic and diastolic blood pressure, also significan-tly improved, and mean glycemic control saw clinically valuable improvements. These findings will be further expanded upon in the subsequent paragraphs.
The significant reduction in perceived stress is particularly noteworthy, given the well-established link between chronic stress and poor diabetes outcomes, including impaired glucose metabolism, increased insulin resistance, and negative effects on blood pressure, a common comorbidity.24,25,51–53 We theorize the observed reduction in stress predicted by improvements in self-efficacy (i.e., diabetes self-management, and food skills confidence) resulted from the strategic combination of social resources and empowerment—including individualized behavioral support, tailored diabetes/food literacy education, and improved access to healthy food via the provision of a PRx. This comprehensive approach helps to address both the practical burdens of managing T2DM (e.g., taking medications, monitoring blood glucose, planning/preparing healthy meals) and alleviates some of the psychological strain, particularly among populations with lower education and resources.5,8,10,13–15 Given the importance of self-efficacy for the long-term management of diabetes, future FIM interventions should consider incorporating similar education, especially when working with vulnerable populations that are disproportionately burdened by T2DM, food insecurity, stress, and are less likely to access DSME.5,7–9,14,17
Beyond stress reduction, it is notable that the FS FIM model significantly improved patients’ diabetes self-management self-efficacy. This is a critical outcome and cornerstone of effective diabetes management and good glycemic control.5,7,8 The FS intervention effectively integrated DSME within the group education and individualized diet and physical activity support through one-on-one health coaching. This approach goes beyond simply improving access to healthy food and supports the development of knowledge and skills to empower participants to make informed decisions about their health. This is likely even more critical for populations with well-documented barriers to healthcare access and DSME.8–10 While several FIM studies have reported general health improvements, this is the first to the author’s knowledge to integrate DSME alongside a PRx and report improvements in diabetes self-management—not only a positive psychosocial outcome but also a factor that is predictive of overall adherence to diabetes self-management behaviors.54–57
Food skills confidence also significantly increased and predicted a decrease in overall stress. The FS group classes also focused on food literacy, ensuring that participants acquired new knowledge and skills, which they applied to their lifestyle through individualized dietary goals supported by health coaches, which yielded significant improvements in diet quality. Food literacy and culinary educational components are critical to enhancing diet quality. This support extends beyond addressing food insecurity and traditional DSME to overcome additional dietary barriers, such as taste preferences and time constraints, that may hinder the preparation of meals rich in nonstarchy vegetables and snacks high in fiber, which aligns with optimal dietary patterns for glycemic control.6,58,59 Our findings align with previous studies that have associated food knowledge and skills with diet quality, diet quality with glycemic control, and food skills with glycemic control.20,21,60
Furthermore, these findings underscore the critical importance of food skills not only nutrition knowledge as a means of managing T2DM but also as a potential mechanism for stress reduction, especially in populations at higher risk for T2DM disparities (e.g., rural, minority, lower-education, lower-income) who often experience heightened financial and food-related stress.13,20,21,61
In addition to improved self-efficacy and nutrition behaviors, participants also demonstrated clinical improvements. The significant improvements in systolic blood pressure are especially noteworthy, as hypertension is one of the common co-morbidities and further increases the risk of a stroke and other adverse cardiovascular outcomes.24,25 Improvements in diet quality, decreased stress, and weight loss observed (although not statistically significant) may have contributed to the significant declines in blood pressure. A carb-controlled DASH dietary pattern was also emphasized as it is one of the most effective and evidence-based dietary patterns for improved cardiometabolic health.6,46–48 Notably, previous FIM interventions focusing on blood pressure control have not demonstrated the same level of impact on blood pressure outcomes.27–29 However, the comprehensive approach of the FS model, which integrated food literacy education, emphasized the DASH diet, and culinary support (cooking, taste-testing, recipes) enhanced participants’ capacity for dietary change and stress reduction. Although the average weight loss and HbA1c reduction observed in our study were not statistically significant, findings are clinically promising, and these outcomes are consistent with other interventions, which suggest that longer intervention periods may be necessary.62,63
Strengths and limitations
Notable strengths of this study were the demonstration of a unique, timely, and relevant intervention model that combined DSME with a FIM intervention, the impact on a medically underserved socioeconomically disadvantaged, diverse patient population, and the use of validated tools to assess diabetes self-management, food skills confidence, and perceived stress which add to the rigor of the study’s findings.41,42,44 However, this study also has several limitations. First, the absence of a control/comparison group poses a risk to internal validity and makes it challenging to attribute the observed changes solely to the intervention. Without a control group, we cannot establish causality, only an association between food skills, diabetes self-management, and perceived stress. Second, we did not control for medication use or physical activity, which was also promoted in the program, both of which may have confounded the observed clinical changes. Third, an a priori power analysis was not conducted to determine the required sample size. Instead, the sample size was based on the number of participants enrolled per the capacity of the community-based program’s available resources and funding., However, a post-hoc power analysis indicated sufficient power to detect a true effect.
Additionally, we used complete-case analysis, including only participants with full pre- and postintervention data. While sex was controlled for in the analysis, baseline differences between completers and noncompleters in food skills confidence may have introduced attrition bias. Noncompleters had significantly lower preintervention food skills confidence scores, and their exclusion may have led to an overestimation of the intervention’s effectiveness in decreasing stress through food skills confidence improvements. The reliance on self-reported behavioral measures for several key outcomes is another limitation, as these are subject to social desirability bias and may not fully capture actual behavior changes. 64 Lastly, while the FS intervention approach showed promise, the multilayered approach required substantial resources, including administrative support, which may limit the replicability of this study, despite its novel contributions.
Partnership with local/community organizations which already provide some components of this program could be advantageous—for example, cooperative extension agencies lead nutrition education on a local, state, and national levels and may offer strong partners to support integration of food skills/food literacy education, as FIM continues to grow within healthcare, more and more opportunities to connect patients with healthy food through their insurance, and virtual as well as in person options for DSME are available with billing and reimbursement support. While this comprehensive approach was resource-intensive, the vulnerable, rural, medically underserved patient group in our study still demonstrated promising behavioral and clinical outcomes, which suggest the potential value for FIM programs to expand resources to enhance capacity and skills—for example, food skills education in combination with chronic disease self-management education for other vulnerable patient populations (e.g., food insecure, lower-income, medically underserved/Medicaid). Despite these limitations, the study makes a novel contribution to the field of diabetes and chronic disease management by highlighting the potential for comprehensive, tailored FIM interventions to improve both practical and psychosocial outcomes in underserved populations with T2DM.
Conclusion
In summary, findings from this study emphasize the practical need for expanded education that focuses on developing skills in addition to improving healthy food access within FIM, as well as provision of standard DSME especially with vulnerable, medically under-insured patient populations, to build self-efficacy (i.e., food and health literacy) resulting in improved dietary behaviors, clinical outcomes, and reduced stress. While previous studies have explored the individual effects of DSME and food literacy, this study is among the first to demonstrate a direct link between food literacy, diabetes self-management, and perceived stress. Given the links between food insecurity, stress, food skills, diet quality, health literacy, self-management self-efficacy, and cardiometabolic health outcomes, it is time to bolster the intersections between clinical care (e.g., DSME), education/behavioral support (e.g., food skills), and community/social resources (e.g., FIM, PRx). The FS FIM comprehensive model offers a promising approach and results, and future studies may build off of this framework within an experimental design to further examine and identify the most efficacious approaches to guide future clinical practice and research. Future research should also continue to investigate the potential relationship between social and clinical risk factors and explore and evaluate comprehensive, potentially synergistic intervention approaches. Lastly, future studies may also examine long-term potential for sustained lifestyle changes with more skill- and resource focused education versus knowledge-centered in building stronger maintenance postintervention, as well as the potential for less-intensive strategies to support maintenance of behavior changes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251346020 – Supplemental material for Enhancing diabetes self-management and reducing stress through food skills education with medically under-insured individuals with type-2 diabetes
Supplemental material, sj-docx-1-smo-10.1177_20503121251346020 for Enhancing diabetes self-management and reducing stress through food skills education with medically under-insured individuals with type-2 diabetes by Hannah-Therese Rayala, Brandon J Stroud and Lauren R Sastre in SAGE Open Medicine
Footnotes
Acknowledgements
We would also like to thank the Food Bank of Central and Eastern North Carolina and all farmers who contributed produce for the produce prescription. We would like to thank all the clinical staff who assisted with clinical data collection, as well as our paid research assistants and student volunteers who assisted with program implementation and data collection. Lastly, we would like to thank the patients who enrolled in the 2023 Fresh Start program.
Ethical considerations
This study and all materials were approved after a full ethical review from the East Carolina University and Medical Center Institutional Review Board (UMCIRB: #21-001619) on 12/07/2021.
Consent to participate
Written informed consent was obtained from all research participants before enrollment in the program and/or collection of any data. Written informed consent was obtained from all subjects before the study.
Author contributions
The authors confirm contributions to the article as follows: Study Conceptualization: BJS and LRS; Data Curation: BJS and LRS; Formal Analysis: BJS and H-TR; Funding Acquisition: LRS; Investigation: BJS, LRS, and H-TR; Methodology: BJS and LRS; Project Administration: BJS and LRS; Supervision: BJS and LRS; Writing Original Draft: H-TR, BJS, and LRS; Writing Review and Editing: H-TR, BJS, and LRS. All authors reviewed the results and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) would like to report that this project was funded by the Duke Endowment. Additional funding were provided by the Department of Nutrition Science at East Carolina University to cover some program-related costs.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are not publicly available due to containing information that could compromise the privacy of research participants but are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.