
Abstract
Objective:
This study aimed to identify which components of the event-related potentials N170, vertex positive potential, late positive potential, and P3 were most significantly associated with depression in temporal lobe epilepsy.
Methods:
Patients with temporal lobe epilepsy were divided into two groups based on the presence or absence of comorbid depression as diagnosed by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition: those with depression (epilepsy patients with depression group) and those without depression (epilepsy patients without depression group). Both groups were matched for age, education, and seizure-related parameters. A control group of volunteers without epilepsy and depression was also included. Participants underwent electroencephalographic recordings while performing the Oddball task, and the emotional conflict Stroop face-word task. The electroencephalographic data were analyzed using the EEGLAB software.
Results:
The study included 20 patients in the epilepsy patients with depression group and 16 in the epilepsy without depression group, matched for age, gender, and seizure-related parameters. In the epilepsy patients with depression group, the N170 peak amplitude and latency, the vertex positive potential peak latency, and the area under the late positive potential waveform were significantly greater, while the P3 peak latency was shorter compared to the epilepsy without depression group. The areas under the curve for N170, vertex positive potential, late positive potential, and P3 were 0.755, 0.692, 0.645, and 0.731, respectively. Notably, when these four event-related potential components were combined, the areas under the curve increased to 0.922, with a sensitivity of 0.950 and specificity of 0.812 for assessing depression based on the 17-item Hamilton Depression Rating Scale score.
Conclusion:
Specific features of N170, vertex positive potential, late positive potential, and P3 components were significantly associated with depression in patients with temporal lobe epilepsy. These findings suggest that event-related potential components may provide an objective and quantitative approach to enhance the assessment and treatment of depression in epilepsy.
Introduction
The comorbidity of epilepsy and depression is a frequent clinical challenge. According to a meta-analysis by Fiest et al., 1 an overall prevalence of active depression (current or past year) in patients with epilepsy was 23.1% (95% CI: 20.6%–28.31%). Comorbid depressive symptoms significantly impair the quality of life, exacerbate the severity of seizures, and increase the incidence of injuries and accidents.2,3
Epilepsy and depression share common neural circuits and pathogenic mechanisms, suggesting a bidirectional relationship. 4 Notably, 65% of newly diagnosed epilepsy patients exhibit depressive symptoms, pointing to early shared neural damage of epilepsy and comorbid depression during epileptogenesis.5,6 These shared pathways, particularly within the affective network (AN) and cognitive control networks (CCN), may destabilize emotional regulation, contributing to comorbid depression in epilepsy, 7 especially the “cognitive” phenotype depressive symptoms in patients with epilepsy. 8
Despite the use of scales like the Patient Health Questionnaire 99,10 and the 17-item Hamilton Depression Rating Scale (HAMD-17) 11 for assessing depressive symptoms clinically, objective biomarkers that reflect network dysfunction in epilepsy-related depression are still lacking. As important objective biomarkers, electroencephalography (EEG) and event-related potential (ERP) have emerged as promising tools in guiding diagnosis, prognosis, and personalized treatment approaches in patients with major depressive disorders (MDDs). 12 Key EEG features, including activations in alpha and beta bands, EEG alpha asymmetry, EEG coherence, as well as ERP components like P3, have shown potential in predicting treatment outcomes and understanding MDD pathophysiology. 13
The N170, vertex positive potential (VPP), late positive potential (LPP), and P3 are classical ERP components which measure attention and emotion regulation 14 may reflect the functional status of the AN and CNN, offering potential electrophysiological biomarkers for depression in epilepsy. N170 is a negative deflection around 170 ms post-stimulus originated in the occipitotemporal cortex, primarily linked to the perception of faces and facial features. VPP is considered the positive counterpart of N170. Previous studies indicate that N170 and VPP are associated with enhanced neuronal activity in face-sensitive regions and are involved in facial emotion recognition, modulated by attentional, and perceptual demands. LPP is a positive deflection occurring 300–600 ms poststimulus, which reflects the engagement of emotional and motivational systems and is linked to the activation of prefrontal and parietal areas, indicating emotional intensity processing and extended cognitive evaluation.15,16 The P3 component is a widely studied component occurring around 300 ms poststimulus, which is associated with activity in the parietal cortex and medial temporal lobe, linked to cognitive processing such as attentional allocation and activation of immediate memory. 17
The previous study indicated that decreased amplitude and prolonged latency of the N170 and VPP components were observed in patients with bidirectional affective disorder and depression. 15 And the P3 component was verified to have a longer latency period in depressed patients compared to the healthy control (HC). 18
This study aims to determine which ERP components N170, VPP, LPP, and P3 are most significantly associated with depression in patients with temporal lobe epilepsy (TLE). By providing a more objective and quantitative approach to assessing depression, the findings may improve clinical evaluation and management strategies for depression in epilepsy.
Methods
This is a case–control study. We recruited patients with epilepsy in the clinics of Zhongshan Hospital Fudan University, Shanghai, China, from January 1, 2021 to February 3, 2023. All procedures involving the patients complied with the ethical standards of our institutional and national research committees and with the 1964 Declaration of Helsinki and its later amendments. All the included patients signed the informed consent statement.
Subjects
Patients included in this study met the following inclusion criteria: (1) aged between 18 and 65 years, with no gender restrictions; (2) met the diagnostic criteria for TLE as defined by the International League Against Epilepsy in 2014 and 2017,19,20 who had at least two unprovoked (or reflex) seizures occurring >24 h apart or one unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures, occurring over the next 10 years, with the typical clinical manifestations, epileptiform discharges originating in the temporal lobe by video EEG monitoring, presence or absence of structural lesions on cranial magnetic resonance imaging (MRI); (3) seizure-free for at least 72 h; and (4) with no severe cognitive or psychiatric impairments and is able to cooperate in completing the neuropsychological scale assessment and understand and cooperate in completing the paradigms of ERP. Patients were excluded if they had severe medical conditions, malignant tumors, severe cognitive impairment, or mental disorders, had used psychotropic substances and antidepressant drugs in the 2 weeks before the EEG recording, or were unable to cooperate with EEG monitoring task. HC subjects without epilepsy, depression, or other medical conditions were also enrolled. All participants provided informed consent, and the study was approved by the Ethics Committee of Zhongshan Hospital Fudan University, Shanghai, China (Ethics Approved Number: B2020-361, date of approval: December 15, 2020).
Groups based on neuropsychological assessments
All patients with TLE were assessed using neuropsychological scales, including the HAMD-17 and the Mini-Mental State Exam (MMSE).21 –23 The HAMD-17 was employed to assess the severity of depression, while the MMSE was used to evaluate cognitive function and to exclude patients with significant cognitive impairment.
The sample size of the participants was calculated using PASS 15.0 developed by the Number Cruncher Statistical Systems (NCSS LLC, power = 0.90339, alpha = 0.05), determining that approximately 20 participants were needed in each group. Patients with a HAMD-17 score of 7 or more and a diagnosis of depression according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) 24 were enrolled in the epilepsy patients with depression (EPD) group (TLE patients with comorbidity of depression). Age- and gender-matched TLE patients without depression were enrolled in the epilepsy patients without depression (EPN) group (TLE patients without comorbidity of depression). HC volunteers scoring <7 on the HAMD-17 and >28 on the MMSE were also enrolled.
Experimental paradigms
All paradigms in this study were designed and presented using E-prime 2.0 (Psychology Software Tools Inc., Pittsburgh, PA, USA).
Oddball task
The oddball task involved presenting stimuli of different shape, with the target stimulus being a large cross and the standard stimulus being a circle. The stimuli were displayed on or by the computer in a pseudo-randomized order to minimize learning effects, with an interstimulus interval of 1000–1500 ms. Each block comprised 30 standard and 10 odd pictures, each task consisted of 3 blocks, and each of which lasted for 2 min. Participants were instructed to press a button as soon as the odd stimulus appeared.
Emotional conflict Stroop face-word task
The emotional face images were selected from the Chinese Facial Expression Image System revised by Gong et al. 25 A total of 120 facial expression images, including 40 positive emotional faces (20 males and 20 females), 40 negative emotional faces (20 males and 20 females), and 40 neutral emotional faces (20 males and 20 females) were selected in the paradigm. Two typical emotional words, “sad” and “happy,” were selected as vocabulary materials, displayed in red type at the center of the image to create conditions of emotional conflict through word-face consistency and inconsistency. The stimuli were divided into 4 blocks, and each block consisted of 100 trials. Each trial presented 1 face picture, and each block presented a total of 40 positive emotional faces, 40 negative emotional faces, and 20 neutral emotional faces. The face pictures were presented in a random order, and the emotional words “sad” or “happy” were randomly presented in the center of the face pictures. A small black cross was presented in the center of the screen for 500 ms, during which participants were instructed to fixate on the dot. After the fixation point disappeared, the emotional face-word stimuli were presented in the center of the screen for 1000 ms, and participants were required to respond to the image within 500 ms by pressing the “F” or “J” key. This sequence was repeated throughout the task (Supplemental material Figure S1).
EEG recordings, postanalysis, and statistics
A 32-channel EEG cap was placed on each participant’s head according to the revised international 10-20 system. The impedance of each electrode was less than 5 kΩ. EEG signals were continuously recorded using a Nihon Kohden digital amplifier system, with a sampling rate of 500 Hz, a bandpass filter range of 0.1–70 Hz, the fronto-central electrode as the ground, and Cz as the reference electrode. The Oddball task and emotional conflict Stroop face-word task were performed during the process of EEG monitoring.
Artifacts on the raw EEG data, including eye movement artifacts, muscle artifacts, heart artifacts, line noise, and channel noise, were removed by independent component analysis using the EEGLAB toolbox (http://www.sccn.ucsd.edu/eeglab/), with a maximum iteration setting of 2000. The baseline interval was defined as the 1000 ms period before stimulus onset, lasting for 500 ms. The 1000 ms period following stimulus presentation was considered the test interval. Event-related spectral perturbations (ERSPs) were calculated using the EEGLAB newtimef function to detect event-related changes in spectral power. 26
All results were tested for normality, and there were no missing data or data interpolation in this study. Data conforming to a normal distribution were expressed as mean ± standard deviation (SD), while nonnormally distributed parameters were reported as quartiles. The variance test or Wilcoxon rank-sum test was used to compare ERP amplitude, peak latency, and area under the curve between groups. The Pearson’s correlation coefficient was employed to analyze the relationship between HAMD-17 scores and ERP results. Receiver operating characteristic (ROC) curves were plotted to assess the sensitivity and specificity of ERP components in detecting comorbid depression in epilepsy. Statistical significance was set at p < 0.05.
Results
Comparisons of demographic and clinical characteristics in patients with TLE comorbid with and without depression (EPD and EPN groups)
This study included 36 patients with TLE, comprising 20 patients in the EPD group and 16 in the EPN group. Furthermore, 20 gender-matched HCs (male:female = 6:14) without epilepsy or depression, as verified by the MINI-International Neuropsychiatric Interview, 27 were recruited, with an average age of 23.7 ± 2.3 years and an educational duration of 15.8 ± 1.6 years. As shown in Table 1, there were no statistically significant differences between the EPD and EPN groups regarding age, gender, age of onset, disease duration, anti-seizure medication (ASM) regimens, or seizure frequency. Additionally, no significant differences were observed in the MMSE scores between the two groups.
Comparisons of the demographic and clinical characteristics between the EPD and EPN groups.
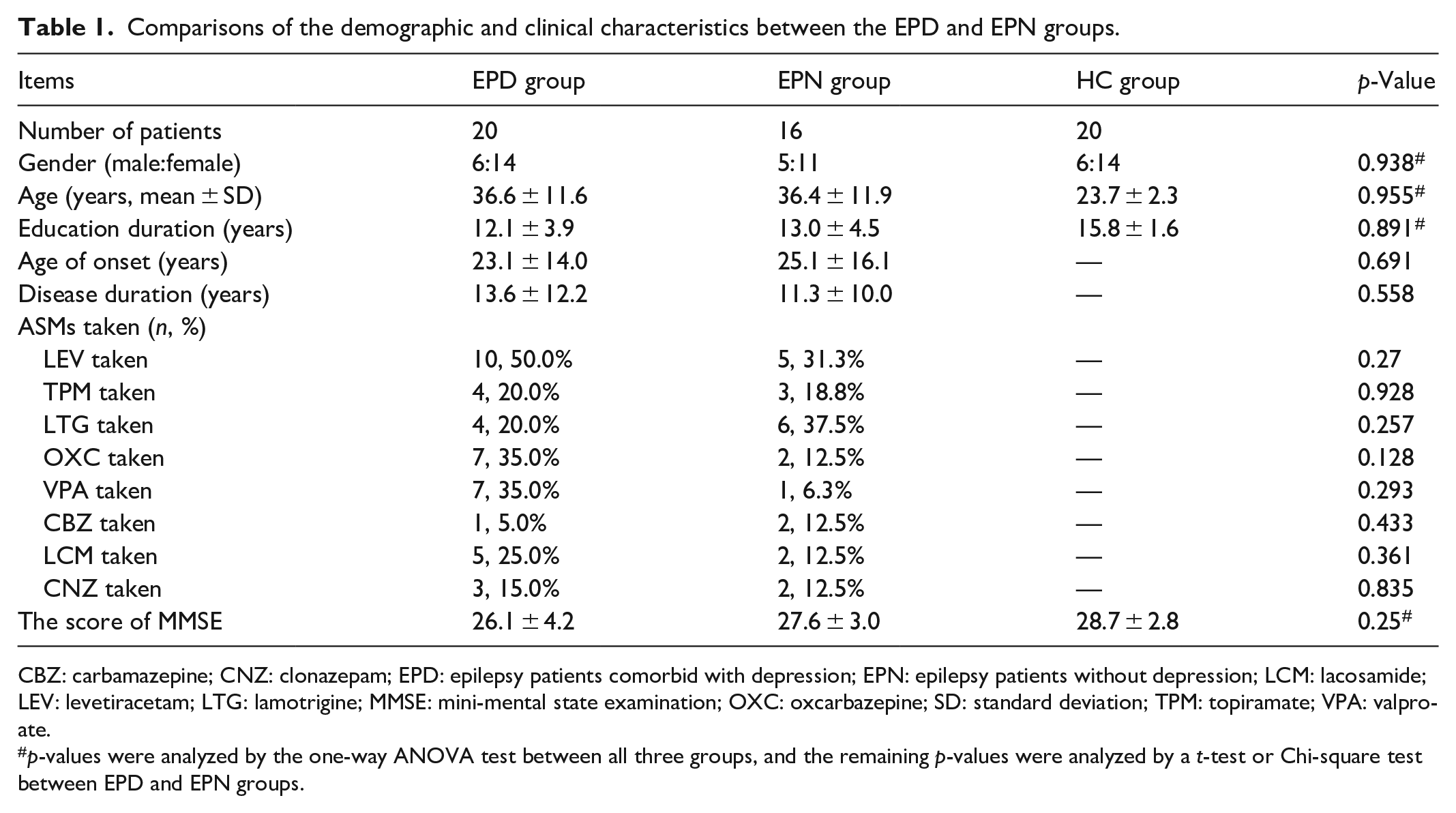
CBZ: carbamazepine; CNZ: clonazepam; EPD: epilepsy patients comorbid with depression; EPN: epilepsy patients without depression; LCM: lacosamide; LEV: levetiracetam; LTG: lamotrigine; MMSE: mini-mental state examination; OXC: oxcarbazepine; SD: standard deviation; TPM: topiramate; VPA: valproate.
p-values were analyzed by the one-way ANOVA test between all three groups, and the remaining p-values were analyzed by a t-test or Chi-square test between EPD and EPN groups.
Electrophysiological characteristics in time domain
The latency of P3 was significantly shorter in the EPD group compared to the EPN group
All study participants were right-handed with normal or corrected-to-normal vision. In the Oddball paradigm, the P3 component was successfully elicited, characterized by a positive potential occurring within the 250–350 ms time window. As shown in Figure 1, patients in the EPD group exhibited a significantly shorter P3 latency compared to those in the EPN group (p = 0.038). No significant differences were found in the peak amplitude, peak latency, or area under the P3 waveform among the EPD, EPN, and HC groups (see Supplemental Material Table S1).

The ERP of the Oddball task in the time domain. The waveform on the left represents the ERP elicited by the target stimuli of the Oddball task, while the waveform on the right represents the ERP elicited by the standard stimuli. The blue color represents the EPD group, the red color represents the EPN group, and the gray color represents the HC group. The right part shows the group comparison of the peak latency of the P3 component between the EPD and EPN groups, with the EPD group showing a significantly shorter latency than the EPN group (*p < 0.05).
The amplitude and latency of N170, the latency of VPP, and the area under the waveform of LPP were significantly greater in the EPD group compared to the EPN group
In the emotional Stroop word-face paradigm, the N170 and VPP components were successfully elicited. The N170 appeared as a negative potential at the P7 scalp electrode within the 100–200 ms time window, while the VPP appeared as a positive potential at the CP4 scalp electrode. Additionally, a distinct LPP component emerged after 600 ms as a positive potential at the O2 scalp electrode (as shown in Figure 2(a)).

(a) Comparison of the ERPs between the EPD group (red), the EPN group (blue) and the HC group (black), elicited by the emotional Stroop word-face task, showed that the peak amplitudes of the N170 and VPP were both higher in the EPD and EPN groups than those in the HC group, respectively (p < 0.05); (b) there was a significant negative correlation between the peak amplitude of the N170 component and the HAMD-17 score (r = −0.452, p = 0.006).
The peak amplitudes of the N170 and VPP components elicited by the emotional Stroop word-face task were significantly higher in both the EPD and EPN groups compared to the HC group (p < 0.05, see Figure 2(a)). Notably, the negative amplitude of the N170 component in epilepsy patients was correlated with the HAMD-17 score (r = −0.452, p = 0.006, see Figure 2(b)), suggesting a close relationship between N170 amplitude and the severity of depression in epilepsy patients. However, no significant correlation was found between the N170 component and other scales, such as the MMSE.
The N170 amplitude was significantly larger across conditions 1–3, especially in condition 3, and its peak latency in conditions 2 was significantly longer in the EPD group compared to the EPN group. The peak latency of the VPP in condition 3 was also longer, and the area under the LPP waveform in conditions 1–3 was significantly larger in the EPD group than in the EPN group (see Table 2 and Figure 3).
Comparisons of the peak amplitude, peak latency, and area under the curve of N170, VPP, and LPP between the EPD and EPN groups.

EPD: epilepsy patients comorbid with depression; EPN: epilepsy patients without depression.

The four columns from left to right represent the ERP waveforms elicited by conditions 1–4 of the emotional Stroop word-face task (condition 1: positive emotional faces with negative words; condition 2: negative emotional faces with positive words; condition 3: neutral faces with positive words; condition 4: neutral faces with negative words).
Time–frequency domain of the emotional conflict task
Time–frequency power maps for the four conditions of the emotional conflict tasks were compared between the HC, EPD, and EPN groups. The results showed that HC group exhibited significantly greater event-related synchronization (ERS) in the alpha and beta band during the 100–200 ms time window, an effect absent in the epilepsy groups. Nevertheless, the EPD group exhibited significantly higher ERS in the theta frequency band during the 200–500 ms time window elicited by condition 4, and significantly lower event-related desynchronization (ERD) in the beta frequency band during the 300–600 ms time window elicited by condition 2 compared to the EPN group (see Figure 4).

A significant high ERS in the alpha and beta band during the 100–200 ms time window was shown in the HC group, which was absent in the epilepsy groups. A significantly higher ERS in the theta frequency band during the 200–500 ms time window elicited by the condition 4 and a significantly lower ERD in the beta frequency band during the 300–600 ms time window elicited by the condition 2 were found in the EPD group than those in the EPN group (p < 0.05). In the color bar, red represents ERS, and blue represents ERD, with darker colors indicating larger ERSP values. The deep red area in the right column shows frequency bands with a significant difference in ERSP values between the EPD and EPN groups within the time windows.
Sensitivity and specificity of N170, VPP, LPP, and P3 components in assessing depression in TLE patients
A predictive model was constructed using binary logistic regression, incorporating the peak latency of the P3 elicited by the Oddball task, the peak amplitude of the N170, the peak latency of the VPP, and the area under the LPP waveform elicited by condition 3 of the emotional Stroop face-word task as individual or composite electrophysiological markers. ROC curves were plotted to evaluate the diagnostic value of this model. As shown in Figure 5, the AUC values for N170, VPP, LPP, and P3 were 0.755, 0.692, 0.645, and 0.731, respectively. The composite marker combining all four ERP components achieved the highest AUC value of 0.922, significantly surpassing the performance of the individual components. This predictive model demonstrated high diagnostic value, with a sensitivity of 0.950, specificity of 0.812, and a Youden’s index of 0.762 at the optimal cut-off point.

The predictive model used the HAMD-17 score as the gold standard and adopted the peak latency of P3, the peak amplitude of N170, the peak latency of VPP, and the area under the waveform of LPP as a composite electrophysiological marker. The ROC curve showed that the composite electrophysiological marker had the highest area under the curve (AUC = 0.922), which was significantly higher than the individual components.
Discussion
Although the DSM-V is a diagnostic gold standard for depression, it relies heavily on subjective self-reports and clinical interviews, making it prone to interpretation bias, recall issues, and cultural influences. Stigma and limited receptivity among TLE patients may further reduce the efficacy of psychological interviews. In this study, we investigated ERP as an electrophysiological biomarker to evaluate depressive comorbidity in this population.
Our findings indicated that the N170, VPP, LPP, and P3 components were reliably elicited, with significant differences in amplitude and latency between groups, reflecting distinct neural responses associated with emotional conflict and depressive symptoms. Combining the peak latency of P3, the peak amplitude of N170, the peak latency of VPP, and the area under the LPP waveform achieved a sensitivity of 0.950 and a specificity of 0.812 in detecting depression in TLE patients, highlighting the utility of combinatorial ERP measures as potential biomarkers for assessing depression in epilepsy.
Different psychological paradigms elicit distinct ERP components, each offering unique insights into cognitive and emotional processes. For example, the Oddball paradigm reliably produces a robust P3 component, 14 which has been extensively employed in research to investigate attention and working memory. In contrast, the emotional conflict Stroop face-word paradigm predominantly triggers N170, VPP, and LPP components, revealing critical aspects of emotional cognition. 28 Recognizing the complementary strengths of these paradigms, we have integrated both into our study to achieve a more holistic perspective on the neural mechanisms underlying emotional processing.
The amplitude and latency of ERPs elicited by emotional Stroop tasks are sensitive indicators of the brain's processing speed and attentional biases. 14 The increased amplitudes of the N170 and VPP components in both the EPD and EPN groups, compared to the HC group, suggest heightened neural sensitivity to emotional stimuli among patients with epilepsy. Notably, the negative amplitude of N170 had a correlation with HAMD-17 scores highlights a potential link between neural processing of facial stimuli and the severity of depressive symptoms in epilepsy. As shown by Jacques et al. 29 in an intracranial EEG study, the N170 component may be generated in the right fusiform gyrus, a brain area primarily involved in face recognition. Our findings suggest that TLE patients with epileptogenic foci in the temporal lobe exhibit enhanced neural responses to faces, particularly in those with comorbid depression. This finding aligns with previous studies suggesting that early visual processing, as indexed by N170, is modulated by emotional states, particularly depression. However, the absence of significant correlations between N170 and other cognitive scales, such as the MMSE, underscores the specificity of this component to emotional, rather than cognitive, dysfunction.
The VPP, considered the vertex counterpart of the occipitotemporal N170 component, 30 showed significantly longer peak latencies in condition 3 along with the greater peak latency of the N170 in conditions 2 and 4 within the EPD group than the EPN group, may reflect delayed neural processing of emotional stimuli, which is consistent with altered cognitive control mechanisms in depression. These latency differences suggest that the neural pathways involved in rapid emotional processing are disrupted in patients with comorbid epilepsy and depression. Previous studies using scalp EEG 31 and fMRI 32 have localized the sources of N170 and VPP to the anterior cingulate gyrus, temporal, and parietal lobes, with involvement of the anterior cingulate gyrus in emotional conflict processing. These findings align with our prior work showing abnormal functional connectivity in the anterior cingulate gyrus among patients with both epilepsy and depression. 33
The LPP is typically larger during the presentation of emotional stimuli compared to neutral stimuli. 34 Previous research has indicated that the emotional effects of LPP are independent of stimulus size and perceptual characteristics, 35 and the LPP can persist for seconds during emotional picture presentations. 36 The enlarged area under the LPP waveform in the EPD group further supports the idea of prolonged emotional engagement, indicating sustained attention to emotionally salient stimuli. This heightened and prolonged neural response could reflect an increased cognitive load when processing emotional conflict, as often observed in depressive disorders. 37
Interestingly, although previous studies have reported longer P3 latencies in epilepsy patients compared to HCs, 38 our findings revealed shorter P3 latencies in the EPD group compared to the EPN group. Since P3 typically reflects immediate attention allocation, 39 this may suggest temporarily increased attention during stimulus detection in the EPD group.
To sum up, combining multiple paradigms and ERP components offers a more comprehensive and precise understanding of depressive symptoms in epilepsy patients, particularly when seizures affect multiple brain networks. Our findings demonstrate that the integration of N170, VPP, LPP, and P3 components provides a sensitive and accurate reflection of depressive symptoms and their severity, which may enhance diagnostic precision. The generator of P3 might be contributed by glutamatergic neurotransmission in the temporal and parietal cortical areas. 40 As dopamine, norepinephrine, and serotonin were the basis for all emotions, 41 these transmitters in emotional circuits might be involved in producing components of N170, VPP, and LPP elicited by Emotional Stroop tasks in this study. Therefore, this approach reveals the complex neural disruptions underlying epilepsy-related depression.
We also observed distinct patterns of ERS and ERD in the theta and beta bands, respectively, between the EPD and EPN groups via the time–frequency analysis. The enhanced theta ERS in the EPD group during emotional conflict tasks, aligns with Ma et al., 28 who reported increased theta-band power in frontal and frontocentral areas associated with attentional bias toward negative emotions, indicating greater emotional arousal and cognitive effort, a hallmark of depression. Conversely, the reduced beta ERD in the EPD group suggests impaired disengagement from emotional stimuli, potentially reflecting the emotional processing disturbances. 42 These findings emphasize the importance of frequency-specific neural dynamics in distinguishing emotional processing in clinical groups and highlight the need to examine both time and frequency domains to understand emotional conflict processing in epilepsy.
Although previous studies have shown that ASMs induce notable changes in EEG patterns,43,44 ERP and ERSP had virtues of eliminating nontime-locked and nonphase-locked EEG background changes through iterative averaging. Furthermore, no significant differences in types of ASMs usage were found between the EPD and EPN groups, indicating that ASMs-induced EEG alterations might have no statistical differences.
A limitation of this study is the potential presence of other psychiatric comorbidities in the EPD group, although we excluded psychotic symptoms using the Brief Psychiatric Rating Scale. We controlled for group differences in ASMs, age, gender, and MMSE scores between the EPD and EPN groups to minimize confounding effects. Future research should include a larger sample size and consider additional psychiatric assessments to better delineate the impact of comorbidities.
Conclusion
In conclusion, this study shows that TLE patients with comorbid depression have distinct ERP features. Compared to those without depression, they have a higher N170 amplitude, longer VPP latency, larger LPP waveform area, shorter P3 latency, higher theta ERS, and lower beta ERD. The binary logistic regression results indicate that the multicomponent ERP approach could be a valuable clinical assessment tool.
The ERP analysis provides an objective and quantitative approach, thereby augmenting traditional subjective evaluations, enhancing the diagnostic accuracy of depression in patients with epilepsy, and facilitating more timely therapeutic interventions. Moreover, the results of this study contribute to a deeper understanding of the pathophysiological mechanisms underlying the comorbidity of epilepsy and depression.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251335468 – Supplemental material for Event-related potential biomarkers in temporal lobe epilepsy: N170, vertex positive potential, late positive potential, and P3 signatures of depression comorbidity
Supplemental material, sj-docx-1-smo-10.1177_20503121251335468 for Event-related potential biomarkers in temporal lobe epilepsy: N170, vertex positive potential, late positive potential, and P3 signatures of depression comorbidity by Weifeng Peng, Zihan Hu, Jia Liang, Jing Ding and Xin Wang in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121251335468 – Supplemental material for Event-related potential biomarkers in temporal lobe epilepsy: N170, vertex positive potential, late positive potential, and P3 signatures of depression comorbidity
Supplemental material, sj-docx-2-smo-10.1177_20503121251335468 for Event-related potential biomarkers in temporal lobe epilepsy: N170, vertex positive potential, late positive potential, and P3 signatures of depression comorbidity by Weifeng Peng, Zihan Hu, Jia Liang, Jing Ding and Xin Wang in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121251335468 – Supplemental material for Event-related potential biomarkers in temporal lobe epilepsy: N170, vertex positive potential, late positive potential, and P3 signatures of depression comorbidity
Supplemental material, sj-docx-3-smo-10.1177_20503121251335468 for Event-related potential biomarkers in temporal lobe epilepsy: N170, vertex positive potential, late positive potential, and P3 signatures of depression comorbidity by Weifeng Peng, Zihan Hu, Jia Liang, Jing Ding and Xin Wang in SAGE Open Medicine
Supplemental Material
sj-jpg-4-smo-10.1177_20503121251335468 – Supplemental material for Event-related potential biomarkers in temporal lobe epilepsy: N170, vertex positive potential, late positive potential, and P3 signatures of depression comorbidity
Supplemental material, sj-jpg-4-smo-10.1177_20503121251335468 for Event-related potential biomarkers in temporal lobe epilepsy: N170, vertex positive potential, late positive potential, and P3 signatures of depression comorbidity by Weifeng Peng, Zihan Hu, Jia Liang, Jing Ding and Xin Wang in SAGE Open Medicine
Footnotes
Acknowledgements
We thank all the participants involved in this study.
Ethical considerations
Ethical approval for this study was obtained from the Ethics Committee of Zhongshan Hospital Fudan University, Shanghai, China (Ethics Approved Number: B2020-361, date of approval: December 15, 2020). We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Consent to participate
Written informed consent was obtained from all subjects before the study. All procedures involving the patients complied with the ethical standards of our institutional and national research committees and with the 1964 Declaration of Helsinki and its later amendments. All the included patients signed the informed consent statement.
Author contributions
WP designed the study, recruited patients, and rewrote the manuscript. ZH did most of the ERP experiment, collected data, conducted statistical works, and participated in writing the primary manuscript. JL did a portion of the ERP experiment. JD and XW conceptualized, designed, and sponsored the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by Science and Technology Plan Project of Fujian Province (2021GGB033).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during the current study shall be make available by the corresponding author upon reasonable request, subject to regulatory approval.
Trial registration
This randomized clinical trial was not registered because it’s an observational study without interventions and evaluating causal relationships to health outcomes.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.