
Abstract
Background:
Endometriosis involves the presence of endometrial-like tissue outside the uterus, driven by inflammatory pathways including elevated interleukin-32 and vascular endothelial growth factor. One potential anti-inflammatory agent is active vitamin D (1,25(OH)2D3).
Objectives:
This research investigates the correlation among 1,25(OH)2D3 levels, interleukin-32, and vascular endothelial growth factor in confirmed endometriosis cases.
Methods:
This observational analytic correlational study aimed to explore the relationship between these inflammatory factors and vitamin D levels in endometriosis. The study involved 46 participants, with histopathologically confirmed endometriosis cyst tissue collected from patients undergoing laparotomy or laparoscopy at three hospitals: Dr. Hasan Sadikin Hospital Bandung, Cibabat General Hospital Cimahi, and Limijati Maternity and Children’s Hospital. The levels of interleukin-32, vascular endothelial growth factor, and 1,25(OH)2D3 were measured using the enzyme-linked immunosorbent assay method at the Clinical Pathology Laboratory of Dr. Hasan Sadikin Hospital Bandung.
Results:
The study revealed significant negative correlations between 1,25(OH)2D3 and both interleukin-32 (r = −0.346; p = 0.019) and vascular endothelial growth factor levels (r = −0.316; p = 0.032). Conversely, there was a significant positive correlation between vascular endothelial growth factor and interleukin-32 (r = 0.490; p = 0.001).
Conclusions:
These findings underscore the role of active vitamin D in mitigating inflammation associated with endometriosis by reducing interleukin-32 and vascular endothelial growth factor, critical factors in inflammatory responses and blood vessel formation. Moreover, the positive association between vascular endothelial growth factor and interleukin-32 highlights their collaborative role in the inflammatory processes underlying endometriosis. This study contributes to understanding how vitamin D may modulate key inflammatory pathways implicated in the pathogenesis of this condition.
Introduction
Endometriosis is a chronic inflammatory disease characterized by the presence of tissue similar to the endometrium outside the uterus. 1 The age range of patients diagnosed with endometriosis is between 20 and 42 years. The prevalence of endometriosis is estimated to be between 2% and 10% in the female population worldwide, and up to 50% of infertility cases are associated with endometriosis. 2
Potential origins of endometriosis lesions include the transplantation of endometrial tissue through retrograde menstruation and in situ metaplasia of coelomic epithelium. Lesions outside the pelvis may be caused by vascular or lymphatic metastasis. 2 Superficial and deep infiltrating endometriosis lesions form through molecular mechanisms involving interactions between adhesion, cell proliferation, systemic and local steroidogenesis, chronic inflammation, immune dysregulation, vascularization, and innervation. 3
The chronic inflammatory response in endometriosis involves both innate and adaptive immune responses influenced by estrogen hormones. 4 The initial innate immune response involves macrophage phagocytosis mediated by scavenger receptors and regulated by cytokines. Patients with endometriosis exhibit abnormalities in their innate immune response, where macrophages fail to perform phagocytic functions on endometriosis lesions, particularly during the mediation process by scavenger receptors. 5
The adaptive immune system becomes involved when the innate immune response is insufficient to handle the pathological conditions. The adaptive immune system consists primarily of T and B lymphocytes. In patients with endometriosis, there is an increase in cytokine modulation by T cells and the formation of autoantibodies by B cells. 6
Cytokines are proteins produced by various cells including stromal cells, fibroblasts, and endothelial cells. Interleukin-32 (IL-32) is one among proinflammatory cytokines thought to be involved in the pathogenesis of endometriosis. IL-32 has diverse functions such as regulating the body’s immune response during infection, contributing to autoimmune diseases, cancer, and inflammatory reactions. 7
IL-32 is recognized as a proinflammatory cytokines and a potent inducer similar to other proinflammatory cytokines such as TNF-α and IL-8. IL-32 activates specific cytokine signaling pathways including NF-ĸB and p38 mitogen-activated protein kinases. Activation of the NF-ĸB pathway leads to inflammation, invasion of endometriosis cells, angiogenesis, proliferation, and inhibition of apoptosis processes within endometriosis cells. 8 Another cytokine pathway activated by IL-32 is the p38 mitogen-activated protein kinases pathway, which results in increased cytokine production, proliferation of endometriosis cells, and reduced apoptosis processes. 9
Vascular endothelial growth factor (VEGF) is a vasoactive substance involved in various physiological processes in the body, including wound healing and endometrial revascularization. Increased VEGF levels trigger excessive angiogenesis, allowing endometriosis lesions to persist and progress. Activation of VEGF receptors in endothelial cells initiates processes such as endothelial cell proliferation, migration, increased blood vessel permeability, and induction of blood vessel remodeling, ultimately leading to the formation of new blood vessels. 10
Another factor involved in endometriosis pathogenesis is vitamin D deficiency. 6 Vitamin D has anti-inflammatory benefits by reducing cytokine production in the body. The most active metabolite of vitamin D is 1,25(OH)2D3, which has been shown to have significant antiproliferative effects in preclinical models, inhibiting cell differentiation processes, angiogenesis, and inducing apoptosis.11,12
The role of vitamin D in relation to IL-32 is indirect, involving inhibition of NF-ĸB by direct binding to IKKβ, thereby reducing IL-32 levels. 11 Additionally, evidence suggests that vitamin D can affect the normal function of endothelial cells in angiogenesis by suppressing VEGF production through autocrine Wnt/β-catenin pathway inhibition. 13
Methods
Study design
This observational analytic correlational study measures independent and dependent variables simultaneously. The included subjects were patients aged 20 and 42 years diagnosed with endometriosis confirmed by histopathological examination. On the other hand, patients were excluded if they used hormone therapy within the last 3 months (progestin only, combination, leuprolide acetate), patients with ovarian infections, and ovarian malignancies. Sample selection was done using consecutive sampling, where endometriosis patients who visited Dr. Hasan Sadikin General Hospital Bandung, Limijati Mother and Child Hospital, and Cibabat Regional General Hospital from January to May 2024 who met the criteria were included until the minimum sample size was met.
Data collection
Patients who met the criteria were informed about the study and given informed consent. Endometriosis diagnosis was established based on medical history, physical examination, transvaginal ultrasound, operative findings by Obstetrics and Gynecology specialists, and histopathological diagnostic examination by pathology specialists. Endometriosis tissue diagnosed based on histopathological findings were sent to the Clinical Pathology Laboratory of Dr. Hasan Sadikin General Hospital Bandung.
Tissue specimens underwent homogenization, protein extraction, and total protein concentration measurement, with focus on target protein concentrations. The concentrations of target proteins (1,25(OH)2D3, VEGF, and IL-32) extracted were quantified using ELISA method and spectrophotometric techniques, and results were compared with standard curves for normalization to obtain quantitative data.
Statistical methods
Pearson’s based calculation method sampling for correlation test was used in this study. By considering alpha (α) = 0.05, power (1-Beta) = 0.80 (80%), and for Pearson’s coefficient = 0.4. Thus, the calculated sample size was 46. Data collected was analyzed using SPSS version 25. A p-value less than 0.05 is considered statistically significant. Normality of numeric variables was assessed using the Shapiro–Wilk test. The data were not normally distributed; therefore, the correlation between the levels of 1,25(OH)2D3, IL-32, and VEGF levels were analyzed using Spearman’s rank correlation.
Results
A total of 46 patients diagnosed with endometriosis cysts, who underwent surgery either through laparoscopy or laparotomy at Dr. Hasan Sadikin General Hospital and Cibabat Regional Hospital from January to May 2024, were included in the study analysis.
Table 1 shows most endometrial cyst patients were found in the age group of 31–36 years (34.8%). The average age was 30.8 years (SD ± 5.7 years), indicating a wide variation in ages around the average. The average body mass index (BMI) of the patients reached 24.12 ± 4.31 kg/m², showing that most of the BMI levels are classified as normoweight. All study subjects were recorded as nonsmokers (100%). Out of 46 samples in this study, it was found that only about 10.9%, or five patients, did not have infertility issues. The rest of the subjects were diagnosed with infertility. Subsequently, further bivariate analyses were conducted to uncover potential correlations among the various variables encompassed in the study, as delineated below.
Sociodemographic characteristics of 46 patients with endometriosis cysts attending several hospitals in Bandung.

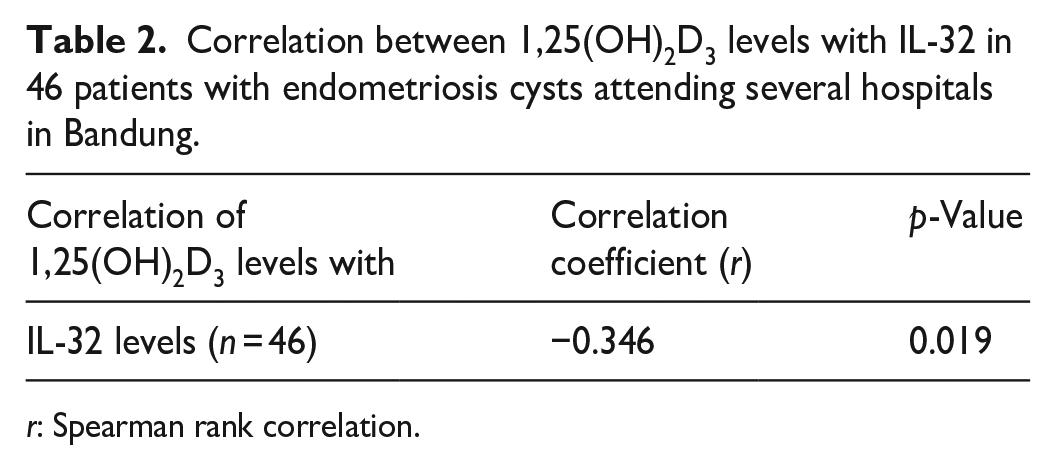
Table 2 and Figure 1 show that the levels of 1,25(OH)2D3 and IL-32 in endometriosis cysts were found to be significantly and negatively correlated in all measurements (p-value < 0.005). The correlation coefficient (r) was −0.346 meaning that an increase in the levels of 1,25(OH)2D3 will be followed by a decrease in the levels of IL-32, and vice versa.
Correlation between 1,25(OH)2D3 levels with IL-32 in 46 patients with endometriosis cysts attending several hospitals in Bandung.
r: Spearman rank correlation.

Correlation between 1,25(OH)2D3 levels with IL-32 in 46 patients with endometriosis cysts attending several hospitals in Bandung.
Meanwhile, the correlation between 1,25(OH)2D3 levels and VEGF in endometriosis cysts is shown in Table 3. The analysis revealed a correlation coefficient (r) of −0.316, indicating a negative correlation between 1,25(OH)2D3 and VEGF levels. This suggests that an increase in 1,25(OH)2D3 levels tends to be followed by a decrease in VEGF levels, and vice versa. The correlation is weak to moderate represented by Figure 2. However, the correlation is found to be statistically significant (p < 0.05).
Correlation between 1,25(OH)2D3 levels with VEGF level in 46 patients with endometriosis cysts attending several hospitals in Bandung.

r: Spearman’s rank correlation.

Correlation between 1,25(OH)2D3 levels with VEGF level in 46 patients with endometriosis cysts attending several hospitals in Bandung.
Further, the correlation between IL-32 levels and VEGF in endometriosis cysts is presented in Table 4. The analysis found a correlation coefficient (r) of 0.490 and a p-value of 0.001. This indicates a positive correlation between IL-32 and VEGF levels. Figure 3 shows that as IL-32 levels increase, VEGF levels also tend to increase, and vice versa. The p-value of 0.001 suggests that this correlation is highly statistically significant.
Correlation between IL-32 levels with VEGF levels in 46 patients with endometriosis cysts attending several hospitals in Bandung.

r: Spearman’s rank correlation.

Correlation between IL-32 levels with VEGF level in 46 patients with endometriosis cysts attending several hospitals in Bandung.
Table 5 shows the correlation between IL-32 levels and BMI has a coefficient (r) of 0.065, indicating a weak positive correlation. The p-value of 0.666 shows that this result is not statistically significant. The correlation between IL-32 levels and the duration of infertility has a coefficient (r) of −0.005, indicating a very weak negative correlation, with a p-value of 0.978, showing that this result is also not statistically significant.
Correlation between IL-32 levels with BMI and duration of infertility in 46 patients with endometriosis cysts attending several hospitals in Bandung.

r: Spearman’s rank correlation.
Table 6 shows the correlation between VEGF levels and BMI has a coefficient (r) of 0.234, indicating a weak positive correlation. The p-value of 0.117 suggests that this result is not statistically significant. The correlation between VEGF levels and the duration of infertility has a coefficient (r) of −0.005, indicating a very weak negative correlation, with a p-value of 0.975, showing that this result is also not statistically significant.
Correlation between IL-32 levels with VEGF levels in 46 patients with endometriosis cysts attending several hospitals in Bandung.

r: Spearman’s rank correlation.
Discussion
Endometriosis is a chronic inflammatory disease characterized by the presence of tissue resembling endometrium outside the uterus. 1 The pathogenesis of endometriosis is complex. The growth of endometriosis lesions involves interactions among endocrine, immunological, pro-inflammatory, and pro-angiogenic processes. 14 Endometriosis can cause symptoms such as dysmenorrhea, dyspareunia, dysuria, dyschezia, rectal bleeding with pain, hematuria, catamenial pneumothorax, and infertility. 1 These issues arise due to inflammatory processes being activated, involving cytokine pathways such as increased IL-32 and the angiogenesis factor VEGF. One factor that can inhibit inflammation is vitamin D in its active form, 1,25(OH)2D3. Vitamin D plays a molecular role as an anti-proliferative, anti-inflammatory, and immunomodulatory agent. 15
In this study, subjects selected for research sample material were patients with histopathologically confirmed endometriosis cysts, ranging in age from 20 to 42 years. The majority of subjects were in the age group of 31–36 years, comprising 34.8% of the subjects. This is consistent with the theory that endometriosis has the highest incidence between the ages of 30 and 34 years. 2 Another characteristic examined in this study was BMI. The average BMI in the study sample was 24.12 kg/m² with a standard deviation of 4.31 kg/m², indicating that on average, subjects fell within the normal BMI category (18.5–24.9 kg/m²), with some variations toward the overweight category (25–29.9 kg/m²). These study findings align with those reported by Carson et al., 16 indicating an average BMI of 25 kg/m² among endometriosis patients, and all subjects in the sample were nonsmokers, thereby concluding that smoking was not a confounding variable in this study. The study also investigated the duration of infertility (months) and found that 89.1% of the research subjects experienced infertility for more than 12 months, while only 10.9% did not experience infertility. These research findings are consistent with theories proposed by Taylor et al., 17 suggesting that more than 50% of endometriosis patients experience infertility issues.
This study explains that there is a negative correlation between the levels of 1,25(OH)2D3 and IL-32 in endometriosis cyst tissue (r = −0.346; p = 0.019). This indicates that an increase in 1,25(OH)2D3 levels is followed by a decrease in IL-32 levels, and vice versa, with a significance value of p < 0.05, showing that the results of this study are statistically significant. The findings of this study are consistent with those proposed by Bharali et al., 11 suggesting that vitamin D can reduce IL-32 levels by suppressing the IκB kinase β (IKKβ) pathway. 11 Another theory, proposed by Gatera et al., 12 states that one of the benefits of vitamin D in reducing inflammation is by lowering cytokine levels produced by the body. This study also found a negative correlation between the levels of 1,25(OH)2D3 and VEGF in endometriosis cyst tissue (r = −0.316; p = 0.032). This indicates that an increase in 1,25(OH)2D3 levels tends to be followed by a decrease in VEGF levels, with a significance value of p < 0.05, demonstrating that these results are statistically significant. Vitamin D is capable of suppressing the expression of VEGF, a crucial angiogenic factor that plays a significant role in the formation of new blood vessels. 18 Similar findings have been reported in studies on patients with colorectal cancer, indicating that 1,25(OH)2D3 suppresses VEGF through the Wnt/b-catenin pathway in cell nuclei indirectly by inhibiting the Notch pathway in angiogenesis processes. 19 Another study by Irani et al. 20 also showed that vitamin D3 supplementation in patients with polycystic ovary syndrome can reduce VEGF levels.
In this study, the correlation between VEGF and IL-32 levels in endometriosis cyst tissue was also analyzed, revealing a positive correlation (r = 0.490; p = 0.001). This indicates a direct relationship between IL-32 and VEGF levels, meaning that an increase in IL-32 levels is associated with an increase in VEGF levels, and vice versa. The significance value of p < 0.05 shows that this correlation result is highly statistically significant. These findings align with the theory proposed by Shim et al., 21 stating that IL-32 plays a crucial role in both innate and adaptive immune responses and can induce various cytokines such as TNF-α, IL-1β, IL-6, IL-8, and VEGF. Other studies by Nishida et al. 22 and Jafrin et al. 23 have explained that IL-32 can enhance angiogenesis by stimulating the production of VEGF and MMP, which affect cell migration and invasion. The confounding variables examined in this study include the correlation between IL-32 levels and BMI, which showed a positive correlation (r = 0.065; p = 0.666). This indicates a positive relationship between IL-32 levels and BMI, but because the p-value is >0.05, these results are not statistically significant. Research by Catalán et al. 24 states that IL-32 increases in obesity and can induce inflammation processes in adipose tissue and the extracellular matrix. IL-32 is regulated in obesity, promoting inflammation and remodeling of the extracellular matrix in adipose tissue, inducing the expression of pro-inflammatory cytokines and genes related to extracellular matrix in human adipocytes. 25 This study also analyzed another confounding variable regarding the correlation between IL-32 levels and infertility duration (r = −0.005; p = 0.978). The correlation coefficient (r) being very close to zero indicates that there is almost no linear relationship between IL-32 levels and infertility duration. In this context, changes in IL-32 levels are not related to changes in infertility duration, and with a p-value > 0.05, these results are not statistically significant. This differs from the findings presented by Ehsani et al., 26 who suggest that IL-32 can indirectly affect cytokine levels, disrupting the balance between pro-inflammatory and anti-inflammatory responses that may lead to infertility. An increase in the ratio of pro-inflammatory to anti-inflammatory cytokines occurs in women with unexplained infertility.
Limitation of study
Limitations of this study include a limited sample size of only 46 subjects, as well as high variability in data for several variables, such as infertility duration (ranging from 12 to 240 months) and VEGF levels (ranging from 0.01 to 2.93 ng/mL). The cross-sectional, observational, and correlational design of the study also limits the ability to infer causal relationships or observe changes in 1,25(OH)2D3, IL-32, and VEGF levels over time within individuals. Consequently, we cannot assess how these biomarkers correlate with disease progression or symptom severity.
Moreover, our study did not account for confounding factors such as diet, lifestyle, genetic predispositions, or disease stage, all of which could influence biomarker levels. The population was primarily composed of Sundanese women from hospitals in West Java, limiting the generalizability of our findings to other ethnic or geographic populations. Additionally, we did not differentiate between the various types or locations of endometriosis, which would be an important consideration for understanding how these biomarkers vary across different disease phenotypes. These factors point to the need for future studies with larger, more diverse populations and longitudinal designs to explore the impact of these variables on the biomarkers of interest.
Conclusion
This study concluded that there is a statistically significant negative correlation between the levels of 1,25(OH)2D3 and IL-32, as well as between the levels of 1,25(OH)2D3 and VEGF. This finding indicates that an increase in Vitamin D levels was associated with a reduction in the levels of inflammatory cytokines, particularly IL-32 and VEGF. Additionally, there is a statistically significant positive correlation between VEGF and IL-32 levels. These findings are consistent with the anti-inflammatory properties of vitamin D, which can also suppress VEGF expression, thereby potentially reducing angiogenesis processes in endometriosis. The data from this study also indicates an interaction between inflammatory pathways and angiogenesis in endometriosis tissue, where increased VEGF levels are associated with elevated IL-32 levels. This study is the first to investigate the relationship between 1,25(OH)2D3 levels and IL-32 and VEGF levels in endometriosis cyst tissue in Indonesia. This study could serve as a foundation for future interventional studies using vitamin D supplementation to lower IL-32 and VEGF levels in endometriosis cysts, with the expectation of reducing the progressivity of the disease. However, further research on the role of vitamin D in the pathogenesis of endometriosis involving a larger number of research subjects is still needed.
Footnotes
Acknowledgements
This article has been presented as a preprint and is available at Research Square database (![]() ).
27
).
27