
Abstract
Objectives:
To explore the impact of obesity on clinical outcomes, health-related quality of life, emotional well-being, and work productivity in people/patients with obesity across six countries by body mass index and the presence of complications.
Methods:
Adelphi Real World Obesity Disease Specific Programme™ captured data related to physicians and their consulting people/patients with obesity on a weight management program or anti-obesity medication in Brazil, Canada, China, Japan, Kingdom of Saudi Arabia, and the United Arab Emirates from April to December 2022. Physicians reported data for up to eight qualifying people/patients with obesity. People/patients with obesity voluntarily completed outcome measures: 36-Item Short Form Health Survey, emotional well-being, and Work Productivity and Activity Impairment.
Results:
Of 1506 people/patients with obesity, 58% were female (mean ± standard deviation age: 41 ± 12.7 years; body mass index: 32.3 kg/m2 ± 7.7 kg/m2). Overall, 82% had ⩾1 complication (median and interquartile range: 2.0 (1.0–3.0)). People/patients with obesity struggled with weight for a mean ± SD of 64.1 ± 86.6 months with a median (interquartile range) of 3.0 (2.0–5.0) weight-loss attempts. Mean ± standard deviation 36-Item Short Form Health Survey scores for people/patients with obesity above the obesity threshold showed impairment in general health (42.3 ± 11.5), social functioning (44.3 ± 9.2), role-emotional (46.0 ± 9.3), and mental health (45.7 ± 9.6). People/patients with obesity with complications showed similar impairment. People/patients with obesity reported bother/embarrassment about their weight, with 72% worried about future weight gain. Work productivity and activity impairment scores among people/patients with obesity above the obesity threshold showed impairment in activity (36%), overall work (34%), and presenteeism (31%). Findings were similar for people/patients with obesity with complications.
Conclusion:
Results suggest that obesity alongside the presence of complications negatively impacts health-related quality of life, emotional well-being, and work productivity, reinforcing the need for comprehensive interventions for this complex health issue.
Introduction
Obesity is a chronic disease characterized by excessive body fat, increasing the risk of numerous diseases such as type 2 diabetes (T2D), cardiovascular diseases, and cancer adversely affecting overall health1,2 and leading to premature death. 3 Obesity can cause significant psychological problems such as depression, stress, and anxiety. 1 While obesity is increasingly being recognized as a disease, there is a need for significant national policies to prevent and manage obesity and its long-term effects.4–8
Overweight and obesity are widespread in the World Health Organization (WHO) European region and affect nearly 60% of adults, with about one-quarter (23%) living with obesity. 9 The global prevalence of obesity (body mass index (BMI) ⩾ 30 kg/m2) is predicted to increase from 14% in 2020 to 24% by 2035, affecting nearly two billion people, including children and adolescents. 4 However, obesity prevalence is underestimated due to several reasons including variability in BMI classifications and the extent of underdiagnosis 10 BMI is one of the most frequently used clinical measures to classify and characterize obesity, but country-specific modifications to this classification exist. Some countries have independently established their guidelines to consider country-specific population risk. The WHO defines overweight and obesity as a BMI of 25 to <30 kg/m2 and ⩾30 kg/m2, respectively. 11 The WHO Regional Office for the Western Pacific, International Association for the Study of Obesity, and International Obesity Task Force proposed different cutoffs according to three broad population groupings, with overweight defined as BMI ⩾ 23 kg/m2 for Asian populations, ⩾25 kg/m2 for European populations, and ⩾26 kg/m2 for Pacific Island populations.12,13
The three main pillars for treating obesity are lifestyle modifications comprising nutrition, physical activity, and behavioral interventions; anti-obesity medication (AOM); and bariatric surgery.14,15 Lifestyle and behavioral interventions provide moderate efficacy and should be considered in all people/patients with obesity (PwO), independent of other obesity treatments (AOM or surgical interventions). Although first-generation AOMs have been used over the years, their use in routine clinical practice has been limited, and some have been withdrawn from the market due to safety concerns. 16 Several reasons exist for the limited use of AOMs, such as the stigma surrounding obesity and the perception that AOMs are only for short-term use. 17 Next-generation AOMs such as glucagon-like peptide-1 receptor agonists and glucose-dependent insulinotropic polypeptide agonists are entering the market with greater efficacy, leading to meaningful health improvements for PwO.17–21 Bariatric surgery also represents an effective weight-loss approach. 22 Despite these treatment options, access to obesity care is limited23,24 and significantly varies by region and socio-economic status. 25
Obesity also poses a significant economic burden on healthcare systems and PwO, resulting from direct treatments along with treating associated complications such as T2D. 2 The burden includes direct treatments, associated complications, increased healthcare services usage, more medications, and reduced productivity.26,27 According to Neovius et al., 28 productivity losses are twice as high for PwO than for people with a healthy weight (defined as BMI ⩾18.5 kg/m2–<25 kg/m2) over a lifetime. A study comprising data from 161 countries estimated the economic impact of overweight/obesity to be 2.19% of the global gross domestic product in 2019. 29 Obesity can also impact health-related quality of life (HRQoL) and psychosocial and emotional well-being. 30
When distinguishing obesity as a disease, evaluating the HRQoL and emotional impact of PwO against this changing backdrop is critical. While some evidence of clinical, economic, and patient-reported effects of obesity exist, large-scale multinational studies are needed. This study aimed to evaluate the impact of obesity on clinical outcomes, HRQoL, emotional well-being, healthcare resource utilization (HCRU), and work productivity in PwO across six countries using data from the Adelphi Real World Obesity Disease Specific Programme™ (DSP). The study also explored HRQoL, emotional well-being, and work productivity among PwO according to obesity threshold and presence of complications.
Methods
Study design and population
This observational multinational study was conducted in six countries (Brazil, Canada, China, Japan, Kingdom of Saudi Arabia [KSA], and United Arab Emirates [UAE]) based on data drawn from the Adelphi Real World Obesity Disease Specific Programme (DSP)™, a cross-sectional survey with retrospective data captured from April to December 2022. This DSP was a patient record-based survey of PwO and physicians managing PwO (including primary care physicians [PCPs]/internists, diabetologists/endocrinologists, cardiologists, and obstetricians/gynecologists [OB/GYN]), based on one of the six countries (Figure 1). The DSP methodology has been previously described,21,31 validated, 32 and shown to be representative and consistent over time. 33

Obesity disease-specific program methodology.
The DSP study population comprised physicians and their consulting PwO (aged ⩾ 18 years) with a confirmed obesity diagnosis as defined by enrollment in a weight management program and/or a BMI ⩾ 30 kg/m2 in Brazil, Canada, KSA, and UAE, ⩾28 kg/m2 in China, or ⩾25 kg/m2 in Japan. PwO were excluded from participation in the DSP if they were involved in a clinical trial for obesity at the time of recruitment. PwO were recruited into either of two groups: (1) PwO receiving AOM and (2) PwO not receiving AOM. Obesity was defined as a BMI ⩾ 30 kg/m2 in all countries except China (⩾28 kg/m2) and Japan (based on the Japan Society for the Study of Obesity definition: ⩾25 kg/m2 with ⩾1 condition including glucose intolerance disorder, dyslipidemia, hypertension, gout, cardiovascular disease, cerebral infarction, nonalcoholic fatty liver disease, sleep/breathing issues, motor dysfunction, and renal disease). 34 At the time of data collection, all PwO had an obesity diagnosis or were being treated for obesity but may not have had a BMI indicating obesity. Of note, some PwO may not have had a BMI indicating obesity at the time of data collection due to successful weight loss as a result of a weight loss program. This approach aligns with recent literature. 35
Physicians in the DSP were recruited from lists of healthcare professionals (HCPs). Participating physicians had to manage at least 10 PwO in Canada, KSA, and UAE, 6 PwO in Japan, and 16 PwO in China and Brazil per month.
Physician- and patient-reported questionnaires
Eligible physicians were instructed to complete a physician-reported form for the first eight PwO they saw who met inclusion criteria. Physicians provided clinical and obesity characteristics for each of their PwO enrolled in the DSP. PwO for whom their physician completed a physician-reported form were invited to complete a voluntary, confidential, patient-reported form immediately after consultation. This was completed via a secure online platform or returned in a sealed envelope, ensuring the patient’s responses were kept confidential from their physician. PwO also provided data on work productivity and activity impairment, as well as HRQoL via validated patient-reported outcome measures (PROMs). Results reported here are of physicians who completed the physician-reported form and their PwO who completed the patient-reported form, which produced matched data. Results are calculated from matched data of physicians and PwO, aggregated across all countries.
Survey measures
The measures reported in this study from the linked physician- and patient-reported form data sources are briefly described below (see also Supplemental Tables S1 and S2).
Clinical and obesity characteristics
Clinical characteristics of PwO included sex, age, a predefined list of complications, and smoking status. Obesity characteristics included the number of days since obesity diagnosis, body weight and BMI at diagnosis, the number of months the PwO struggled with weight, and the number of discrete weight-loss attempts. Examples of questions asked to physicians and PwO include the following: “To the best of your knowledge, when did this patient start living with obesity or require weight reduction?” and “How long do you feel you have struggled with your weight?”
HRQoL impact of obesity
HRQoL was measured using the 36-Item Short Form Health Survey (SF-36v2) 36 for eight health domains: physical functioning, bodily pain, role limitations due to physical health problems (role-physical), role limitations due to personal/emotional problems (role-emotional), emotional well-being (mental health), social functioning, energy/fatigue (vitality), and general health perceptions. After the eight health domains were scored, two overall summary scores were calculated—a physical component summary (PCS) and a mental component summary (MCS). T-scores, a method for analyzing probability by how far a data point is from the mean, were interpreted in relation to normative data from the US general population in 2009 (mean ± standard deviation [SD]: 50 ± 10). A T-score of 47 to 53 was considered within the “normal” range for the US general population. Scores <47 indicated impairment in the specific domain. 37
Emotional impact of obesity
Other questions for PwO included how bothered they are about their current weight, if they ever feel embarrassed about their weight in public, if other people make them feel ashamed of their weight, and if they are concerned about putting on weight in the future.
Impact of obesity on HCRU and work-related outcomes
Measures included socioeconomic status (low, intermediate, or high based on employment status, education level, and health insurance coverage); employment status; education level; and health insurance coverage (funding for obesity treatment). HCRU was measured via the number of obesity-related visits to HCPs (e.g., PCP, endocrinologist, diabetologist, cardiologist, OB/GYN, nurse practitioner, and other); the number of hospitalizations including surgery in the last 12 months; and the percentage of total monthly household income spent on medicines for obesity and other obesity-related health complications. Lost productivity and activity impairment due to obesity were measured using the validated Work Productivity and Activity Impairment (WPAI) questionnaire. The WPAI measures absenteeism (percentage of work hours missed due to obesity), presenteeism (percentage of impairment while working due to obesity), and overall work impairment (overall percentage of work hours affected due to obesity) in the subset of PwO currently employed, along with overall activity impairment (overall percentage of daily activities affected due to obesity) collected from all PwO, regardless of employment status. Scores range from 0% to 100%, and higher scores indicate greater impairment. 38
Sample size and statistical power
This study was descriptive, so no sample size calculations were required. The analysis population consisted of all physicians and PwO contributing data to the DSP. The sampling of the survey respondents was geographically representative.
Analysis
Descriptive summary statistics were generated for all assessments and are reported as mean ± SD or frequency and percentage. Missing data were not imputed; thus, the base number of PwO for analysis could differ by variable and was reported separately for each analysis. Subgroup analyses were conducted to examine results by SF-36v2, emotional impact, and WPAI questions overall; below obesity threshold: BMI < 30 kg/m2 in Brazil/Canada/KSA/UAE, <28 kg/m2 in China, and <25 kg/m2 in Japan, who have had a reduction in BMI owing to an obesity-management program; above obesity threshold: BMI ⩾30 kg/m2 in Brazil/Canada/KSA/UAE, ⩾28 kg/m2 in China, and ⩾25 kg/m2 in Japan.
Results
Overall, 1506 PwO who completed the patient-reported form and had data available from the physician-reported form were included in the analysis. For PROMs, the SF-36v2 and emotional impact questions included 1506 PwO and the WPAI included 1463 PwO.
Clinical and obesity characteristics
Of all included PwO, 58% were female with a mean ± SD age and BMI of 40.8 ± 12.7 years and 32.3 ± 7.7 kg/m2, respectively (Table 1). PwO had a median (interquartile range (IQR)) of 2.0 (1.0–3.0) complications, and 82% had ⩾1 complication. The most commonly reported complications included dyslipidemia (34%), hypertension (33%), T2D (18%), and anxiety (15%). Overall, 68% of PwO had never smoked. The mean ± SD number of days since an obesity diagnosis for PwO was 803.0 ± 1326.8. PwO had struggled with weight for a mean ± SD of 64.1 ± 86.6 months, with a median (IQR) of 3.0 (2.0–5.0) discrete weight-loss attempts. Mean ± SD weight loss since diagnosis was 11% ± 10.6% for PwO below the obesity threshold, 5% ± 7.0% for PwO above the obesity threshold, and 6% ± 7.8% for those with complications.
Clinical and obesity-related characteristics of PwO.
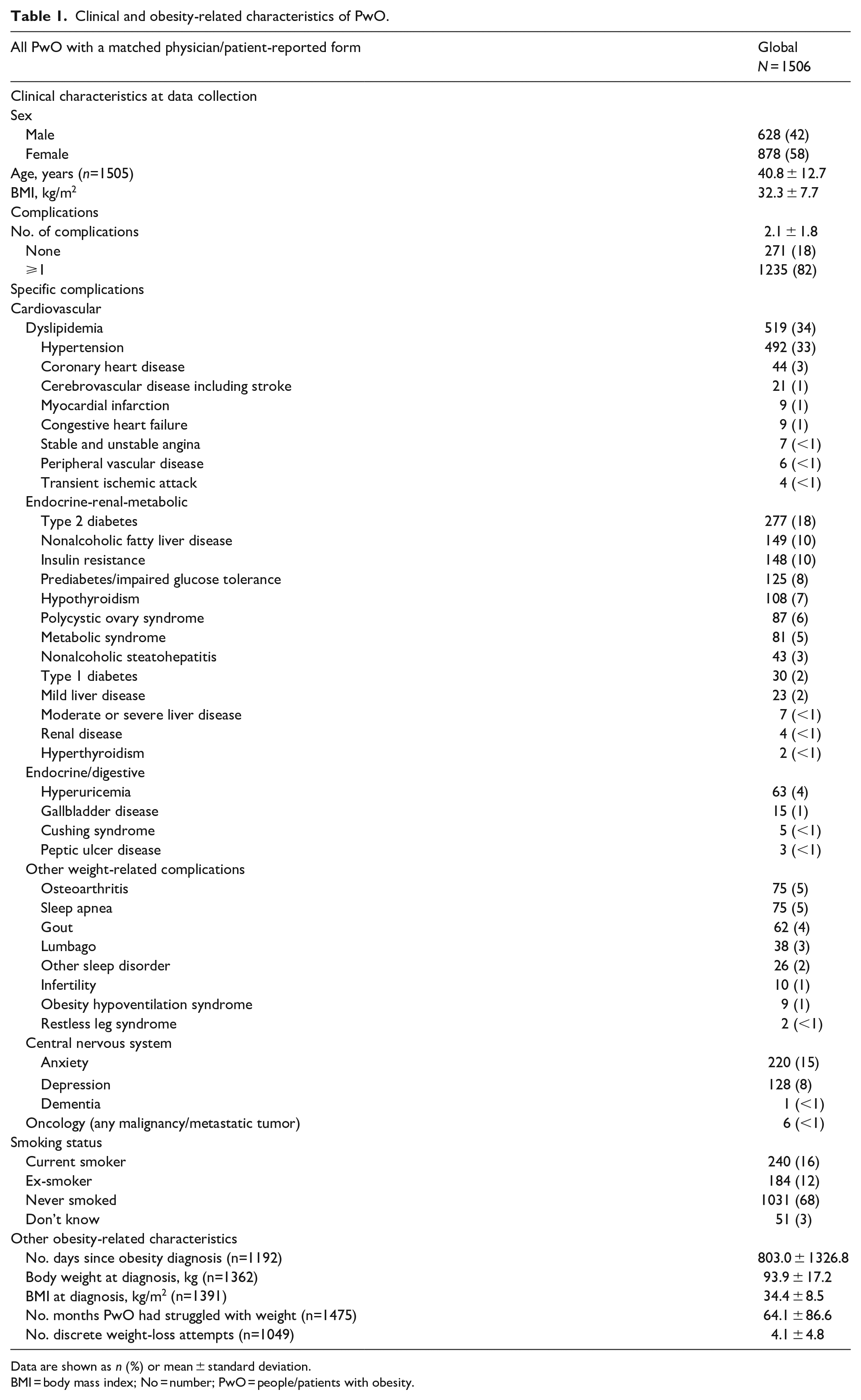
Data are shown as n (%) or mean ± standard deviation.
BMI = body mass index; No = number; PwO = people/patients with obesity.
HRQoL impact of obesity
Overall, mean scores for PwO were below the population norm on 4 of 8 SF-36v2 domains (mean ± SD): general health (43.1 ± 11.4), social functioning (44.6 ± 9.1), role-emotional (46.2 ± 9.2), and mental health (45.9 ± 9.4). Summary scores for PwO were also below the population norm: MCS (46.0 ± 9.3) (Figure 2(a)).
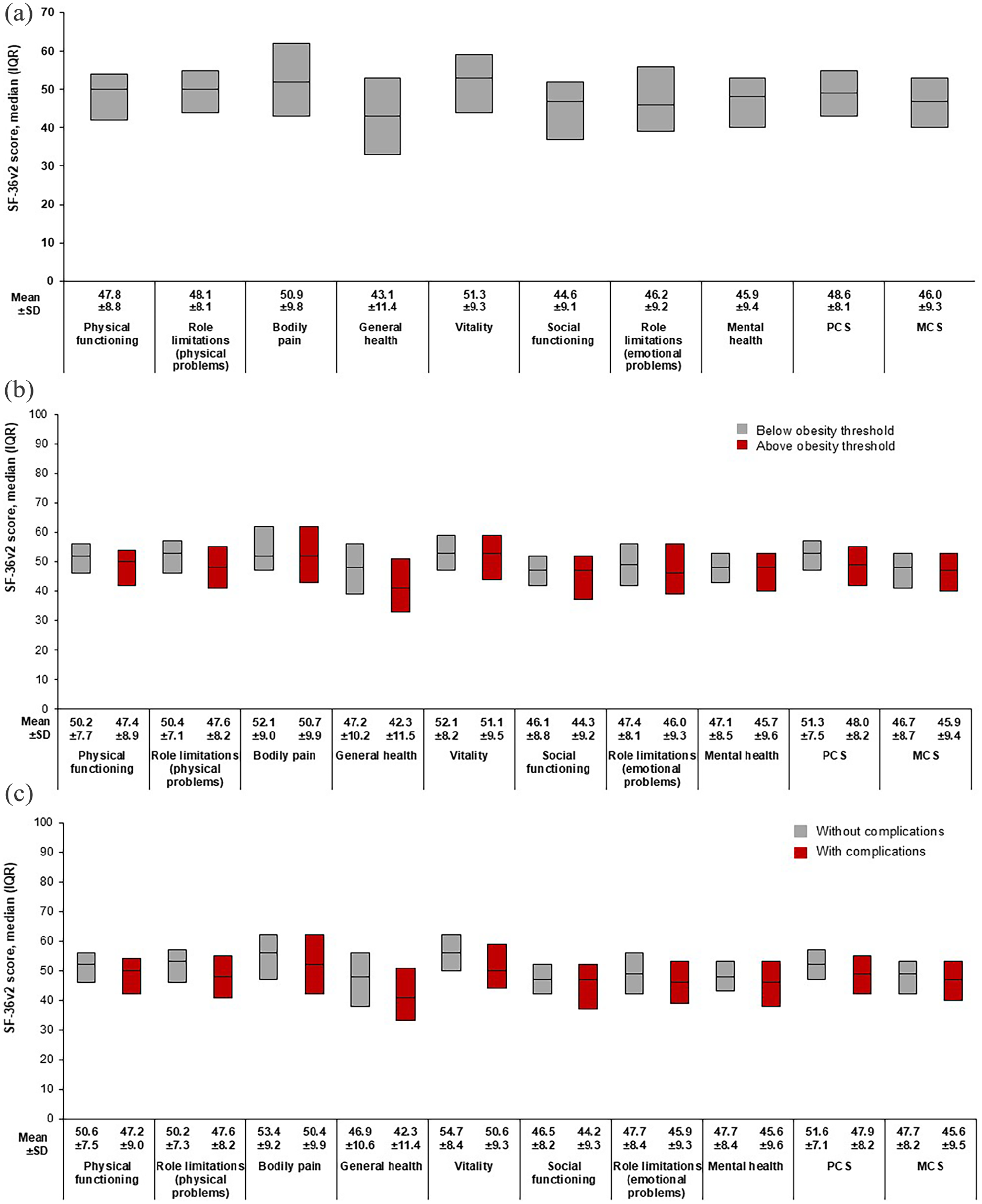
Patient-reported health-related quality of life: SF-36v2 overall domain scores (a), SF-36v2 scores by obesity status at time of data collection (b), and SF-36v2 scores by presence of complications (c).
Scores for PwO above the obesity threshold at the time of data collection showed HRQoL impairment in 4 of 8 SF-36v2 domains (mean ± SD; general health, 42.3 ± 11.5; social functioning, 44.3 ± 9.2; role-emotional, 46.0 ± 9.3; and mental health, 45.7 ± 9.6) and in the MCS score (45.9 ± 9.4) (Figure 2(b) and Figure S1). Similarly, PwO with complications showed HRQoL impairment in the same four domains and the MCS score (Figure 2(c)).
Emotional impact of obesity
Most PwO reported a degree of bother about their weight (66%), which was reported by 68% of those above the obesity threshold and 71% of those without complications (Figure 3(a) and Figure S2a). Similarly, 53% of PwO reported a degree of embarrassment about their weight, reported by 55% of both those above the obesity threshold and those without complications (Figure 3(b) and Figure S2b). More than half of PwO felt that other people made them feel ashamed of their weight (54%) (Figure 3(c) and Figure S2c), with 72% worried they would gain more weight in the future (Figure 3(d) and Figure S2d).
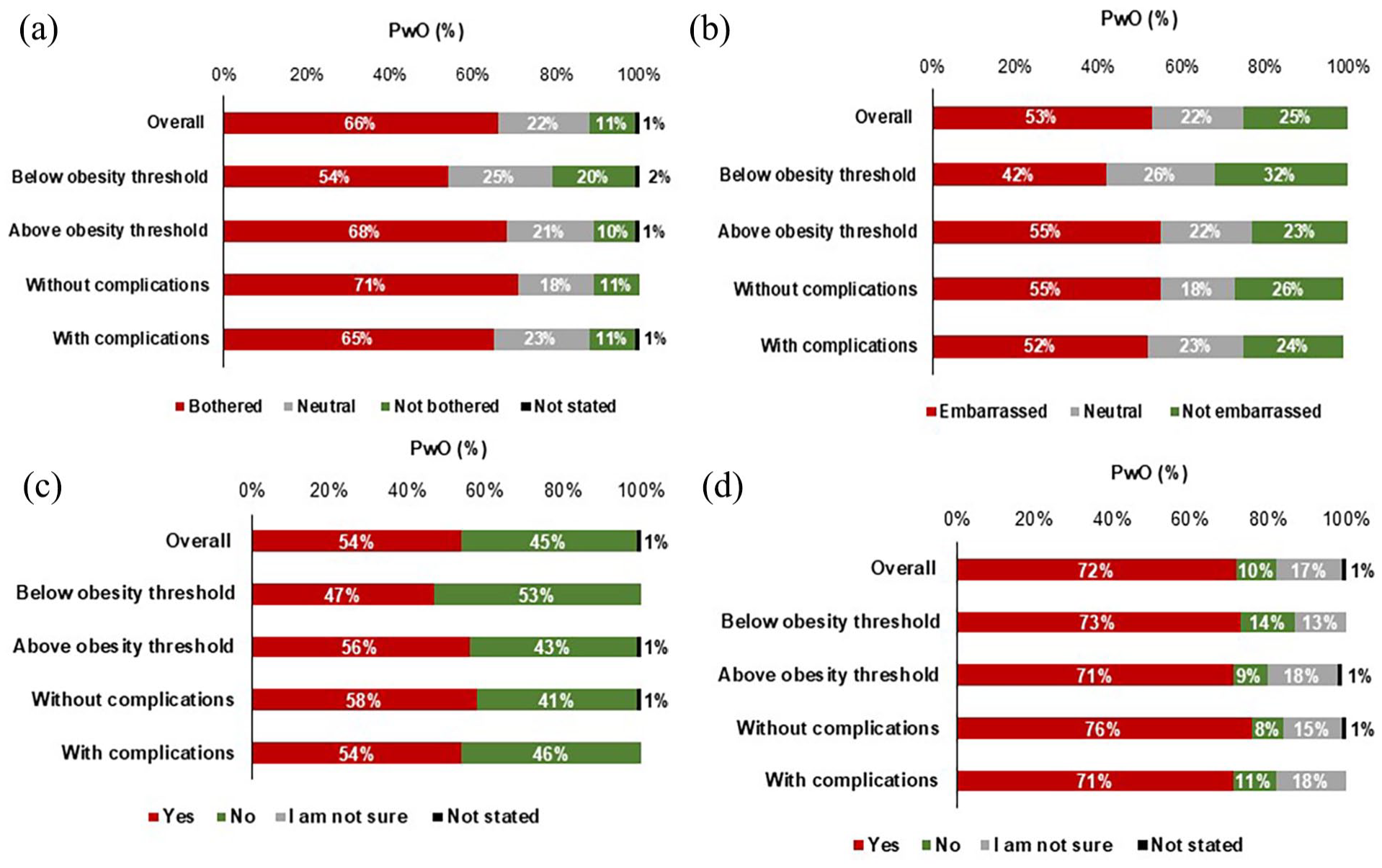
Patient-reported emotional impact: perspectives regarding weight by obesity threshold and presence of complications.
Impact of obesity on HCRU and work-related outcomes
PwO presented with similar socio-economic statuses of low (43%) and high (42%). In terms of patient-reported employment (n = 1506), 70% (n = 1053) of PwO were working (62% (n = 939) full time and 8% (n = 114) part time) and 30% (n = 453) were not working. Among PwO who reported being on long-term sick leave, retired, or unemployed (n = 231), 86% (n = 198) reported this was a result of their condition (Table 2). Overall, 59% (n = 887) of PwO were educated at an undergraduate level or higher. Of 1498 responding PwO, 45% (n = 667) reported paying out-of-pocket expenses for obesity treatment. Respondents (n = 1092) reported spending a mean ± SD of 9.9% ± 9.8% of their total monthly household income on obesity treatment. PwO reported visiting a PCP/internist or endocrinologist at a mean ± SD of 2.7 ± 3.0 (n = 1205) and 2.3 ± 2.8 (n = 1183) times, respectively, in the past 12 months.
Impact of obesity on healthcare resource utilization and work-related outcomes.

Data are shown as n (%) or mean ± standard deviation.
HCP, healthcare professional; No., number; PwO, people/patients with obesity.
Mean WPAI scores among PwO above the obesity threshold showed higher levels of activity impairment (36%), overall work impairment (34%), and presenteeism (31%) than those for PwO below the obesity threshold (Figure 4(a) and Figure S3). Similarly, mean WPAI scores among PwO with complications demonstrated increased activity impairment (36%), overall work impairment (34%), and presenteeism (31%) versus scores for PwO without complications (27%, 26%, and 24%, respectively) (Figure 4(b)).

Patient-reported economic impact: WPAI scores by obesity threshold (a) and presence of complications (b).
Discussion
This large-scale multinational study highlights the burden and impact that obesity can impose on HRQoL, emotional well-being, and work productivity on PwO and healthcare systems. This real-world data analysis shows that most PwO who attend a clinical practice had ⩾2 complications such as hypertension, dyslipidemia, and T2D, which is comparable to prior research identifying obesity as an entryway to a range of non-transmittable diseases that adversely affect overall health.1–3 Physicians in this study reported that PwO struggled with their weight for several months before a formal diagnosis. PwO may develop obesity-related complications within the time it takes to receive a diagnosis, which explains the high complication rates. Results from the ACTION-IO study showed that PwO and HCPs had differing opinions on weight management, causing a mean 9-year delay in discussions. 39 Furthermore, obesity is not always treated as a disease despite being classified as such,5–8 and discussions around weight management are deprioritized among HCPs. 40 In a study evaluating whether obesity diagnoses and treatment plans are documented among PCPs, only 1 of 5 PwO had their disease documented and a management plan established. 41 In addition, follow-up care for obesity is not routine. 40 Research shows that obesity counseling occurs more often among patients with complications, particularly those with diabetes. 41 HCP education is crucial to change obesity perceptions and disease management. HCPs should also be encouraged to schedule follow-up visits focusing on the obesity diagnosis and management plan. 40
Consistent with previous literature, HRQoL findings in this study showed impairment in general health, social functioning, and mental health domains and the MCS score, with similar results observed for PwO above the obesity threshold and those with complications. Impaired HRQoL among PwO has been seen in European-based studies,42–44 and studies with Asian 45 and South American 46 populations. Research has shown that even a moderate reduction in weight is associated with improved HRQoL.47,48 Although greater impairment for MCS was demonstrated in this study, a greater difference, between those with a BMI over 30 versus those with a BMI under 30 at the time of data collection, for the physical component was also evident (Figure 2(b)). Impaired physical (but not mental) HRQoL was found among 2732 surveyed PwO in Germany, 43 while Baumeister and Härter 44 reported an association between increasing weight and risk of mental health conditions. AOMs and bariatric surgery have demonstrated positive and sustainable effects on HRQoL. 49 However, little is known about whether increased HRQoL is sustained given the difficulties in losing weight and maintaining weight loss. 47 From a public health perspective, efforts should be made to develop and implement treatments that address the biopsychosocial impact of excess body weight.
PwO reported feelings of bother and embarrassment about their weight, with results suggesting comorbidities do not substantially impact PwO perceptions in this regard. This is corroborated by a qualitative study of experiences and expectations of PwO seeking bariatric surgery wherein participants reported persistent shame and embarrassment regarding their appearance, worried that others would think they had “let themselves go.” 50 Research has shown that weight bias among healthcare settings results in insensitive care and shaming of patients, impeding access to effective obesity management. 51 HCPs should develop a patient-centered approach by being sensitive to the emotional impact that obesity has on self-esteem 52 and taking actions to reduce weight bias in patient care. 51
PwO reported spending, on average, 9.9% of their total monthly household income on medicines for weight and other obesity-related health complications. In a study evaluating BMI and its associated costs, PwO reported higher obesity-related indirect and total direct costs compared with normal-weight respondents. 53 While out-of-pocket costs were identified in our study, the extent to which these might be refunded by insurance plans was not available. Obesity-related HCRU among PwO was mainly for PCP or endocrinologist appointments, with an average of two visits in the previous year for obesity-related concerns. Research shows that PwO may require more time with their HCP and more follow-up appointments, which may not be adequately reimbursed by health insurance. 54 However, obesity management and treatment may help lower healthcare costs. 51 In this study, PwO above the obesity threshold and those with complications had higher activity impairment, overall work impairment, and presenteeism. Similarly, Finkelstein et al. 55 found that healthcare costs, absenteeism, and presenteeism were all higher among PwO, and a health and wellness survey in Europe found that PwO had significantly increased work-related productivity loss. 53
This study provides valuable insight into the impact of using the widely published and validated DSP methodology, while collecting uniform data for cross-country comparisons, reflecting real-world practice. Other strengths include the population size, coverage, and collection of clinical characteristics and PROMs. Using matched data from physicians and their PwO provides important insights on HRQoL and emotional well-being among a multi-country sample, helping to fill a critical gap in the literature.
It is important to note the limitations of this study. The cross-sectional design of this study prevents any conclusions about causal relationships; however, the identification of significant associations is possible. Physicians were asked to provide data for a consecutive series of patients to avoid selection bias, but no formal patient selection verification procedures were in place. PwO who participated in the surveys may not reflect the general obesity population as patients are visiting their physician and are those who visit more frequently and may be more severely affected than those who do not consult their physician as frequently. Recall bias might also have affected the responses of both patients and physicians to the questionnaires, which is a common limitation of surveys. However, the data for these analyses were collected at the time of each patient’s appointment and this is expected to reduce the likelihood of recall bias. Although all PwO were invited to provide PROMs, only a subsample of patients did so, and the extent to which this subpopulation is systematically different from the pool of patients who were invited remains unclear. While it would be interesting to assess the differences, it is out of scope for this study. No sample size calculations, or adjustments for bias or confounding, were performed owing to the descriptive nature of the study. The sample size was also dependent on feasibility. PROMs may be influenced by additional factors beyond BMI and complications not currently captured in the analysis, such as the extent of weight loss as a result of weight management. However, exploration of these was limited by the lack of data on changes in PROMs from baseline. Future research to further investigate this and other associated factors is warranted. Finally, study findings may not be generalizable to the entire obesity population. As AOM use was higher in this study, owing to its design, the characteristics of the study population reflect those seeking care or undergoing some type of intervention.
Conclusion
Results suggest that obesity alongside the presence of complications negatively impacts HRQoL, emotional well-being, and work productivity. The evidence from this study reinforces the need for broad and effective interventions/treatment plans implemented early to avoid disease progression and the development of further obesity-related complications.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241313082 – Supplemental material for Experiences and overall impact reported by people living with obesity: results from a multinational study
Supplemental material, sj-docx-1-smo-10.1177_20503121241313082 for Experiences and overall impact reported by people living with obesity: results from a multinational study by Esther Artime, Swarna Khare, Sarah Zimner-Rapuch, Josefine Redig, Caragh Flannery, Victoria Higgins, Andrea Leith, Ashley Mortimer, Bruno Halpern and Nasreen Alfaris in SAGE Open Medicine
Footnotes
Acknowledgements
Quality review and editorial support were provided by Adrienne Schreiber of Syneos Health, funded by Eli Lilly and Company.
Author contributions
EA, SK, SZR, and JR were responsible for clinical oversight and guidance as lead authors. Study setup and data collection were led by VH, AL, and AM. Analysis design was conducted by VH, AL, and AM with analyses prepared by VH, AL, and AM. All authors wrote the manuscript supported by a medical writer. All authors participated in manuscript development and finalization, assume responsibility for the accuracy and completeness of the data, and vouch for the study’s fidelity to the protocol. VH is the guarantor of this work, has full access to all the data, and takes full responsibility for the integrity of data and accuracy of the data analysis.
Data availability statement
All data relevant to the analysis are included in the article. All data that support the findings of this survey are the intellectual property of Adelphi Real World. The data sets generated and/or analyzed during the current study are available upon reasonable request to Victoria Higgins at Victoria.Higgins@adelphigroup.com.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EA, SK, SZR, JR, and CF are employees and minor shareholders of Eli Lilly and Company. VH, AL, and AM are employees of Adelphi Real World. BH reports payment or honoraria from Abbott Nutrition, AstraZeneca, Eli Lilly and Company, Merck SA, and Novo Nordisk; travel/meeting support from Novo Nordisk; participation on a Data Safety Monitoring Board or Advisory Board for Eli Lilly and Company, Merck SA, and Novo Nordisk; receipt of equipment, materials, drugs, medical writing, gifts, or other services from Eli Lilly and Company and Novo Nordisk; and is President of the Brazilian Association of Obesity and a Member of Board of Trustees of World Obesity Federation representing Latin America. NA has provided consultancy to Novo Nordisk.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This analysis was funded by Eli Lilly and Company. Data collection was undertaken by Adelphi Real World as part of an independent survey, entitled the Adelphi Real World Obesity Disease Specific Programme (DSP). Eli Lilly and Company did not influence the original survey through either contribution to the design of questionnaires or data collection. The analysis described here used data from the Adelphi Real World Obesity DSP. The DSP is a wholly owned Adelphi product. Eli Lilly and Company is one of multiple subscribers to the DSP.
Ethics approval
Ethical approval for this study was waived by the Pearl Institutional Review Board (Approval No. #22-ADRW-136) for Brazil, Canada, China, Japan, KSA, and UAE.
Informed consent
Written informed consent was obtained from all subjects before the study. All participants provided written informed consent for using their anonymized and aggregated data.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.