
Abstract
Background:
OULA is a high-energy dance workout to top 40 hits that is inspired by yoga and non-impact aerobics. Created in Missoula, Montana, the program has been gaining national and international popularity. To understand the demographic composition, reasons for attending OULA, and experiences with depression/anxiety, we conducted an Internet-based survey.
Methods:
A pilot descriptive cross-sectional Internet-based survey was created in Qualtrics and distributed through social media and flyers.
Results:
The 38-item survey received responses from 302 participants. Current OULA participants chose “exercise” as the primary reason for attending (40.2%, 95% confidence interval: 33.3–48.2), followed by “stress relief/improve mood” (28.8%, 95% confidence interval: 23.0–35.6). Participants listed “stress relief/improve mood” as the most common secondary (35.6%, 95% confidence interval: 29.0–43.2) and tertiary (38.6%, 95% confidence interval: 31.7–46.7) reason for attending OULA. A majority of the participants said that OULA makes them feel like part of a community (93.2%, 95% confidence interval: 82.5–105.1) and increases their energy outside of class (80.1%, 95% confidence interval: 70.2–91.1). In our sample, 12.5% (95% confidence interval: 8.8–17.1) and 9.0% (95% confidence interval: 5.9–12.9) were currently taking antidepressants and anxiolytics, respectively.
Conclusion:
These results suggest that current OULA participants are already using the program to relieve stress or improve mood. Further research should be conducted to understand the relationship between OULA and depression/anxiety.
Introduction
It is consistently documented that both exercise1–7 and dance,8–16 including dance movement therapy17,18 and Biodanza®,19–22 have beneficial physical and psychological effects for both healthy individuals and individuals with medical and psychiatric diagnoses. The combination of dance and exercise (i.e. dance fitness) has also been shown to have a positive effect on body composition and mood.23–25 The dance fitness industry is ever changing with new formats being created each year. The dance fitness program OULA, named after the city of Missoula, Montana, has been gaining popularity since its creation in 2010.
OULA is a high-energy dance workout to Top 40 hits. Kali Lindner created the program based on philosophies from Yoga and non-impact aerobics (NIA) technique. 26 Comparable to other popular group exercise programs, such as Zumba®, Biodanza®, and Jazzercise, OULA is a dance-oriented form of fitness. However, like Biodanza®, OULA differs from most other dance fitness programs in that it focuses on the mind–body connection and offers an environment for participants to safely experience emotions via song and dance. In contrast to Biodanza®, which is a free form of dance, OULA is choreographed to carefully selected songs that focus on connection with the self and others, femininity, power, determination, letting go, and love. The primary focus of OULA is how a participant feels as opposed to how they look. In a traditionally image-obsessed fitness industry, participants have the opportunity to exercise in a judgment-free zone. This approach to fitness is designed to build self-confidence while improving overall health.
Community is an important aspect of OULA, as one of the main underpinnings of OULA is connection with self and others. Bringing people together to dance and sing allows opportunity for social interaction and friendships are formed. Instructors and OULA participants are warm and inviting by introducing themselves to new participants before the start of their first class. Given that the need to belong is a fundamental part of human existence,27,28 a fitness model that provides a friendly environment may help generate higher self-esteem and self-worth and bolster success.
There are several OULA formats, each with different techniques. OULA is the original format, and it has an emphasis on dancing to top 40 hits. OULA.One has a focus similar to yoga; it includes stretching, deep breathing, holding poses to build strength, and practicing mindfulness. Further, OULA.One encourages emotional awareness by lying on floor mats at the end of the session and focusing on breathing to become more emotionally in-tune. There is also OULA Power, which has a cardio and strength training emphasis and is the most physically taxing form of OULA. Since each of these formats can be practiced at an individual’s own pace, they are all available to a variety of ages and skill levels. Finally, the fourth format of OULA is OULA Jr., which is an OULA class for children and adolescents.
Aerobic exercise and dance are gaining popularity among clinicians as complementary and alternative ways of treating depression and anxiety. Consistent research findings have shown benefits from exercise combined with medications for depression. 29 Further, in randomized controlled trials comparing exercise with antidepressants, studies have shown that both treatments are equally effective. 30 Recent evidence has also shown that exercise, specifically dance, can significantly reduce anxiety symptoms.6,7,16,24,31 Despite this evidence, depressive disorders are most commonly treated with medications, psychotherapy, or a combination of the two. 32 Since the 1960s, treatment of depressive disorders has relied heavily on the use of antidepressants, even though individual responses to antidepressants vary greatly among patients. 33 Antidepressants are not universally successful; an individual may have to try multiple medication treatments, some with negative side effects, before finding an antidepressant that alleviates symptoms. 34 Dance fitness is a plausible substitute for or adjunct to medications, as evidence has indicated that dance and exercise can be effective in alleviating depression and anxiety, specifically in women. 5
To our knowledge, there has not been any research conducted on OULA to date. Thus, to learn more about the demographic composition of OULA participants, their exercise habits, motivations for attending OULA, and experience with depression and anxiety, we conducted an Internet-based survey.
Methods
Design considerations
The purpose of this pilot descriptive cross-sectional study was to describe OULA participants in terms of who they are, their exercise habits, their motivations for attending OULA, and potential benefits of attending OULA. As a pilot study, the feasibility objectives were to search for potential associations that might be worth investigating in a subsequent larger trial, 35 as well as to assess the recruitment potential of OULA participants. We elected to use an Internet-based survey design to optimize generalizability and enhance the ability to capture national and international OULA participants.
Sample, eligibility, and recruitment
Data were collected via an Internet-based survey created in Qualtrics, which received 302 responses between August and October 2016. Individuals eligible to take the survey were current OULA participants. The survey was distributed through social media every other week for 3 months until there were no new respondents for 3 weeks. In addition, a recruitment card with the survey link was available at the OULA studio in Missoula, Montana. Instructors also announced the survey in their OULA classes.
Study procedure
The authors developed the survey questions. The completed survey was sent to the creator of OULA as a test of face validity 36 and questions were revised with her input to improve accuracy of the questions. The survey questions were optional and participants were able to stop the anonymous survey at any time. The survey was designed to be completed in less than 10 min and included multiple-choice questions, closed-ended questions, and rating scales. The survey included a total of 38 questions, of which 21 questions allowed for subject narrative via an “other” response option. Furthermore, some questions allowed respondents to select multiple responses, whereas other questions were on a Likert-type scale. Question content included demographics, current forms of exercise, length of OULA attendance, reasons for participating in OULA, and questions about personal history with depression and anxiety, including medication use (see Appendix 1 for the survey).
Statistical analysis
Nominal- and ordinal-level survey responses were characterized as percentages and 95% confidence intervals (CIs). The confidence limits are based on the Byar’s approximation of the exact Poisson distribution, which is extremely accurate even with small sample sizes. 37 The mean and standard deviation were calculated for continuous level data. This descriptive study was a pilot study, and a power analysis to determine the number of subjects for statistical significance was not performed.38–40 As described above, the survey was distributed via social media and in OULA classes every other week for 3 months until there were no new respondents for 3 weeks. This resulted in n = 302.
To evaluate the association between some demographic characteristics and motivations for attending OULA, Chi-square tests of association were conducted. Specifically, we re-coded demographic variables to meet the assumptions of a Chi-square test of association, 39 for example, (a) using the median age, we dichotomized age as less than 33 years and greater than 33 years; (b) we categorized level of education as 1 = no college degree, 2 = Associate’s degree, 3 = Bachelor’s degree, and 4 = Advanced degree (Master’s, Doctoral, or Professional degree); (c) we categorized length of time regularly participating in OULA as 1 = less than 2 years and 2 = more than 2 years; and (d) we dichotomized frequency of weekly OULA attendance as 1 = less than 3 days per week and 2 = more than 3 days per week. Using the three most frequent reasons for attending OULA, we categorized the primary reasons for attending OULA as 1 = exercise, 2 = fun, 3 = stress relief/improve mood, and 4 = other. Significance was set at a p-value of ⩽0.05, and data were analyzed using IBM SPSS Statistics for Mac version 25.
Ethical considerations
Montana State University Institutional Review Board (IRB) approved the survey prior to data collection. All procedures performed in the study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments. A consent paragraph was included as an introduction to the survey.
Results
A total of n = 302 survey responses were recorded. Incomplete surveys were not excluded from data analysis but only questions that were completed were included in the analysis. Of the n = 302 responses recorded, n = 282 (93.7%) individuals completed the entire survey.
Participant demographics
Of the responses recorded, n = 282 (99.3%, 95% CI: 88.2–111.4) were female and had a mean age of 35.9 years with a standard deviation of 10.8. A majority of the respondents were Caucasian (n = 265; 93.6%, 95% CI: 82.9–105.4) and married (n = 175; 61.4%, 95% CI: 52.8–71.0), and the most common level of education was a Bachelor’s degree (n = 127; 44.6%, 95% CI: 37.3–52.8). Predominantly, respondents were from Montana (n = 177; 63.2, 95% CI: 54.4–73.1). Moreover, participants were asked about personal history with depression and anxiety. Of the responses recorded, n = 35 (12.5%, 95% CI: 8.8–17.1) were currently taking antidepressants, while n = 25 (9.0%, 95% CI: 5.9–12.9) were currently taking anxiolytics. See Table 1 for a complete list of demographics.
Demographics.

GED: General Equivalency Diploma; SD: standard deviation.
Options with responses only are listed (i.e. if no one selected a response, it was not included in the table). 95% confidence interval was calculated using Byar’s approximation.
Current exercise habits
The most common length of OULA attendance was 4–5 years (n = 69; 24.6%, 95% CI: 19.3–30.9). The majority of the participants (n = 264; 94.3%, 95% CI: 83.4–106.2) attended the original format, OULA, and n = 156 (56.6%, 95% CI: 48.3–65.9) of the sample attended OULA 2–3 days a week, followed by n = 63 (22.4%, 95% CI: 17.4–28.5) of the participants reporting 4–5 days a week attendance. Participants were asked if they participated in other regular exercise and n = 104 (37.0%, 95% CI: 30.4–44.7) reported no. Of those who said yes, the most common selections were walking (n = 81; 46.8%, 95% CI: 37.4–57.9) and weight lifting (n = 66; 38.2%, 95% CI: 29.8–48.2). Table 2 outlines the OULA habit questions from our survey.
OULA habits.
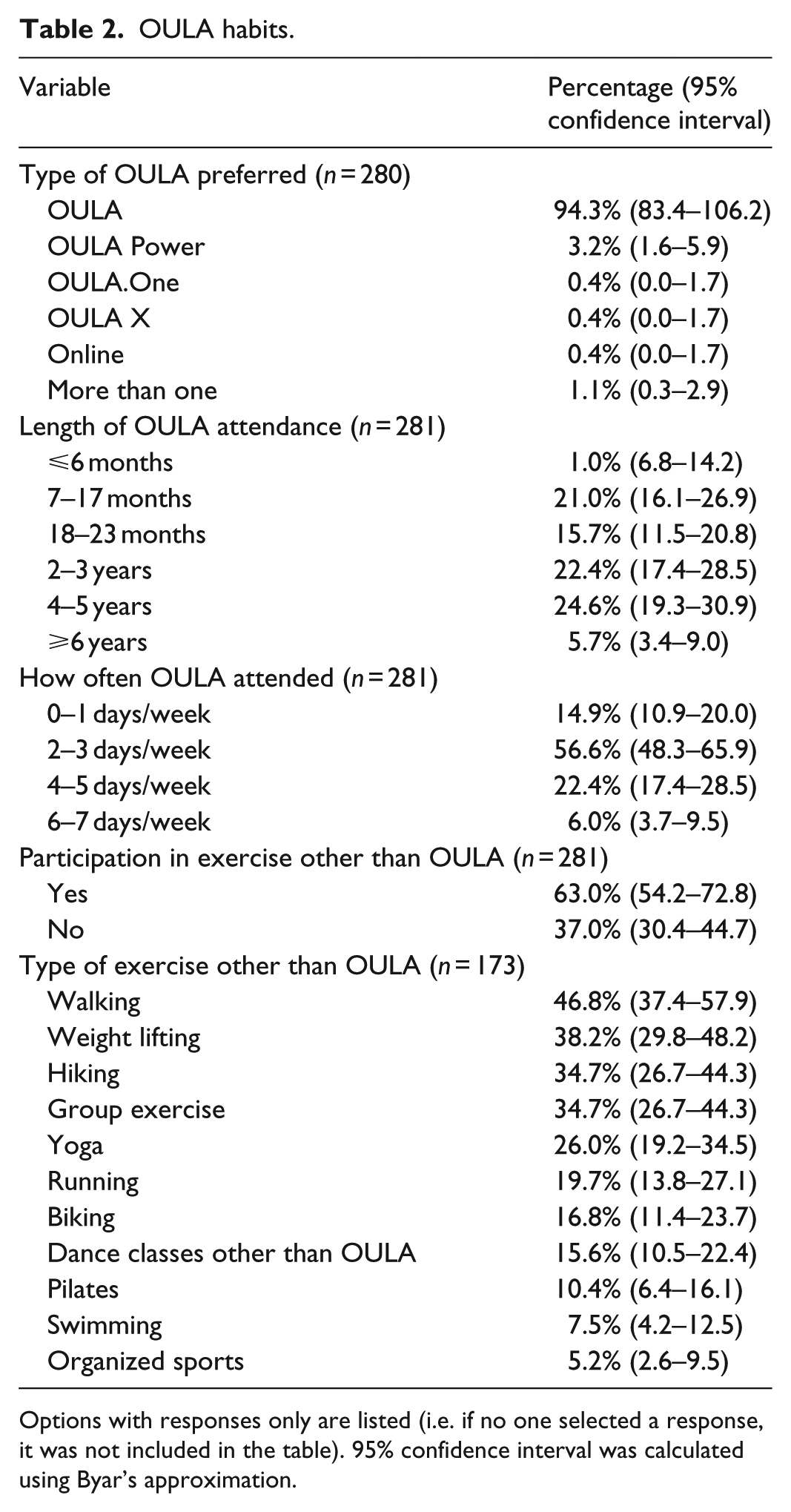
Options with responses only are listed (i.e. if no one selected a response, it was not included in the table). 95% confidence interval was calculated using Byar’s approximation.
Motivation for attending OULA
Individuals were asked to provide their primary, secondary, and tertiary reasons for attending OULA. Of the responses recorded, n = 113 (40.2%, 95% CI: 33.3–48.2) listed “exercise” as their primary reason for attending, followed by “stress relief/improve mood” (n = 81; 28.8%, 95% CI: 23.0–35.6). Participants (n = 96, 35.6%, 95% CI: 29.0–43.2) listed “stress relief/improve mood” as the most common secondary reason for attending OULA, followed by “exercise” (n = 73; 27%, 95% CI: 21.4–33.8). “Stress relief/improve mood” was also the most popular selection for tertiary reason for attending OULA (n = 102; 38.6%, 95% CI: 31.7–46.7). See Table 3 for a complete list of reasons for attending OULA.
Reasons for attending OULA.

Options with responses only are listed (i.e. if no one selected a response, it was not included in the table). 95% confidence interval was calculated using Byar’s approximation.
Potential benefits of OULA
Participants were asked if OULA makes them feel like part of a community. Of the responses recorded, n = 262 (93.2%, 95% CI: 82.5–105.1) said yes. They were also asked if OULA increases their energy outside the class and n = 225 (80.1%, 95% CI: 70.2–91.1) strongly agreed. If participants were not taking antidepressants or anxiolytics at the time of the survey, they were asked if they were able to stop taking medications after starting OULA. Of these individuals, n = 15 (6.1%, 95% CI: 3.6–9.8) were able to stop taking an antidepressant and n = 10 (3.9%, 95% CI: 2.0–6.9) were able to stop taking an anxiolytic after starting OULA. Table 4 outlines the potential benefits of participating in OULA.
Potential Benefits of OULA.

Options with responses only are listed (i.e. if no one selected a response, it was not included in the table). 95% confidence interval calculated using Byar’s approximation.
Tests of association
A Chi-square test of association was performed to examine the following relationships: age (<33 years and >33 years) and the primary reason for attending OULA, level of education and primary reason for attending OULA, length of time regularly participating in OULA (<2 years and >2 years) and the primary reason for attending OULA, and the frequency of attending OULA (<3 days per week and >3 days per week) and the primary reason for attending OULA. The only relationship that was significant was between the frequency of attending OULA and the primary reason for attending OULA χ2 (3, n = 280), 9.08, p = 0.028, Cramér’s V = 0.18. Post hoc comparisons revealed an adjusted standardized residual of 2.7 for individuals who attended OULA less than three times per week and selected exercise as their main motivation, meaning that there were more people who use OULA for exercise when attending 3 days a week or less than expected. Furthermore, an adjusted standardized residual of −2.7 was found for individuals who attended OULA more than three times per week and selected exercise as their main motivation, meaning that there were less people who use OULA for exercise when attending more than 3 days a week than expected.
Discussion
The authors report the results of what is, to the best of our knowledge, the first survey conducted on OULA participants. The primary goal of this survey was to collect data about current OULA participants’ demographics, exercise habits, motivations for attending OULA, and potential benefits from participating in the dance fitness program OULA. The 38-item survey received 302 responses with a completion rate of 93.7% (n = 282).
Participants reported “exercise” as the most common reason for attending OULA followed by “stress relief/improve mood.” They also reported “stress relief/improve mood” as the most common secondary and tertiary reason for participation. This suggests that current OULA participants are using the dance fitness program as a type of self-guided mood therapy. Our findings align with previous research that has demonstrated that exercise,41–46 dance,47–50 dance movement therapy,51–53 and Biodanza®19–22 have beneficial physical and psychological results.
Research findings have shown that exercise interventions have high attrition rates, typically ranging between 25% and 50%. 54 While our survey did not capture attrition since we targeted active OULA participants, we were surprised to learn that the majority of survey respondents attended OULA for 4–5 years. Further, predominantly, participants indicated that they attend classes two to three times a week. It has been suggested that 3 days of exercise a week can improve perceived physical fitness and physical appearance evaluation, 55 which may explain the number of frequent and loyal OULA participants. “Stress relief/improve mood” was also a common reason that was reported in this survey as motivation for attending OULA classes, and this may suggest that psychological health is a successful motivator for ongoing participation in exercise.
Intrinsic motivation (internal enjoyment of an activity) has been shown to be an incentive for performing actions due to enjoyment of the activity or identifying with its positive outcomes. 56 A study conducted on Zumba®, which is a dance exercise program similar to OULA, found that intrinsic motivation scores improved during the study because the exercise program is a fun, sustainable form of exercise for women. 57 In our survey, 18.5% (95% CI: 14.0–24.1) of participants indicated that “fun” is their primary reason for attending OULA, while 28.8% (95% CI: 23.0–35.6) listed improve mood as their primary reason. Given that mood improvement and enjoyment are documented attributes in maintaining compliance to an exercise program, 56 this demonstrates that OULA participants are motivated by mood improvement and fun. Therefore, OULA has the potential to successfully maintain exercise compliance.
In our sample, there were more respondents who participate in only OULA compared to those who engage in other forms of exercise. This may suggest that OULA provides satisfactory outcomes related to fitness, and participants do not feel the need to seek other fitness avenues. Considering that intrinsic motivation is a key factor in adherence to exercise, we believe that feeling a sense of belonging is important to an exercise program’s success. The need to belong has demonstrated that the desire for interpersonal attachment is a fundamental human motivation.27,28 In our survey, 93.2% (95% CI: 82.5–105.1) of participants indicated that OULA makes them feel like part of a community and 12.6% (95% CI: 0.9–1.7) of the participants listed “socializing/community” as their secondary reason for attending OULA. This may explain that part of OULA’s success in maintaining participants is due to the strong sense of community a person feels when active in the program.
Another factor that highlights OULA’s differences from the typically image-obsessed fitness industry and its success in maintaining participants is the low number of people who indicated “weight control” as their motivation for attendance. Only n = 4 (1.4%, 95% CI: 0.5–3.5) participants listed “weight control” as their primary reason for participating in OULA. In comparison, more participants listed “cope with grief or trauma” (n = 5; 1.8%, 95% CI: 0.7–3.9) than “weight control.” OULA encourages self-love over losing weight, which may contribute to OULA’s ability to achieve improvement in mood, socializing, and feeling like part of a community while exercising.
Survey participants were also asked if OULA gave them more energy outside of class. Of the responses recorded, n = 225 (80.1%, 95% CI: 82.5–105.1) strongly agreed that OULA gives them more energy in general, which is a key element in treating depression. Low energy or fatigue is one of the most commonly reported symptoms of major depressive disorder and these symptoms are clinically relevant for patients seeking treatment.58,59 In our survey, we asked participants about their experience with depression and anxiety, assessing if people are using OULA as a treatment without clinician guidance. Participants were asked if they were currently taking antidepressants or anxiolytics at the time of the survey. Of the responses recorded, 12.5% (95% CI: 8.8–17.1) indicated that they were currently taking antidepressants and 8.9% (95% CI: 5.9–12.9) were taking anxiolytics. If participants indicated that they were not currently taking one or both, they were asked if they had previously been taking either and stopped taking one or both after starting regular OULA attendance. Of these responses recorded, 6.1% (95% CI: 3.6–9.8) said they were able to stop taking an antidepressant after starting OULA and 3.9% (95% CI: 2.0–6.9) said they were able to stop taking an anxiolytic. This may suggest that OULA has the potential to replace or augment pharmaceutical options with a natural, non-pharmacological approach to treating mood disorders and anxiety.
Compared to the number of respondents who enter OULA for stress relief/improve mood, it is possible that OULA is effective for approximately one third of the sample based on the number of respondents who discontinued an antidepressant or anxiolytic after starting OULA. These numbers should be interpreted very cautiously, though, because the sample size is low, and we did not ask adequate question to investigate if respondents ceased antidepressants or anxiolytics due to OULA or if there were other reasons for termination. Further research with respect to OULA providing depression or anxiety symptom relief is warranted.
Finally, tests of association revealed no association between demographic characteristics and the main reason for attending OULA except for a significant finding between the number of days attending OULA and exercise as the primary reason for attending. This finding shows that individuals who attend OULA less than 3 days per week attend for exercise, whereas individuals who attend more than three times per week attend for reasons other than exercise. Considering that regular exercise is known to promote mental health 60 and that stress relief/improve mood was the second most common reason for attending OULA, this finding is not too surprising. However, even though exercise is well known to improve mental health, some research suggests that mental illness, like depression61–63 and anxiety,64,65 is a barrier to exercise or physical activity. Perhaps, the collective unique features of OULA, for example, community aspect, physical activity, less focus on physical appearance, and emotional processing through song and dance, explain why individuals who join OULA more than 3 days a week attend for reasons other than exercise.
Limitations
Our study has limitations that merit consideration. First, our sample was homogeneous with respect to gender, race, marital status, geographic location, and education level, limiting the generalizability of findings. Second, given the nature of our study design, a pilot, descriptive cross-sectional study via an Internet-based survey, there is uncertainty about the validity of the responses. Furthermore, this design poses sampling issues, as it is possible that we did not reach some OULA participants who are not computer savvy or do not have access to a computer. Our sampling timeframe was also limited to only 3 months. We posted the link to the survey every 2–3 weeks on social media and reminded OULA instructors to continue to announce the survey availability until there were no further responses for 3 weeks. Future Internet-based surveys of OULA might consider a longer sampling timeframe to maximize the number of respondents, as well as a comparison group with data collected in specific settings where the number of respondents could be counted, and the differences between a systematic search of responders and the general Internet survey could be measured. Also, even though weight loss was not a common selection for a reason to attend OULA, we failed to consider body mass index (BMI) as a variable. The inclusion of BMI would have allowed us to evaluate an association between BMI and motivation for OULA participation.
As a final limitation to our study, while we inquired about participants terminating antidepressants or anxiolytics after initiating OULA, we did not query if the reason that antidepressants or anxiolytics were discontinued was because of OULA participation. Our finding of 6.1% (95% CI: 3.6–9.8) or 3.9% (95% CI: 2.0–6.9) of respondents discontinuing an antidepressant or anxiolytic, respectively, after starting OULA should be interpreted cautiously. Further investigation with a well-designed study should be conducted to better understand the relationship between abating antidepressants or anxiolytics with OULA attendance.
Conclusion
In conclusion, OULA is a relatively new form of dance fitness that is available to a variety of skill levels. OULA participants appear to be committed to attending OULA regularly (i.e. two to three times per week) primarily for exercise and to improve mood for an average duration of 4–5 years. Given the documented benefits of both exercise and dance on physical and psychological well-being, healthcare professionals might consider recommending OULA participation to patients seeking a new form of exercise that has a strong community focus. Utilizing OULA as a complementary and alternative modality to managing depression and anxiety should be further explored before it is recommended. However, it is unlikely that dancing and singing in a group fitness setting would cause harm to patients with depression and anxiety.
Footnotes
Appendix 1
My name is Tracy Hellem, PhD, and I am an Assistant Professor at the College of Nursing at Montana State University. My research interests are focused on exploring novel treatments for mood symptoms, specifically among women. I am conducting a survey to learn more about why people attend OULA and the potential benefits of it. The long-term goal of this is to study OULA as an intervention for mood symptoms. My colleague, Hayden Ferguson, is helping with the survey. Participation is voluntary, you can stop at any time, and you can choose to not answer any questions you do not want to answer. The data from the survey will be used in a publication that describes the results of the survey. By entering the survey, you provide your informed consent to participate in this study and for your anonymous data to be used in a publication. Thank you for taking our survey.
What is your age?
What gender do you identify most closely with?
Choose one or more races that you consider yourself to be:
Are you Spanish, Hispanic, or Latino or none of these?
Are you Spanish, Hispanic, or Latino?
What is your relationship status?
What is the highest level of school you have completed or the highest degree you have received?
Where do you live?
How long have you been attending OULA regularly?
Which OULA class do you attend MOST often?
How often do you attend OULA in an average week?
What is the primary reason you attend OULA? Please choose one.
What type of grief are you coping with through OULA?
What type of pain are you experiencing that OULA helps alleviate?
What type of trauma are you coping with through OULA?
Are there other reasons you attend OULA?
What is the secondary reason you attend OULA? Please choose one, not the same answer as your primary reason for attending OULA.
What type of grief are you coping with through OULA?
What type of pain are you experiencing that OULA helps alleviate?
What type of trauma are you coping with through OULA?
Is there another reason you attend OULA?
What is the third reason you attend OULA? Please choose one, not the same answer as your primary or secondary reason for attending OULA.
What type of grief are you coping with through OULA?
What type of pain are you experiencing that OULA helps alleviate?
What type of trauma are you coping with through OULA?
Do you have a regular exercise routine other than OULA?
What kind of exercise do you regularly do outside of OULA? (Choose all that apply)
Does OULA help you feel like you are a part of a community?
Does OULA increase your overall energy?
Do you currently take medication for depression?
Which medication(s) are you taking for depression?
Were you taking any medication for depression when you started OULA that you are no longer taking?
What medication(s) for depression were you taking when you started OULA?
How long after starting OULA did you stop taking medication for depression?
Do you currently take medication for anxiety?
What medication(s) for anxiety are you currently taking?
Were you taking medication for anxiety when you started OULA that you are no longer taking?
What medication(s) for anxiety were you taking when you started OULA that you are no longer taking?
Acknowledgements
We acknowledge Kali Lindner and Laura Hildreth for their support and contribution to this work. Ms Lindner provided feedback on survey questions, in addition to distributing the Qualtrics URL. Dr Hildreth provided statistical consultation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
For IRB study no. #TH072816-EX, Montana State University Institutional Review Board issued an exemption in accordance with the Code of Federal Regulations, part 46, section 101.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T.H. received funding from The College of Nursing and Office of Research and Economic Development at Montana State University to support this project.
Informed consent
A consent paragraph was included as an introduction to the survey. Participants provided consent by entering the survey after reading the consent paragraph. In this paragraph, participants were notified that the survey was anonymous and voluntary and that they could stop at any time and choose not to answer the questions. They were also informed that the results of the survey would be used in a publication.