
Abstract
Backgrounds:
Beauty standards vary across cultures and regions. To date, no research has identified ideal nasal profiles for Thai individuals. This study aims to determine the preferred nasal aesthetics among the Thai population.
Methods:
This cross-sectional study employed an online self-assessment questionnaire to investigate the ideal nasal profiles among Thai adults aged 18–60. Data were collected from participants across all regions of Thailand and included demographic information, rhinoplasty intentions, and perceptions of ideal nasal features.
Results:
Of the 1452 respondents, 35.74% (519 individuals) have either undergone or plan to undergo rhinoplasty, while the remaining 64.26% (933 individuals) expressed either no interest or uncertainty about the procedure. The ideal nasolabial angle was found to be between 97 and 108 degrees for males and 88 to 98 degrees for females, respectively. Male participants in the rhinoplasty and control groups exhibited statistically significant differences in nasolabial angle (p = 0.017), nasofrontal angle (p < 0.001), and alar-intercanthal distance ratio (p < 0.001). Female participants demonstrated statistically significant differences between groups in nasofacial angle (p < 0.001) and nasolabial angle (p < 0.001).
Conclusions:
Our study identified distinct ideal nasal profiles among the Thai general population and those considering rhinoplasty. Our findings differed from the neoclassical orbitonasal proportion (canon V). These findings offer insights into contemporary Thai beauty standards for the nose, which can inform clinical decision-making in nasal treatment.
Introduction
Rhinoplasty is a surgical procedure aimed at altering and reconstructing the nose. This procedure encompasses both reconstructive surgery, which restores the form and function of the nose following trauma or congenital defects, and cosmetic surgery, which focuses solely on enhancing the aesthetic appearance of the nose. The intent of functional rhinoplasty is to improve nasal airflow (and the perception thereof) by surgically correcting the anatomical sources of obstruction in the nasal airway. 1 According to the systematic review, functional rhinoplasty may have a positive effect on nasal obstruction caused by nasal valve problems 2 and improve quality of life of patients. 3
Globally, the procedure has become increasingly popular as an aesthetic enhancement. 4 For optimal aesthetic rhinoplasty results, patients should discuss their goals, concerns, and expectations with their surgeon, including potential complications and the desired nasal shape.5,6
Given the cultural and regional diversity of beauty standards, research focused on specific populations is essential. A study involving 150 Caucasian males identified an idealized silhouette nasofrontal angle range of 106–148 degrees. Angles outside this range were perceived as less attractive, with those beyond 118–145 degrees considered highly unattractive. 7
Ideal nasal aesthetics have also evolved over time. A study revealed that younger generations, including Gen Z and Millennials in their 20s and 30s, favor a more pronounced radix. While Gen Z, Millennials in their 20s, and Gen X preferred a 90-degree nasolabial angle, Millennials in their 30s leaned toward a 100-degree angle. 8
A 2024 cross-sectional study of 197 individuals from Canada, Saudi Arabia, Kuwait, and Lebanon revealed mean ideal nasolabial angles of 97.1 ± 6.39 degrees for males and 109.5 ± 5.32 degrees for females. 9
Identifying the ideal nasal profile is crucial for establishing patient-centered aesthetic goals. While numerous studies have delineated ideal nasal profiles across different countries, a corresponding profile for the Thai population remains elusive.7,10,11
This study aimed to find ideal nasal profiles including nasofacial angle, nasolabial angle, nasofrontal angle, and alar-intercanthal distance ratio in the Thai population.
Materials and methods
Study design and setting
A cross-sectional study during December 2020 and May 2021 in Thailand.
Participants
Inclusion criteria
Thai participants aged 18–60 with sufficient literacy to complete the self-assessment questionnaire were included in the study. The “rhinoplasty group” consists of participants who have undergone or plan to undergo rhinoplasty. The “control group” comprises participants who have no interest in rhinoplasty.
Participant recruitment
Participants completed a self-assessment questionnaire, available in both online and paper versions. An online questionnaire, created and distributed via Google Forms, was publicized at 21 faculties of Khon Kaen University (8 preclinic, 13 clinic), 11 medical university in Thailand, and 4 rhinoplasty clinics (3 in Khon Kaen, 1 in Bangkok). Additionally, paper questionnaires were collected from patients in the outpatient department of Otorhinolaryngology at Khon Kaen University’s Faculty of Medicine.
Exclusion criteria
Participants who failed to answer all required questions or provided incorrect responses to test questions were excluded. These test questions verified participants’ ability to view images in the electronic format and comprehend the rating scale.
The questionnaire instructions included guidance on identifying angles and facial features on the model, as well as instructions for answering the questions. A few practice questions were provided to ensure understanding. Responses were considered “incorrect” if they did not match the correct answers.
• Example of guidance: The nasolabial angle, measured between the lower edge of the nose and the upper lip, was 35 degrees in this model.
• Example of guidance: In this model, you can see the example includes an example marking indicating the preferred nasolabial angle, which is 27.5 degrees.
• Example of question: Do you understand how to use the markings?
• Example of answer: I understand.
• Example of question: We will provide a model with markings indicating the preferred angle and ask you to identify the exact angle.
• Example of answer: 37 degrees.
Model creation
A Canon 760D camera was used to photograph the model, capturing images with a 3472 * 2320 (3:2) aspect ratio. The camera was positioned directly in front of the model’s nose, ensuring a perpendicular angle.
The frontal and lateral facial images in the photographs were symmetrical in terms of eyebrows, eyes, nose tip, and lips, as demonstrated in the sample image. This symmetry ensures accurate and precise simulation of the nose in various shapes and angles. Written consent was obtained from both male and female models (Figure 1).
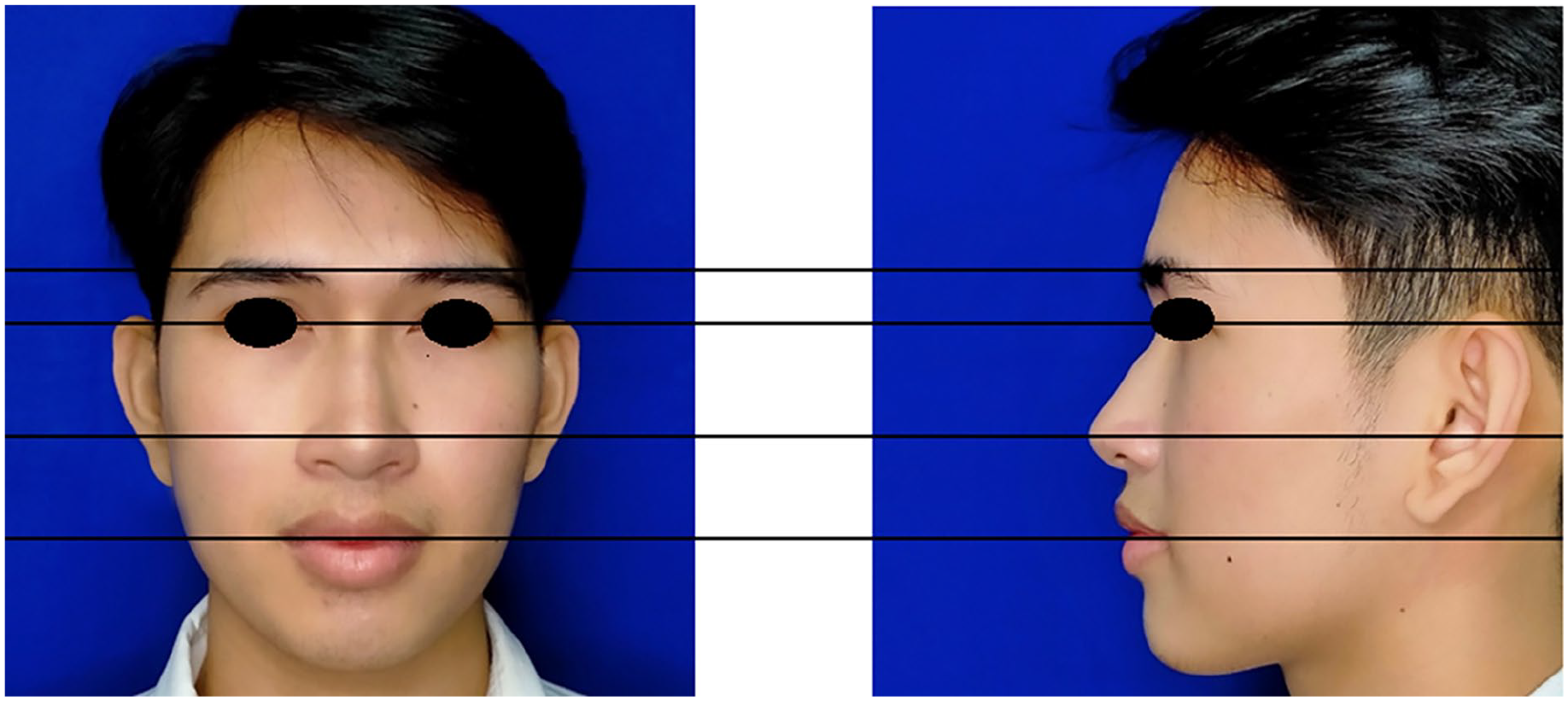
Model creation.
The frontal and lateral facial images were cropped to a 913 * 913 (1:1) aspect ratio using Adobe Photoshop. Subsequently, image editing tools were employed to create simulated noses in various shapes and angles based on ideal values as shown in Table 1.
Angles and ratios for female and male models.

The following steps outline the process utilized for creating a simulated nose image, leveraging specific tools within Adobe Photoshop.
1. Determination of nose angle and size: The manipulation process begins by identifying the appropriate angle or size of the nose image as described in Table 1.
2. Selection of the target area using the lasso tool (Adobe Inc., CA, USA): To isolate the specific region of the image for alteration, the “Lasso Tool” was employed. This tool enables the precise selection of the area surrounding the nose, facilitating focused modifications.
3. Defining the selection boundary: The Lasso Tool (Adobe Inc., CA, USA) was used to trace the outline of the nose. This step ensures that only the region designated for modification is selected, thereby preserving the integrity of the rest of the image.
4. Copying the selected region: Once the nose area was successfully selected, it was copied to create an isolated image layer. This duplication allows for independent manipulation of the nose image without affecting the original.
5. Application of the puppet warp tool: The “Puppet Warp Tool” was subsequently applied to the isolated nose image. This tool provides the ability to manipulate the shape of an object through the placement of control points, referred to as “pins,” at strategic locations.
6. Adjustment of the image using pin placement: Pins were positioned around the nose image, serving as anchor points that enable controlled adjustments. By repositioning these pins, the image was altered to achieve the desired proportional and angular adjustments, as specified by the initial calculated values.
7. Finalization of image manipulation: Upon completing the necessary adjustments, the nose image was finalized to match the predetermined specifications. This concluded the manipulation process, resulting in the desired shape and orientation.
Outcomes
Demographic data
Gender, age group, education, occupation, income, marital status, religion, and region were collected.
Reason for rhinoplasty
To identify participants interested in rhinoplasty, respondents were queried about their motivations for considering the procedure, their awareness of potential postoperative complications, and their preferred surgical technique.
Control group participants were queried about their reasons for not considering rhinoplasty and their knowledge of potential postoperative complications.
Ideal nasal profiles
Computer-manipulated lateral and frontal view photographs of Thai female and male nasal profiles were generated. Five keyframe continua, evenly spaced and centered around Caucasian ideal nasal profiles, were created. Participants selected their preferred profile by marking a numeric rating scale below the images (Figure 2).

Example of questionnaire of Thai female nasal profiles with numeric rating scale.
To ensure the validity of the questionnaire, it was evaluated by a panel of 5 otorhinolaryngology experts and pilot-tested with 30 participants. The questionnaire was revised iteratively until consensus was reached among the experts and no further comments were raised.
In the lateral view, the participants will rate:
Nasofacial angle—the incline of the nasal dorsum in relationship to the facial plane. It is formed by a vertical line tangent to the glabella and tangent to the pogonion intersecting with the line tangent to the nasal dorsum.
Nasolabial angle—the angle between the inferior border of the nose and the labial surface of the upper lip.
Nasofrontal angle—the angle between a line tangent to the glabella through the nasion and intersecting with the line tangent to the nasal dorsum.
In the front view, the participants will rate:
Alar/intercanthal distance ratio—the ratio of the distance between the outermost point of alar bases at the junction of the alar base and lip with the distance between the medial canthi of eyes.
Statistical analysis
The sample size calculation was based on a hypothesized difference in nasofacial angle of 0.33 degrees between the rhinoplasty and normal populations, 12 with a significance level of 0.05 and a power of 90%, the estimated sample size required for each group is 1477. This calculation suggests that a total of 2954 participants (1477 in the rhinoplasty group and 1477 in the control group) would be necessary to detect a statistically significant difference between the two groups, assuming the hypothesized difference is true.
Statistical analyses were performed using the SPSS version 20 (International Business Machines Corporation, NY, USA). Data were described as either means (for the continuous variables) or frequencies and percentages (for the categorical variables). Significant differences between groups were determined using the student t-test or the Mann–Whitney U test for continuous variables. The Chi-square test or the Fisher exact test was used to determine whether there was a significant difference between the expected frequencies and the observed frequencies. For all tests, p < 0.05 was considered statistically significant.
Results
A total of 2028 participants completed the questionnaire. After excluding 576 responses due to missing data or invalid answers, 1452 responses were analyzed. Of these, 519 participants have either undergone or plan to undergo rhinoplasty (rhinoplasty group), while 933 indicated no interest or uncertainty about the procedure (control group). When comparing the rhinoplasty and control groups, we observed demographic disparities. Individuals in the rhinoplasty group exhibited lower educational attainment (p < 0.001). They were also more likely to be resided primarily in the Central, Northeast, or North of Thailand (p < 0.05). Demographic data for both groups are summarized in Table 2.
Demographic data.

Statistically significant.
The mean and standard deviation of ideal nasal profiles in both rhinoplasty group and control group were presented in Table 3. Statistically significant differences in nasal angles were observed between the two groups. Females exhibited differences in nasofacial and nasolabial angles (p < 0.05), while males showed differences in nasolabial angle, nasofrontal angle, and alar-intercanthal distance ratio (p < 0.05).
Ideal nasal profiles.

Statistical significance.
The rhinoplasty group primarily sought the procedure for aesthetic enhancement (76.69%) and increased self-confidence (72.25%). Most participants demonstrated awareness of potential complications, with silicone implantation being the preferred surgical method (61.08%). Detailed findings are presented in Table 4.
Attitude and knowledge in rhinoplasty group.

The control group primarily cited satisfaction with their current nasal appearance (52.66%) and fear of surgery (40.84%) as reasons for not considering rhinoplasty. Moreover, most participants in this group demonstrated knowledge of potential postoperative complications. Detailed results are presented in Table 5.
Attitude and knowledge in control group.

Discussion
Nasal profiles are integral to facial aesthetics. While numerous studies have explored ideal nasal aesthetics, including anatomical features, gender-specific preferences, cultural influences, and temporal variations, a corresponding dataset specific to the Thai population remains absent.7,13
Western studies have contributed significantly to our understanding of ideal nasal aesthetics. Sinno et al.’s 14 Canadian study on 98 volunteers determined the most aesthetically pleasing nasolabial angle to be 104.9 ± 4.0 degrees for females and 97.0 ± 6.3 degrees for males.
Research from Iran involving 70 participants highlighted the importance of nasolabial angle (p < 0.001) and nasofacial angle (p = 0.028) in overall facial beauty, suggesting that less prominent noses with higher tips enhance profile aesthetics. 15
Additionally, Milutinovic et al.’s 16 2014 Serbian study compared facial proportions of 24 attractive females to 83 anonymous controls. Attractive females exhibited facial symmetry, including an alar-intercanthal ratio approximating 1, aligning with established aesthetic ideals.
Asian populations exhibit distinct facial characteristics. Choi et al. highlighted the influence of increased upper lip protrusion on nasolabial angle differences between Asians and Caucasians. 17 Wang et al.’s 18 comparison of Chinese and North American Caucasians revealed a closer approximation of ideal alar-intercanthal distance ratios among Chinese individuals.
There was no ideal nasal profile study in Thailand. A Thai baseline anatomical study examining 240 adults aged 18–35 revealed nasolabial angle ranges of 86.4–105.76 degrees for females and 78.05–104.71 degrees for males. Nasofrontal angles were 127.51–140.67 degrees in females and 121.38–135.76 degrees in males. The alar-intercanthal distance ratio was 1.15 for females and 1.16 for males. 19
Burusapat and Lekdaeng 20 retrospectively reviewed the photographs of Miss Universe Thailand and Miss Universe from 2001 to 2015 and compared them with neoclassical canons and the facial golden ratio. The study revealed that the modern facial proportion of beauty demonstrated a wider alar/intercanthal distance ratio, and the ratio was wider when comparing Miss Universe Thailand to Miss Universe.
In this study, the control group demonstrated ideal nasolabial angles of 102.47 ± 5.30 degrees and 93.56 ± 5.86 degrees for females and males, respectively. Nasofrontal angles were 126.62 ± 4.23 degrees for females and 126.09 ± 4.15 degrees for males. Alar-intercanthal distance ratios were 1.05 ± 0.10 for females and 1.10 ± 0.11 for males, aligning with previous research on normal ranges.
This finding was consistent with a Chinese study that identified a preferred nasolabial angle of 106 degrees for both men and women. 21 The study in Iranian population also found the consistent preference for nasofrontal angles were 137.64 ± 4.20 degrees for males and 133.55 ± 4.53 degrees for females. The most preferred nasolabial angles were 107.56 ± 5.20 degrees and 98.92 ± 4.88 degrees, respectively. 22
When compared to Neoclassical Nasal Canons, Neoclassical Canon V stipulates that nasal width should equal intercanthal distance. However, our study found alar-intercanthal distance ratios of 1.05 ± 0.10 for females and 1.10 ± 0.11 for males in the Thai population. This suggests a preference for nasal width to be slightly greater than intercanthal distance. Our findings align with numerous studies demonstrating that Neoclassical Nasal Canons may not be universally applicable to contemporary aesthetic preferences.23,24
For the patients who underwent rhinoplasty in Thailand, one study found the average profiles of the rhinoplasty nose were significantly higher nasofrontal angle and alar/intercanthal distance ratio when compared with ideal nasal profiles. 25
In this study, female rhinoplasty candidates exhibited significantly larger nasofacial and nasolabial angles compared to the control group (p < 0.05). Male rhinoplasty candidates displayed significantly larger nasolabial and nasofrontal angles, as well as a smaller alar-intercanthal distance ratio (p < 0.05).
Individuals considering rhinoplasty should be fully informed about potential complications. A study by Arabi Mianroodi et al. 26 on Iranian high school girls revealed that while 53.65% expressed interest in rhinoplasty, many lacked awareness of common complications such as skin discoloration (89.44%) and nasal obstruction (75.15%).
The study assessed participants’ awareness of rhinoplasty complications. While most participants were knowledgeable about common complications, skin discoloration was a notable exception.
When comparing the rhinoplasty and control groups, we observed demographic disparities. Individuals in the rhinoplasty group exhibited lower educational attainment (p < 0.001). They were also more likely to be resided primarily in the Central, Northeast, or North of Thailand (p < 0.05).
Unlike previous studies that limited their focus to the nasofrontal 7 or nasolabial angle,9,17 our study comprehensively evaluated all four angles: nasofacial, nasolabial, nasofrontal, and alar width per intercanthal distance.
Previous studies investigating multiple nasolabial ratios have typically involved smaller sample sizes, ranging from 66 to 1417 participants.7,10,13,14,16 In contrast, our study aimed to recruit a larger sample of 2954 Thai individuals using purposive sampling from various regions. Despite this ambitious goal, the final sample consisted of 2028 participants, with 519 in the rhinoplasty group and 933 in the control group after applying exclusion criteria.
However, a limitation was the uneven distribution of participants across regions, with lower response rates in northern and southern Thailand. This could potentially impact the generalizability of the findings. The reliance on self-assessment and perception-based data can limit the objectivity of research, potentially overlooking nuanced preferences for nasal aesthetics.
To our knowledge, this is the first large-scale study of ideal nasal profiles in Thailand. The findings can empower surgeons to enhance patient satisfaction by incorporating these data into preoperative consultations. Future studies should investigate how demographic factors—such as sex, age, education, income, region, and marital status—affect participants’ preferences for the ideal nasal profile.
Conclusions
Our study identified distinct ideal nasal profiles among the Thai general population and those considering rhinoplasty. Our findings differed from the neoclassical orbitonasal proportion (canon V). These findings offer insights into contemporary Thai beauty standards for the nose, which can inform clinical decision-making in nasal treatment.
Footnotes
Acknowledgements
The authors would like to thank the Center of Cleft Lip-Cleft Palate and Craniofacial Deformities, Khon Kaen University under Tawanchai Royal Grant Project for their support.
Author contributions
CK conceptualized, designed, raised funding for the study, performed data analysis, interpreted results, and first drafted the article. SS, WR, SC, and PK contributed to designed, supervised, and revised the article. KK contributed to the computerized image and revise the article. PP conceptualized, designed, supervised, performed data analysis, interpreted results, and major contribution to the article. All authors contributed to the interpretation and discussion of the results, read, and approved the final article.
Data availability statement
Due to ethical reasons and patients’ confidentiality, the datasets for this study can be requested from the corresponding author with an appropriate reason.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received an internal funding from the Faculty of Medicine, Khon Kaen University (Grant Number IN64114).
Ethics approval
Ethical approval for this study was obtained from the Khon Kaen University Ethics Committee in Human Research (Approval Number: HE631454).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.