
Abstract
Background:
Food aversion is one of the reasons for maternal undernutrition. Early screening for maternal undernutrition risk factors would improve the ability to recognize this problem and intervene early. Hence, this study was intended to identify the association of food aversion with maternal nutritional status.
Objectives:
To assess food aversion and its association with pregnant women’s nutritional status in Teticha Woreda, Sidama region, Ethiopia, March, 2022.
Methods:
In Teticha Woreda, a mixed community-based comparative cross-sectional study was carried out from 1 March to 15 April 2022. Data were collected using an unstructured interview guide for qualitative data and a structured questionnaire for quantitative data. Epi-Data version 3.1 was used to enter quantitative data. Quantitative data were exported and cleaned and analyzed in SPSS version 20. For the quantitative data, descriptive statistics were calculated. To identify predictors of low nutritional status and control for confounders, multivariable logistic regression was utilized. Using Pearson’s Chi-square test, the association between food aversion and the anthropometric status of pregnant women was examined.
Results:
Maternal undernutrition was found in 109 (48.9%; 95% CI: 42.4%–55.4%) of pregnant women with food aversion and 69 (30.9%; 95% CI: 25.1%–37.2%) women without food aversion (mid-upper arm circumference 23 cm). A significant proportion of mothers 95 (42.6%) stated that food aversion stemmed from the taste or smell of the food. Some mothers avoided “Enset,” while others avoided foods like cereal, milk, and coffee. In the Chi-square test, pregnant women who had food aversion had a higher likelihood of maternal undernutrition as compared to women who did not have food aversion (p-value of 0.000).
Conclusion:
This study found higher magnitude of undernutrition among pregnant women who had food aversion as compared to their counterparts. Nutritional interventions, especially nutritional counseling focusing on food aversion, are essential to tackle maternal undernutrition.
Background
Unfavorable influences in the environment, including insufficient nutrition, inadequate health care, and poor education, are disproportionally affecting women. Often, women are most vulnerable to poor nutritional status. 1 Food aversion is one of the factors that affect the food intake and nutritional status during pregnancy. It is strong dislike of a particular food during pregnancy. It is one of the risk factors for maternal undernutrition. 2 For example, aversion to vegetables, a good source of micronutrients like folic acid, during pregnancy may affect both the mother and the developing fetus health status. 3 In addition to food aversion, the available evidences reveled that age, educational status, husband’s education, family size, meal frequency, skipping meals, food taboos, trimester, antenatal care (ANC) follow-up, parity, nausea and vomiting, and nutritional counseling during ANC visit are risk factors for undernutrition during pregnancy.4–8
The level of the food averted varies depending on the geographical area and may be influenced by cultural, ethnic, and/or socioeconomic factors. For example, 71% of women in a study on Yasawa Island, Fiji, 44.8% of women in Ghana, 70.1% of women in Tanzania, and 48.7% of women in Kenya reported food aversion during pregnancy.7,9–11 Even though it is a common and well-known phenomenon, few studies have been conducted in Ethiopia; a study conducted in Boricha, Sidama reported significant proportion (69.2%) of pregnant mothers averted at least one food item in their pregnancies time. 12
Target 2.2 of the Sustainable Development Goals aims to eradicate all types of malnutrition, acknowledging the potential risk of undernutrition. It addresses the nutritional needs of teenage girls, pregnant mothers, and lactating women. It is the internationally agreed target on stunting and wasting in children under the age of five. 13 Additionally, Ethiopia’s government is committed to enhancing nutrition. The goal of the National Nutrition Program’s second phase (NNP II, 2016–2020) was to address malnutrition during the 1000 days that span from pregnancy to the first 2 years of life. One of the program’s objectives is to help women who are pregnant or breastfeeding eat better by providing them with regular, thorough nutritional examinations and counseling. 14
Our goal was to find out how pregnant women’ nutritional status and food aversion are associated. Thus, there was not much evidence available in the research area about the relationship between food aversion and the nutritional status of pregnant mothers. In addition, we employed a mixed comparative cross-sectional study methodology, which distinguishes us apart from earlier research conducted in the subject area.13,14 When it comes to tackling the problem of maternal undernutrition, a study design like this one deepens our understanding of the association between food aversions and a pregnant mother’s nutritional status. Thus, in Teticha Woreda, Sidama Region, Ethiopia, in 2022, the current mixed comparative cross-sectional study sought to ascertain the association between food aversion and nutritional status of pregnant women as well as to investigate community opinions regarding food aversion.
Methods and materials
Study area
This research was carried out in March 2022 in the Teticha Woreda, Sidama region of Ethiopia. The Teticha Woreda has a “dega” (Cool Zone) climate, is located 361 km from Addis Ababa, the country’s capital, and is 88 km from Hawassa, the regional capital. The population projection for 2022–2023 is 79,559, with 39,540 women and 40,019 men, according to data from the Teticha district health office. According to information from the Teticha district health office, there are 15 kebeles overall in the Woreda—1 urban and 15 rural. In the district, there were projected to be 2753 pregnant women during the Ethiopian fiscal year 2014 E.C. There are two government health centers, fifteen health posts, and one non-governmental clinic in the district. The 2013 E.C annual report showed that 89% of women received ANC4 and 105% of women received first prenatal care (ANC1). “Enset,” cabbage, and maize are the district’s major foods. 13
Design and duration of the study
A mixed community-based comparative cross-sectional study supplemented by qualitative approach was used. The study was carried out between 1 March and 15 April 2022.
Population
The study’s source population consisted of all Teticha Woreda pregnant women. The study population consisted of pregnant women who resided in the kebeles that were chosen at random. This study covered all pregnant women who appeared healthy and lived longer than 6 months in Teticha Woreda. Excluded from the study were pregnant women with acute infectious disorders such as typhoid fever, typhus, malaria, and HIV/AIDS as well as chronic diseases like tuberculosis.
Sample size determination and sampling procedure
For quantitative study
The Epi Info7 StatCalc program was used to determine the sample size for double population proportions. Assuming a 1:1 ratio between the study and reference groups, a 95% confidence interval (CI), a 5% margin of error, and 80% power of the study, the proportion of pregnant women in the reference group and among pregnant women with food aversion who were in poor nutritional condition was 26% and 38.4%, respectively. 13 After applying a 10% non-response rate and applying finite correction, it eventually generated a total sample size of 446 (223 with food aversion and 223 without food aversion).
For qualitative study
In-depth interviews and key informant interviews were carried out in Loya Kebele to supplement the quantitative data. Eight pregnant women participated in the in-depth interviews, and six mothers-in-law took part in the key informant interviews. The quantitative section did not include women or mothers-in-law who were part of the qualitative component.
Sampling procedure
For quantitative study
Conveniently, Teticha Woreda was chosen. Pregnant women were chosen using a multi-stage sampling approach. First, a lottery method was used to randomly select five rural kebles out of sixteen kebeles. Second, a probability proportion to size (PPS) allocation technique was employed to determine the number of pregnant women from the chosen kebeles included in the study. This was done based on the ANC yearly plan from kebeles.

The actual study participants were chosen using systematic sampling techniques. The following formula was used to determine the sample fraction (K):
K = N/n Where N = 1008, n = 446; K = 1008/446 = 2.
The initial number—two—was then chosen as the starting point using the Simple Random Sampling approach. Ultimately, starting with number two, every second pregnant woman gave the actual data.
For qualitative study
For the qualitative method, study participants were chosen through the use of purposeful sampling.
Variables of the study
Dependent variable (outcome)
Nutritional status (mid-upper arm circumference (MUAC) < 23.0 cm undernourished, MUAC 23.0 cm > well-nourished).
Independent variable
Sociodemographic characteristics (age, religion, education, husband’s educational status, occupational status, and family size).
Maternal health characteristics (food aversion, pregnancy type (intentional or unintentional), ANC attendance, nutritional counseling during ANC visit, pregnancy trimester, parity, iron supplementation, morning sickness and pica during pregnancy, knowledge of pregnancy danger signs, and previous pregnancy outcomes).
Cultural characteristics (food taboos).
Meal pattern (number of meals per day, additional meals, and skipping meals).
Operational definitions
Food aversion: Strong dislikes and ignorance of specific food items during pregnancy. 15
Food taboos: Social or religious prohibitions or restrictions on certain foods.
Nutritional status: Pregnant women with MUAC < 23.0 cm are undernourished, while pregnant women with MUAC ⩾ 23.0 cm are well-nourished. 12
Procedures and tools for data collection
For quantitative data
Data were gathered via interviewer administer questionnaire. Six diploma-holding nurses were recruited in order to gather data. A health officer who was proficient in both Sidamic and Amharic worked as a supervisor during the data collection phase.
For qualitative data
An interview guide with open-ended questions was created in English, translated into Sidamigna, and then back into English. The information was gathered from pregnant women and mothers-in-law of daughters-in-law who had delivered children or were pregnant. The interviews were took place in the participants home. The investigators, who have qualitative research experiences, carried out all in-depth and key informant interviews, which took between 35 and 60 min. Recordings of the interviews were made. In addition to recording the interviews field notes were used.
Data quality management
A pretest was conducted on a quantitative data collecting questionnaire to assess its accuracy in responses, language clarity, suitability of data collection equipment, time estimation, and necessary revisions to take into account before the real data collection. It was done on 5% of non-study participants who fulfilled the inclusion criteria 1 week before to the real data collection period in Titecha town.
Furthermore, the data collectors and supervisor received 2 days of training on data collection technique. The significance of informing study participants of the study’s potential benefits and purpose prior to the commencement of data collection was also covered in the training. Keeping participants’ privacy private during the entire data collection procedure was also covered and determined during the training.
Every day, the data collection process was supervised by a trained supervisor. Also, the researcher checked for completeness and consistency of questionnaires filled out by the data collectors to ensure the quality of the data. The data quality of the qualitative study was assured by the careful selection of key informants with the help of the health extension workers who were working in the selected kebeles. Moreover, the tapes were transcribed word for word.
Data analysis
For quantitative data
After data collection, the completed data were entered into the statistical software Epidata Version 3.1 and then exported to SPSS Version 20.0 for analysis and cleaning. Descriptive statistics, frequency distribution, measures of variability, and central tendency were computed. Pearson’s Chi-square test at 95% CI was used to determine the association between food aversion and pregnant women’s anthropometric status; a p-value less than or equal to 0.05 was used to declare significant association. Multivariable logistic regression was used to identify predictors of undernutritional status and control for confounding variables. A statistically significant association was defined as one with a p-value of less than 0.05. Strength of association was measured by adjusted odds ratio (AOR) with a 95% CI. Using the Hosmer and Lemeshow tests, the model’s goodness of fit was determined. The variance inflation factor was used to assess predictor variables for multicollinearity.
For qualitative data
To analyze the qualitative data, thematic analysis was employed. After every interview was completed each day, the lead investigator played back the tape recorder and translated and transcribed the qualitative data with the assistance of one translator who speaks Sidamic fluently. Initially, the Sidamic transcription of the interview data was done without changing the words said by the interviewees. To verify the accuracy of the data, the transcribed information was examined and cross-referenced with the recorded information. After the translation was complete, the content was coded, and the codes were arranged according to emerging themes. After the data reached saturation, the initial themes were analyzed, revised, expanded upon, and refined in order to bring together all relevant information and pinpoint the essential concepts of each.
Ethical considerations
The Hawassa University College of Medicine and Health Sciences Institutional Review Board provided a letter of ethical clearance (APPROVAL NUMBER/ID = Ref No: IRB/049/14, Date: 15/02/2022). A formal letter of support was also sent to the Sidama region health bureau by the school of public health. The Sidama region health bureau once more sent a letter of support to the Teticha Woreda health office. Finally, the Woreda health office wrote a letter of support to selected kebeles. Each participant provided written informed consent following an explanation of the study’s nature, objective, and methodology by the data collector. The consent form was signed by each participant. On the consent form, signature was used. In addition to consent obtained from each participants who aged 17 years, additional consent was obtained from parents or guardian or legally authorized representative. By providing the participant with the code, respondent confidentiality was preserved throughout the whole study process. Individuals’ privacy as well as cultural customs were safeguarded. When requested, participants had to fill out the questionnaire in a different location. At the conclusion of the interview, participants who showed signs of having low MUAC status received dietary advice and were given directions to go to the health post for additional monitoring.
Results
Sociodemographic characteristics
This study had 446 pregnant women in total, with a 100% response rate. Of these, 290 (65%) reported being protestants, while 93 (20.9%) identified as Catholics. The age range of the pregnant women was 17–39 years. Pregnant women who did not have a food aversion were 25.87 (+5.1) years old on average (+SD), whereas those who did had a food aversion were 25.66 (+5.5). Among pregnant women who practiced food aversion, 93 (41.7%) had not obtained any formal education, whereas 74 (33.2%) pregnant women without food aversion had not obtained formal education. Regarding occupation, 131 (58.7%) pregnant women without food aversion were housewives, whereas 136 (61%) pregnant women from the food aversion group were housewives. Almost all 440 (98.7%) of the pregnant women were married. Regarding the occupation of their husband, 139 (64.1%) of pregnant women with food aversion and 99 (44.4%) of pregnant women without food aversion were farmers. The number of husbands of pregnant women with food aversion who attended secondary and above education was 35 (16.1%), whereas 56 (25.1%) of the husbands of pregnant women without food aversion attended secondary and above education (Table 1).
Sociodemographic characteristics of pregnant women, in Teticha Woreda, Sidama region, Ethiopia, March, 2022.

Reproductive health characteristics of pregnant women with food aversion
Among pregnant women with food aversion, 118 (21.1%) were in the third trimester of pregnancy and 187 (83.9%) had ANC follow-up. Among pregnant women who had ANC follow-up, 25 (13.4%) had four ANC visits. Pregnant women who had nutritional counseling during the ANC visit were 122 (65.2%). Primigravida women accounted for 79 (35.4%) of all pregnancies. Pregnant women who reported their current pregnancy as unintended were 105 (47.1%). Among multigravidas’ women, 11 and 19 women had abortions and newborn deaths in their previous pregnancies, respectively. Pregnant women who had a history of nausea and vomiting in their current pregnancy were 172 (72.2%). Pregnant women who gave birth at home in their last pregnancy were 79 (54.2%). Pregnant women who knew pregnancy danger signs were 98 (43.9%), and 62.2% of mothers ever used family planning methods (Table 2).
Reproductive-health-related characteristics of pregnant women, in Teticha Woreda, Sidama region, Ethiopia, March, 2022.

Reproductive health characteristics of pregnant women without food aversion
Among pregnant women without food aversion, 129 (57.8%) were in the third trimester of pregnancy. Pregnant women who had ANC follow-up were 184 (82.5%). Among pregnant women who had ANC follow-up, 20 (10.9%) had four ANC visits, and 87 47.2% did not get nutritional counseling during ANC visits. Of all pregnant women without food aversion, 142 (63.7%) were multigravida. More than half 123 (55.2%) of the respondents stated that their current pregnancy was intended. Multigravida women who gave birth at health facilities in their last delivery were 46 (39.4%). Sixty-seven percent of pregnant women had a history of nausea and vomiting in their current pregnancy. The majority of pregnant women (69.5%) were unaware of pregnancy danger signs, and 35.9% had never used FP methods (Table 2).
Dietary pattern of pregnant women with food aversion
Almost all 221 (99.1%) pregnant women ate three times per day. Regarding meal skipping, 37 (16.6%) of the women skipped at least one meal per day, and breakfast was the most frequently skipped meal, with a proportion of 29 (78.4%) followed by lunch (8, 21.6%). Only 30 (13.5%) ate additional meals during their current pregnancy. Of those women who ate an additional meal, 27 (90%) of them ate one additional meal a day (Table 3).
Meal patterns of pregnant women, in Teticha Woreda, Sidama, Ethiopia, March 2022.

Dietary pattern of pregnant women without food aversion
Like pregnant women with food aversion, almost all 218 (97.8%) women in this group ate three meals a day. The majority of pregnant women (84.8%) did not skip a meal, and 15.2% of women ate extra meals during their current pregnancy. Of those who ate additional meals, 30 (88.2%) of them ate one additional meal (Table 3).
Characteristics of pregnant women participated in qualitative study
Qualitative data were collected through in-depth interviews and key informant interviews. In-depth interviews were conducted with pregnant women and key informant interviews were conducted with mothers-in-law in Loya kebele. Eight pregnant women (Table 4) and six mother-in-laws were interviewed (Table 5). Each interview lasted an average of 35–60 min.
Sociodemographic and obstetric characteristics of pregnant mothers participated in qualitative study in Teticha Woreda, Sidama, Ethiopia, March 2022.

Sociodemographic characteristics of mother in-laws participated in qualitative study in Teticha Woreda, Sidama, Ethiopia, March 2022.

Food averted
According to this study, almost all of the participants believed that food aversions are a condition that happens when a woman gets pregnant, and it is due to the developing fetus and changes that take place inside the pregnant woman’s body.
I experienced food aversion in all of my pregnancies. Many of my friends and other women in my village who I know also experience food aversion when they get pregnant. I believe that it may be due to different changes that take place inside our bodies. (A 30-year-old pregnant woman with four children who was 6 months into her pregnancy). Food aversion is common during pregnancy. I used to avoid too many kinds of foods during my pregnancy. Similarly, all of my daughters-in-law and relatives also used to avoid certain kinds of foods when they got pregnant. It is due to a developing fetus inside the pregnant woman’s body. (A 52-year-old woman who had five children and two daughters-in-law)
Types of food items averted and reasons for food aversion
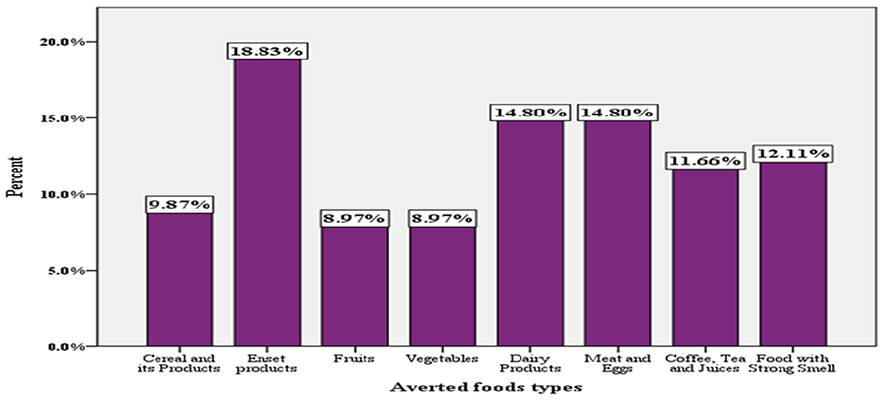
Among mothers who had food aversion, 42 (18.8%) averted “enset” products (“Enset” is edible plant which is a type of banana from which the food the so called “Kocho” is produced. Itis the staple food of the study society (Sidama region) and has high fiber content.), 33 (14.8%) averted dairy products, and 33 (14.8%) averted meat and eggs. Fruits and vegetables were the least averted food items. In line with quantitative study findings, mothers who participated in a qualitative study averted cereals, “enset” products, and dairy products (Figure 1).
I used to avoid “enset” products and foods cooked with butter that have a strong odor during the first 4 months of my pregnancy; I don’t even want to see other people eating such food items. (24 years old, pregnant with 2 children). My daughter-in-law avoids milk and butter during her pregnancy. (54 years old and had 5 children and 3 daughters-in-law).
In the quantitative study, 95 (42.6%) mothers reported that the smell or taste of food was the reason for food aversion, followed by heart burn (49.22%) and nausea and vomiting (34.15.2%) (Table 6).
Reported reason for food aversion of pregnant women in Teticha Woreda, Sidama region, Ethiopia, March 2022.

Reported averted food types by pregnant women in Teticha Woreda, Sidama region, Ethiopia, March 2022.
Similarly, in the qualitative interview, most pregnant women assumed that the taste or smell of food, heartburn, nausea, and vomiting were the reasons for food aversion during pregnancy.
I don’t like to eat “enset” products once I get pregnant, since it causes discomfort in my stomach and heartburn. (A six-month pregnant woman, 23 years old). I didn’t use milk products for the first six months of my pregnancy; I’ve had vomiting even when I see someone using them and smell their odor; especially butter. (An eight-month pregnant, 32-year old mother). I avoided using cereal products in my current pregnancy because as soon as I eat cereal, I experience heartburn and finally vomit everything. (A five-month pregnant, 29-year old mother). My daughter-in-law can’t have coffee during her pregnancy. An odor of coffee was her reason of avoidance. (60 year old mother-in-law who had 6 children and 1 daughter-in-law).
Food restriction and reasons for restriction
From all respondents, 283 (63.5%) mothers reported that there is a food restriction for a pregnant mother in a community (Table 7). Sweets restriction was reported by 87 (30.1%) mothers, and organ meat restriction was reported by 72 (25.4%) mothers (Figure 2). The most stated reason for food restrictions was that the community believes that those foods make a fetus grow big 89 (31.4%) and also hurt the fetus 87(30.7%). Findings from the qualitative study show that there are taboos/restrictions for various food items. Pregnant women are advised to avoid food items like meat, dairy products, some fruits, and sugarcane during pregnancy by the community members. It is believed that these foods’ intake during pregnancy may increase the probability of having a big baby and cause labor difficulty. Also, pregnant women are advised to avoid green leafy vegetables (especially cabbage) and milk and milk products. It is believed that they could be plastered to the fetal head and discolor the baby’s body. Further, there is a restriction on organ meat intake, believing that it increases the risk of abortion and fetal death.
Food restriction and reasons for food restriction for pregnant women in Teticha Woreda, Sidama region, Ethiopia, March 2022.


Reported restricted food types by pregnant women in Teticha Woreda, Sidama region, Ethiopia, March 2022.
I avoided eating cabbage during my pregnancies because my mother-in-law warned me that it could be plastered to my baby’s head and cause “hamessa” (a disease known by the community that is characterized by skin rash, greenish stool, and newborn crying (they assumed the baby cried due to hamessa; and is treated by herbs extracted from trees) on the child after birth. (A 26-year-old pregnant woman with one child who is 9 months pregnant). My family used to tell me not to consume foods like meat and sweets like sugarcane and avocado during my pregnancy since they could make the baby big and delivery difficult. Oils and cabbage could also be plastered to the fetal head, and the newborn may suffer from “hamessa” “Hamessa” is an infant disease known by the study community (Sidama region) which characterized by skin rash, greenish stool (diarrhea) and newborn strong cry (they assumed that the baby cry because of abdominal cramp secondary to Hamessa); and it is treated by herbs extracted from tree.). Therefore, I didn’t consume these foods during my pregnancies. I also advise my pregnant daughters-in-law and other pregnant women around my village to avoid these foods during their pregnancy since they could harm their own and their babies’ health. (A 60-year old pregnant woman who had five children and two daughters-in-law). Our community strongly believes that if a pregnant woman eats sugar cane and fruits she may have a big baby, which endangers her life by making labor difficult, so I didn’t use those food items in all of my pregnancies. (A 24-year-old pregnant with 2 children). My family teaches me not to consume liver and kidney during my pregnancy because eating those meats results in abortion. So, I didn’t do it during my pregnancies. I also advise my pregnant daughters and daughter-in-law to avoid eating kidney and liver during their pregnancy since they could harm the fetus. (61 years old, had 7 children and 4 daughters-in-law).
Prevalence of undernutrition
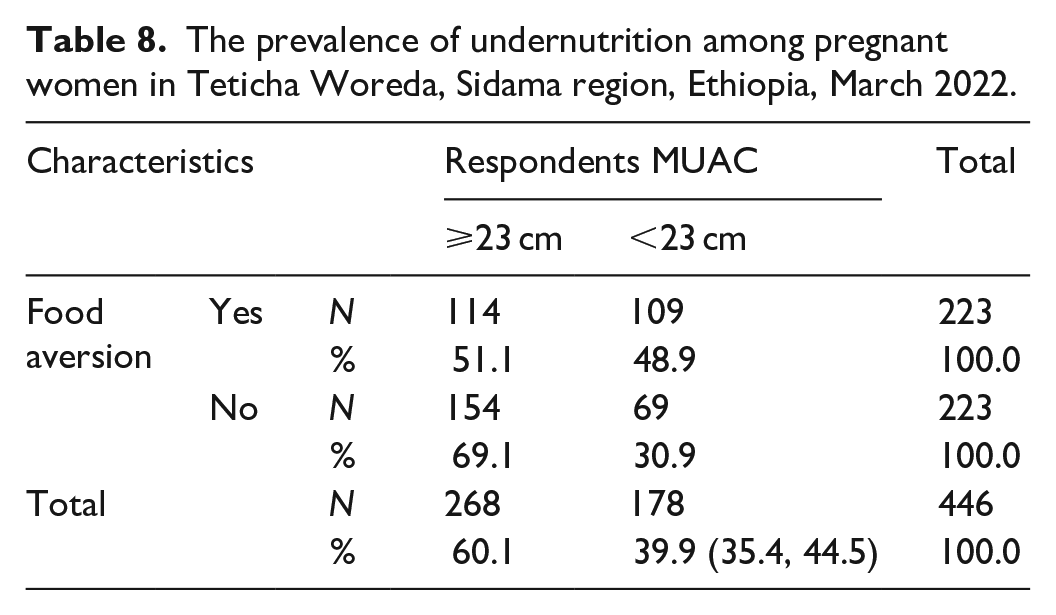
In total, 178 (39.9%) (95% CI: 35.4%–44.5%) pregnant mothers had MUAC measurements less than 23 cm, indicating maternal malnutrition. Of these pregnant women who had a low MUAC measurement, 109 (61.2%) were from the group who had food aversion during their current pregnancy (Table 8).
The prevalence of undernutrition among pregnant women in Teticha Woreda, Sidama region, Ethiopia, March 2022.
Pregnant women’s food aversion association with their MUAC status
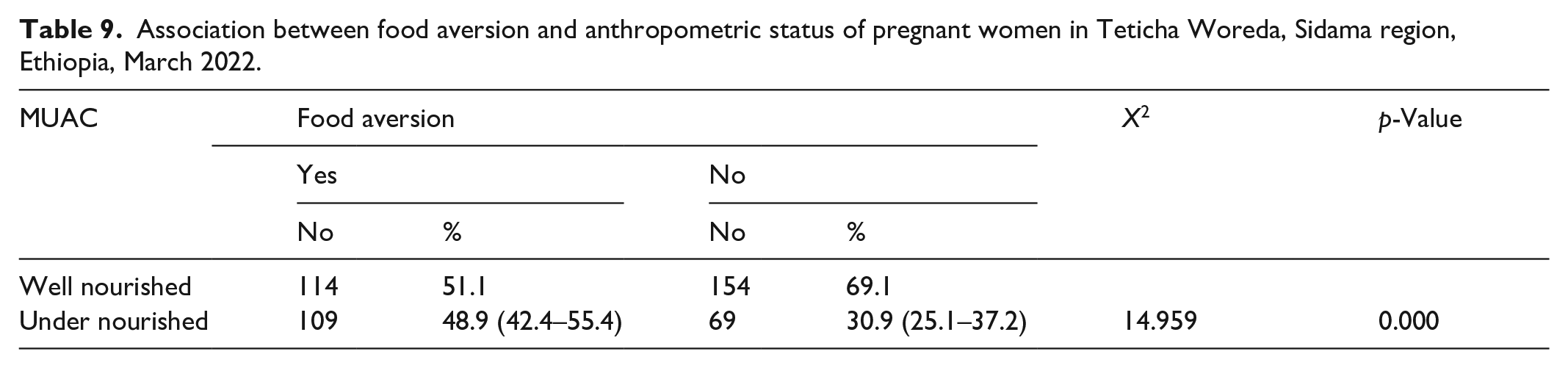
In order to determine how pregnant women’s anthropometric status was associated with food aversion, a Chi-square test was utilized. The anthropometric status of pregnant women and food aversion practice are significantly associated, as indicated by Table 9’s p-value of 0.000, which is less than the 0.05 level of significance. The likelihood of malnutrition (MUAC < 23 cm) is thus higher in women who have a food aversion (Table 10).
Association between food aversion and anthropometric status of pregnant women in Teticha Woreda, Sidama region, Ethiopia, March 2022.
Multivariable logistic regression analysis of maternal under nutrition and food aversion adjusted for other variables.

p-value is significant at p < 0.01, p-value of Hosmer and Lemeshow Test = 0.31
Discussion
The study’s quantitative findings indicated that 39.91%% of pregnant women (95% CI: 35.4%–44.5%) were undernourished. Of these mothers who had low MUAC measurements, 109 (48.9%; 95% CI: 42.4%–55.4%) were from a group who had food aversion during their current pregnancy, and 69 (30.9%; 95% CI: 25.1%–37.2%) were from mothers without food aversion. Also pregnant mothers and mother-in-law participated in the qualitative study perceived the existence of food aversion during pregnancy. This may be due to physiological, culture, and family structure in the study community. Similar findings were reported in study conducted in Pakistan where a combination of physiological, sociocultural, and structural barriers that inhibited healthful dietary intake during pregnancy. 13 This finding suggested that undernutrition and food aversion affected a significant proportion of women. The long-term health and nutritional consequences of the mother and her developing fetus are, therefore, greatly influenced by the nutritional status of the mother before and during pregnancy.
In this study, the undernutrition prevalence among mothers with a history of food aversion during their current pregnancy was 48.9%, which exceeds than the 38.4% found in the study conducted in Boricha Sidama. 14 This discrepancy may be due to different study periods and study designs, as this study employed a comparative method, whereas the overall maternal undernutrition findings of this study were nearly equivalent to those of cross-sectional studies carried out in Ethiopia’s northern Tigray (40.6%), Konso (43.1%), and Goro Dola District, Guji Zone (41.2%).6,16,17 The results’ similarity could be explained by similarities in the socioeconomic characteristics of pregnant women. As a result, the household’s ability to purchase food is based on its income. Lower-income households find it challenging to ensure food security while meeting the dietary needs of pregnant women. Pregnant women who have a food aversion may be more likely to experience undernutrition in these situations. On the other hand, studies showed that pregnant women from households with food security had a lower risk of undernutrition.18–20
On the other hand, the undernutrition prevalence was higher when compared to other similar studies conducted in Boricha Sidama (34.6%), Dale Sidama (15.2%), Gondar town (14.4%), Silte (19.5%), Hosanna (24.6%), Gambela (24.6%), and China (21%).13,21–26 Discrepancies were might be due to sociodemographic characteristics, cultural beliefs such as food taboos, difference in assessment season, range of measurement (study done in Dale and Gambela used MUAC < 21 cm and studies from Hosanna and Gondar uses <22 cm as a cutoff point for undernutrition respectively, while this study used <23 cm), settings (study from Silte and Hosanna were facility based), term of pregnancy (the Gondar study included women in the second and third trimester, while this study includes all), and variation in the sample size.
However, the level of maternal undernutrition observed in this study was significantly lower than that reported from the Ethiopian field site of the Kersa Demographic Surveillance and Health Research Center, which was 47.3% 27 and 71.1% of another study conducted in Southern Nations, Nationalities, and Peoples region. 28
In this study, 63.5% pregnant women reported that there is a food restriction for pregnant women in a community. Sweets and organ meat were common food items restricted by pregnant women. The finding is consistent with a study conducted in Arsi Ethiopia 23 ; the most restricted foods in the study area were fruits, oils and fats, cabbage, and sweets. Moreover, according to the findings of the qualitative part of this study, pregnant women usually avoid cereal products, meat and eggs, dairy products, and enset during their first trimester of pregnancy. This study is in line with that of Boricha district, Sidama Ethiopia. 13 Also, this finding supports the idea which was reported by another study where pregnant women avoid commonly eaten or staple foods. 16 The Sidama Region, where this study was done, is similar to other study place, which is likely the cause of the observed comparability. Cereals and enset were among the foods that were recognized as staples in the study area. These food items were restricted for the concern for difficult deliveries, even though it is generally accepted that ideal weight gain is a sign of a healthy pregnancy.
Strength and limitations of the study
Study’s strengths
Key strength of the study is its utilization of both quantitative and qualitative research methods.
Limitations of the study
Before conducting individual interviews, the goal was clearly stated in detail in order to minimize the potential influence of social desirability bias on some variables, such as meal frequency, skipping meals, and additional meals. Because the study only employed the single MUAC assessment, which does not account for seasonal variations in dietary consumption, there may be seasonal variations in the nutritional status of pregnant women. Manual analysis was performed on the qualitative data.
Conclusion
This study found that the prevalence of maternal undernutrition in Teticha district among pregnant women who had food aversion in their recent pregnancy was 48.9% (95% CI: 42.4%–55.4%). This study indicates that maternal undernutrition among mothers with food aversion is relatively higher than their counterparts.
Since poor maternal nutrition has a significant impact on replicating the intergenerational cycle of malnutrition, due to its negative effect on the developing fetus. Thus, it is critical to comprehend inappropriate eating behaviors, such as food aversion, in order to manage maternal nutrition problems throughout pregnancy.
In the qualitative section, food aversion and food taboos are well-known phenomena in the study area. The most commonly avoided food types were cereal products, meat, eggs, dairy products, coffee, tea, and “enset” products.
The most prohibited foods in the research area were cabbage, oils and fats, sweets, and fruits. Some of the responders do not attribute their behavior to any particular reason. Heartburn, food odor or taste, nausea, and vomiting were the most common reasons for food aversion. Cultural beliefs, like some food types harm the fetus, make the fetus big, and create labor problems, were the most stated reasons for food restrictions in the study area.
The reasons given for food aversion and food taboos by the respondents were nutritionally incorrect. This suggests that nutritional interventions, especially dietary education, should be intensified.
Recommendations
The study’s findings resulted in the following recommendations being forwarded to all relevant stakeholders:
For health care providers, health education must be strengthened, especially focusing on nutrition, including how pregnant mothers correct food aversion (by changing texture and smell/taste of food items that are averted), alternative food choices for pregnant women who are practicing food aversion, and the adverse effect of food taboos.
For nongovernmental organizations—Given that many of the pregnant women in the study region were found to practice food aversion, which may have an impact on the dietary habits and nutritional status of pregnant women, those organizations that engage in nutritional activities ought to concentrate on the needs of maternal nutrition as well.
For other researchers: further research on maternal malnutrition and food aversion using different study designs, setup, and sample size should be done.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241284950 – Supplemental material for Food aversion and its association with pregnant women’s nutritional status in Teticha Woreda, Sidama Region, Ethiopia: A community-based mixed comparative cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121241284950 for Food aversion and its association with pregnant women’s nutritional status in Teticha Woreda, Sidama Region, Ethiopia: A community-based mixed comparative cross-sectional study by Turufat Paskal Gebre, Temesgen Tafesse and Teshome Abuka Abebo in SAGE Open Medicine
Footnotes
Acknowledgements
Our heartfelt thanks will go to Hawassa University for its institutional commitment to permitting us to undertake this scientific project. We greatly thank Teticha Woreda health office and health extension workers for providing us with all the necessary support during data collection. We would like to acknowledge the data collectors and supervisors for their tremendous commitment throughout data collection period. Finally, we would like to acknowledge the study participants for their cooperation during data collection.
Authors’ contributions and declaration
T.P.G, T.T, and T.A.A wrote the proposal, participated in data collection and data analysis, and drafted the paper. All authors participated in preparation of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from the Hawassa University, College of Medicine and Health Sciences, Institutional Review Board (APPROVAL NUMBER/ID = Ref No: IRB/049/14, Date: 15/02/2022).
Informed consent
Written informed consent was obtained from all subjects before the study. In addition to consents obtained from each participant who aged 17 years, additional consent was obtained from parents or guardian or legally authorized representative. Also written support letter was obtained from legally authorized representatives before the study. It was from Sidama Region Health Bureau and Teticha Woreda Health Office.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.