
Abstract
Objectives:
To assess the feasibility, acceptability, and preliminary effectiveness of implementing a home-based aerobic and resistance exercise for patients with breast cancer receiving endocrine treatment in Indonesia.
Methods:
This is a mixed methods study with concurrent design consisting of quantitative single-arm pre-post intervention and qualitative study. We recruited patients with breast cancer (N = 36) receiving endocrine treatment and assigned 12 weeks of home-based pedometer-driven walking and resistance exercises using therapeutic bands. Descriptive statistics were used to assess the feasibility (recruitment, retention, and adherence) and safety. The modified Bruce treadmill test was used to measure predicted aerobic capacity (
Results:
The results showed a recruitment rate of 75%, retention rate of 89%, and adherence rates were 53% for aerobic and 78% for resistance exercise. No severe adverse events were reported. Post-intervention interviews identified positive attitudes toward the intervention, with low burden and high perceived benefit. Exercise duration and predicted
Conclusions:
A home-based aerobic and resistance exercise was feasible when implemented in the context of routine care in our study population, improving predicted aerobic capacity. Further research is required to understand limited changes to Quality of Life and fatigue and adaptations to support implementation in additional sites in Indonesia.
Introduction
Female breast cancer (BC) is the most commonly diagnosed malignancy worldwide with 2.3 million new cases or 11.7% of all newly diagnosed cancers in 2020. In Indonesia, BC has the highest incidence (65.858 new cases, 16.6%) of all cancer types and is the second leading cause of cancer death (9.6%). 1 Specifically, in the region of Yogyakarta, a province in Java that has the highest cancer prevalence in the country, BC is dominated by late presentation of patients with advanced disease (59.4%).2,3 Similar to most countries, the highest prevalence of BC (86%) in Yogyakarta is hormone receptor-positive BC.4,5 This patient population generally receives endocrine treatment for a minimum duration of 5 years, which can result in a multitude of adverse health effects (e.g., pain, arthralgia, reduced muscle mass, and strength) up to 14 years after diagnosis. 6 Finding solutions to help patients to self-manage health problems associated with the disease and its treatment is imperative.
Physical activity can reduce many of the adverse effects resulting from treatment for BC and is a cost-effective, empowering approach that can support self-management.7,8 There is strong evidence that combined moderate-intensity aerobic and resistance exercise performed 2–3 times per week for at least 12 weeks can improve physical function and quality of life (QoL), prevent reoccurrence, prolong survival, and reduce fatigue both during and after BC treatment.7,9,10 Cancer patients are advised to perform 150 min of moderate intensity, or 75 min of vigorous physical activity weekly, as recommended by the American College of Sports Medicine (ACSM). 9 It also recommends performing muscle-strengthening exercises at least twice a week. However, many BC patients become physically inactive after breast surgery due to limited function and mobility of the upper extremity, 11 alongside increases in sedentary behavior mainly due to fatigue. 12 In many low- and middle-income countries (LMICs), increased levels of physical inactivity are exacerbated by a lack of access to high-quality facilities for rural residents, program availability, and lack of information and tailored advice. 13 Supporting patients to be active at the recommended level during and after treatment is therefore important for improving their overall health and well-being. However, there is limited research as to how to support patients in LMICs. Home-based programs may be an effective way to do this.
Exercise prescribed to patients with BC in the home environment has been found to result in significant improvements in aerobic capacity and QoL.11,14,15 Home-based programs are acceptable, convenient, and safe and can be delivered to patients using minimal resources.13,16 However, the bulk of the evidence in this area is heavily skewed toward patients who live in high-income countries (HICs)10,16 with limited research conducted in LMICs. Research findings from HICs may not be transferable to LMICs due to differences in demographic characteristics, health system capacity, sociocultural factors, and resource availability. 17 Furthermore, the word “exercise” and other related terms are not shown in the bibliometric network visualization indicating an under-explored research topic in Indonesia. 18 Home-based exercise programs in LMICs may be important for promoting physical activity in this population as lack of funding, paucity of trained rehabilitation specialists, and lack of a tailored physical activity plan often hinder supervised hospital-based program delivery. 19
Exercise interventions considering sociocultural factors are more effective in influencing health outcomes. It is important to evaluate participants’ acceptance of exercise intervention to assist with their needs and challenges to adhere to exercise intervention. 13 More knowledge about how our patients with BC accept and experience the quantitative change after completing home-based exercise intervention can enrich the findings from the quantitative measurements. This knowledge can provide a holistic picture of implementing a home-based exercise program for patients with BC in Indonesia and develop tailored interventions based on our patients’ experience and acceptance.
The purpose of this mixed methods study was the quantitative assessment of feasibility and preliminary effectiveness of a 12-week home-based exercise program, with qualitative description of how our patients with BC experience and accept the program implementation. We hypothesize that home-based aerobic and resistance exercise is feasible, acceptable, and effective for Indonesia BC patients.
Methods
Study participants and design
A mixed methods study using concurrent design was conducted from January to July 2022 in patients with BC receiving endocrine treatment. This study consisted of a single-arm pre-post intervention study used to evaluate the quantitative feasibility and preliminary effectiveness of participating in a home-based exercise program and a qualitative measure using a semi-structured interview to describe the intervention’s acceptability. Participants were recruited between 3 January and 8 April 2022. Data were collected using a range of device-based (i.e., pedometer, treadmill test) and subjective (i.e., questionnaires, recall interviews, self-reported diaries) measures.
This study enrolled BC patients aged 18–70 years, who had completed primary treatment and received endocrine treatment. Patients with stage I–III BC with Eastern Cooperative Oncology Group score ⩽1 were recruited using a consecutive sampling approach. They were included if they: (a) had completed primary treatment (e.g., surgery, chemotherapy, and radiotherapy); (b) were within 5 years of diagnosis; (c) received ongoing endocrine treatment; (d) were able to perform moderate-intensity physical activity as determined by their oncologist and care team; (e) were able to read and write in Bahasa, Indonesia; and (f) were willing to provide written informed consent. Patients were excluded from the study if they had an ejection fraction of <50%, evidence of cardiac disease, severe musculoskeletal problems, or other contraindications for exercise.
A previous study by Rogers et al.
20
reported a
Study procedures
Potential participants meeting all eligibility criteria were approached by their oncologists (SHH, MSH) during a hospital appointment in the cancer clinic, and the study objectives were explained. All recruited participants signed a written informed consent form before participation. The intervention consisted of a 12-week, home-based, personalized moderate-intensity aerobic and resistance exercise program. All participants received a face-to-face 30-min instructional session with the clinical study coordinator (YKA) under cardiac prevention and rehabilitation consultant supervision (ABH), before they started the intervention. They were provided with a pre-packaged kit, which included a detailed written manual of the intervention, a pedometer (Yamax Digiwalker SW-200, Tokyo, Japan), a set of resistance bands (Happy Fit®, Jakarta, Indonesia), and a self-report diary.
The aerobic exercise consisted of a walking program based on the number of steps per day, which was recorded using a pedometer. The pedometer elicited acceptable inter-unit reliability (p < 0.05) and excellent intra-trial reliability (interclass correlation ⩾ 0.75). 23 Patients were asked to wear the pedometer daily, except when they were sleeping, and were instructed to record their number of steps per day during the 12-week intervention. Patients’ average number of steps per day in the first week served as a baseline value. 24 The target of the aerobic exercise was individually tailored by adding 3000 accumulated steps above their baseline value on 5 days of the week. This value was based on the assumption that moderate brisk walking produces 100 steps a minute. Therefore, 3000 steps would equate to approximately 30 min of moderate-intensity aerobic activity, in line with ACSM recommendations. 24
The resistance exercise program consisted of two sets of biceps curl, triceps extension, chest press, shoulder flexion, shoulder press, lateral extension, seated row, and upright row, with 8–10 repetitions. 25 Patients were instructed to perform each exercise with an average total duration of 10 min on 2 days a week, based on current recommendations 7 at home. The exercises were individually tailored based on participants’ strength and range of movement using a set of three color-coded bands representing low, moderate, and high levels of resistance. The resistance program was focused on targeting the upper body, as the aerobic program focused on the lower body through walking. The participants recorded their resistance exercise frequency, duration, and intensity in a self-reported diary.
The study coordinator (YKA) explained and demonstrated the proper use of the resistance bands and how to safely perform the exercises during the initial 30-min instructional session. A video and written manual was developed and given to patients as guidance. It consisted of step-by-step instructions on how to complete the exercises, exercise frequency, repetition, and intensity (2–4 rating of perceived exertion on a 1–10 Borg scale).
The study coordinator monitored participation through weekly phone communication, recording any side effect occurrence and providing patients with a target for the following week. During participants’ visits to the hospital for their monthly check-ups, they were asked to perform each exercise so the study coordinator could assess their technique and adjust the level of intensity if required.
Measures
Demographic and clinical characteristics
Demographic data collected included age, educational background, employment, and marital status. Clinical data was also collected including body mass index, hypertension comorbidity, cancer stage, primary treatment received (e.g., surgery, chemotherapy, and radiation therapy), and details about the type of endocrine treatment (selective estrogen receptor modulators (SERMs), such as tamoxifen, and aromatase inhibitors (AIs), such as letrozole, anastrozole, and exemestane). Demographic and clinical data were extracted from the participant’s medical records at baseline.
Intervention feasibility
Intervention feasibility was determined by (a) recruitment (ratio of the number of participants recruited to the number of eligible participants approached), (b) retention (ratio of the number of participants who completed the 12-week program to the total number of participants enrolled in the study), (c) adherence (the ratio of the number of participants meeting at least 70% of prescribed activities calculated using steps per day, resistance exercise frequency, duration, and intensity to the total number of participants completing the 12-week program) defined as feasible if those rates were above 75% 26 , and (d) adverse events (e.g., dyspnea, tachycardia, nausea, pain, and myalgia) reported by participants. Adherence data was extracted from participant’s self-reported diary. Baseline demographic, clinical, and treatment factors were compared between adherent and non-adherent participants.
Intervention acceptability
Intervention acceptability was explored using semi-structured interviews with participants (N = 25) post-intervention to: (a) explore their experiences of participating in the intervention and; (b) understand the most prominent aspects of intervention acceptability. The first and last authors (YKA, an MD and graduate student in Master of Medical Science program, and SB, a PhD well-versed in qualitative research) developed the interview guide based on the main areas outlined in the theoretical framework of acceptability. 27 The interview guide was pilot-tested on the first four participants (16%), and minor revisions were made before implementing the final version. Before each interview, informed consent was obtained. Interviews were conducted by two members (AS, FB) of the Center of Health Behavior and Promotion, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada trained in qualitative interview techniques. All interviews were individual and face-to-face, took place in a private room in the cancer clinic, lasting approximately 25–40 min, and audiotaped. No non-participants were present during the interview.
Intervention effectiveness: Aerobic capacity
Participants’ aerobic capacity was assessed at baseline and after participation in the 12-week intervention. Aerobic capacity was determined with the modified Bruce treadmill test, which is a predictive submaximal exercise test deemed appropriate and safe for subjects with a low or unknown functional capacity.
28
A cardiac prevention and rehabilitation consultant (ABH) monitored and supervised all procedures. The treadmill test (Cardiac ScienceTM TM55, Hannover, Germany) was conducted at the Cardiac Rehabilitation Unit, Dr Sardjito General Hospital. Cardiac rehabilitation nurses (EW, DP) measured a participant’s blood pressure at rest, during the test stage, and recovery phase while their heart rate was automatically recorded using a treadmill test monitor. Treadmill speed and inclination were automatically increased every 3 min (test stage). The test was terminated when participants reached volitional fatigue. Exercise duration was recorded in minutes, and aerobic capacity was calculated as
Intervention effectiveness: QoL and fatigue
Quality of life and fatigue were assessed at baseline and after participation in the 12-week intervention using translated and validated Indonesian versions of the EORTC Quality of Life Questionnaire (QLQ-C30) 29 and Fatigue Severity Scale (FSS). 30 A member of the research team (NDS) administered the questionnaires in a private room at the hospital. The EORTC QLQ-C30 consists of global health status, functional scales, and symptom scales. A higher score indicates better health for global health status and functional scales but represents a higher level of burden for symptom scales. 31 The FSS is a nine-item questionnaire to assess the severity of fatigue symptoms and its impact on an individual’s daily functioning. A higher score of the FSS represented a more severe fatigue level and also was classified as no-to-mild fatigue (FSS < 4.0) and severe fatigue (FSS ⩾ 4.0). 32
Data analysis
Participants’ characteristics were calculated using means and standard deviation for numerical data and were described with frequencies and percentages for categorical data. Descriptive statistics were used to calculate the feasibility outcomes including recruitment, retention, adherence rate, and intervention safety. Baseline characteristics were compared between adherent and non-adherent participants using Chi-Square test.
Quantitative analysis
To analyze the effects of the 12-week home-based intervention on health outcomes, we used a paired t-test for treadmill test parameters, except for the physical fitness that was analyzed with the McNemar test as the data was non-parametric. As QoL and fatigue scores were not normally distributed, we used the Wilcoxon signed rank test for the analysis. Participants with complete evaluation data were further classified into two groups (with and without improvement) based on their aerobic capacity change after the 12-week intervention. Participants’ baseline characteristics were analyzed between groups using logistic regression. Participants with incomplete data were not included in the analysis. The p-value under 0.05 was considered statistically significant while p-value under 0.10 was considered a trend that may have clinical significance. Data were analyzed using STATA software, version 17 (Stata Corp., College Station, TX, USA).
Qualitative analysis
Interviews were audiotaped and transcribed verbatim. The analysis followed a deductive thematic approach 33 guided by the theoretical framework of acceptability. 27 The first author (YKA) reviewed all transcripts line by line to become familiar with the data and created descriptive codes. Text passages that had been coded multiple times were put together and designated as a potential sub-theme. These initial sub-themes were then grouped into the themes described in the theoretical framework of acceptability. The transcripts were then reread to make sure no information was left out. The last author was interested in this topic due to prior experience in physical activity research and assumed that this intervention was acceptable for study participants. However, alternative interpretations for the data that were generated were proposed and discussed with the research team using a collaborative procedure. 34 The analysis was conducted manually. Specific quotations were selected to illustrate each of the sub-themes. To ensure confidentiality, each participant was given an arbitrary number as their identifier in the transcripts.
Results
Patient characteristics
The mean age of participants (N = 36) was 52 ± 6.98 years old. All participants had mastectomy and chemotherapy, in which 89%–92% of patients also received radiation therapy. Endocrine therapy regimen used was tamoxifen (SERMs) in 48%–53% and AIs in 52%–55% of participants. The average endocrine therapy duration was 26.9–28.5 months at baseline. There was no baseline characteristics difference between recruited and interviewed participants (Table 1).
Demographics and clinical baseline characteristics.

SD: standard deviation; BMI: body mass index; SERMs: selective estrogen receptor modulators; AIs: aromatase inhibitors.
Intervention feasibility
Recruitment
During the recruitment period between 3 January and 8 April 2022, 48 eligible patients were approached and 36 patients agreed to participate in the study. Six patients declined due to being too busy to participate, two because they were not sure if they would be able to adhere to the intervention and four were reluctant to engage in the study, resulting in a 75% recruitment rate.
Retention and adherence
A total of four participants dropped out from the study due to schedule conflict (n = 1), sickness (n = 1), and did not attend post-intervention data collection (n = 2), resulting in a retention rate of 89% (Figure 1). However, one additional participant who completed the 12-week intervention has partial data, as they had to be excluded from the post-intervention treadmill test and aerobic capacity analysis due to newly acquired musculoskeletal problems. They were able to complete the questionnaires that were included in the analysis.

Flow diagram of participants’ recruitment. From 48 approached eligible patients, 36 patients agreed to participate in the study. Four participants dropped out and one additional participant was excluded from the post-intervention treadmill test analysis. A total of 25 participants underwent semi-structured interview at the end of the study.
Fifty-three percent of participants adhered to the aerobic program, achieving at least 70% of the step/day target. The average number of steps per day significantly increased from baseline to week 12 (5694 ± 2820.98 vs 7728 ± 2509.34; p < 0.001) (Figure 2). Seventy-eight percent of participants adhered to at least 70% of the prescribed resistance exercise sessions. Participants reported an average of 10.3 ± 5.40 min duration and 2.2 ± 1.21 days a week resistance exercise frequency, with a rating of perceived exertion of 3 out of 10, indicating moderate intensity. Participants’ adherence was measured based on self-reported diary and weekly phone monitoring by the research team. There was no significant difference in baseline characteristics including demographic, clinical, and treatment factors, between adherent and non-adherent groups (Table 2).

Participants’ steps per day during the 12-week physical activity intervention. Box plots demonstrated the participants’ steps per day during the 12-week study intervention. Horizontal line is the participants’ median target by adding 3000 steps/day (median 8800 steps/day).
Baseline characteristics influencing participants’ adherence.

BMI: body mass index.
Safety
No severe adverse events were reported. However, five patients (13.9%) reported myalgia after completing the resistance exercises. One participant reported pain, swelling, and discharge around post-mastectomy wounds after completing the 12-week intervention. All symptoms were relieved after a week of oral antibiotics treatment and twice-a-week wound debridement. Due to the absence of laboratory investigation, infection etiology could not be excluded and this case might not be related to study intervention.
Intervention acceptability
Findings on acceptability of the intervention are presented under three separate but interconnected themes including affective attitude, burden, and perceived effectiveness. Exemplary quotes are presented in Table 3 to represent participants’ affective and cognitive responses associated with participating in the home-based program.
Relevant quotations of acceptability themes from BC patients’ participation in home-based exercise intervention (N = 25).

Affective attitude
Most participants reported enjoying participation in the program, with some describing that goal-setting (i.e., target step counts) served as a motivation and challenge that encouraged them to do more. Furthermore, regular contact with the research team provided many participants with a sense of reassurance that they were completing the exercises correctly. However, one participant recounted experiencing discomfort while walking (e.g., knee and foot pain), which had a negative impact on her ability to complete the walking sets.
Burden
The combined aerobic and resistance program was, for the most part, described as straightforward to complete and was not considered to be burdensome. Walking was typically perceived as simple and easy to do, while resistance exercise required participants to concentrate on proper technique. Participants spoke about the benefit and ease of being able to complete the exercises in the home setting, providing them with flexibility in when and where to do the exercises. However, for most participants, there was an initial period at the start of the program that was perceived as stressful. This was due to having to learn new exercises alongside becoming familiar and comfortable with apparatuses such as resistance bands and belt-worn pedometers. In contrast with the vast majority of participants who believed goal-setting was a motivation for them, one participant reported feeling burdened by the need to achieve a weekly exercise target.
Perceived effectiveness
Most of the participants reported feeling that their fitness and stamina improved, and also felt less tired (fatigue), following participation in the program. For some, participating in this program was novel since they did not regularly exercise or participated in no exercise at all. Participants reported positive physical changes including improved range of movement and upper body strength, reduced post-surgical pain, and symptom improvements including increased appetite and reduced tingling in their arm. Psychological improvements were also noted by some participants, such as increased physical self-efficacy and overall well-being.
Intervention effectiveness
Aerobic capacity
At baseline, we found 18 participants (58.1%) had low fitness, 9 (29%) fair fitness, 3 (9.7%) average fitness, and only one participant (3.2%) had good physical fitness, based on the normative values from ACSM.
26
After the 12-week home-based intervention, the number of participants with low and fair physical fitness was reduced (54.8% and 19.4%), while the number of participants with average and good physical fitness was increased (16.1% and 9.7%) (Figure 3). Additionally, the 12-week home-based aerobic and resistance exercise intervention significantly increased test duration and aerobic capacity in predicted

Participants’ physical fitness before and after the 12-week physical activity intervention. A Sankey diagram described participants’ physical fitness before and after the 12-week study intervention. Physical fitness was classified as low, fair, average, and good fitness based on aerobic capacity and age. Line thickness indicates participants’ proportion.
Modified Bruce treadmill test results before and after intervention (N = 31).
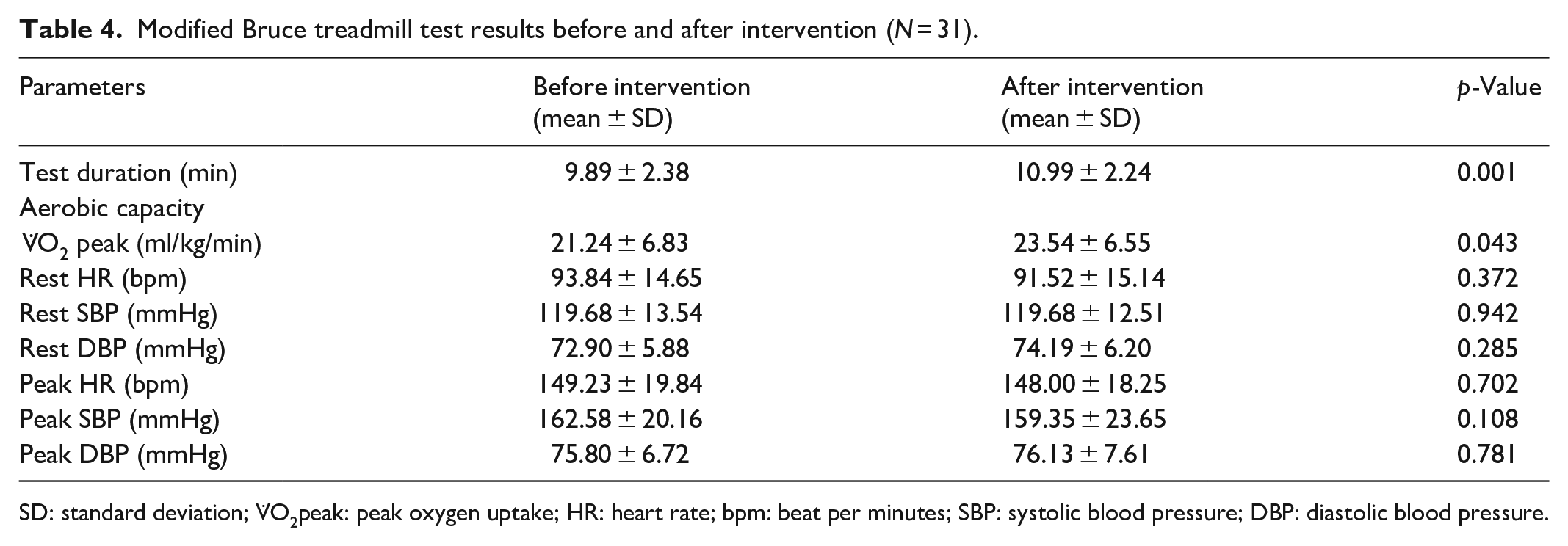
SD: standard deviation;
Twelve participants (38.7%) demonstrated improvement in aerobic capacity after a 12-week intervention, while the rest (n = 19; 61.3%) remained the same or declined. From logistic regression, we found that hypertension comorbidity and low physical fitness at the baseline were significantly associated with aerobic capacity improvement (p = 0.031 and 0.033) (Table 5). Adherence rates to the intervention were not significantly associated with aerobic capacity improvement (p = 0.246 and 0.798).
Participants’ baseline characteristics influencing aerobic capacity improvement (N = 31).

OR: odds ratio; CI: confidence interval; BMI: body mass index.
Quality of life and fatigue
The mean of each QoL domain and FSS at baseline and post-intervention was presented in Table 6. There were no significant changes in all QoL domains before and after the 12-week intervention (p > 0.050). However, most domains in the functional scale were slightly higher in post-intervention evaluation, and appetite loss was trending toward improvement (p = 0.083). The exercise intervention appeared to decrease fatigue severity although statistical significance was not reached (p = 0.299).
Quality of life and fatigue before and after intervention (N = 32).

SD: standard deviation; EORTC QLQ-C30: European organization for research and treatment of cancer quality of life core questionnaire; QoL: quality of life; FSS: fatigue severity scale.
Discussion
This study reports on the feasibility, acceptability, and preliminary effectiveness of a home-based exercise program delivered during endocrine treatment for patients with BC. This is the first study to implement a combined aerobic and resistance exercise intervention in BC care in Indonesia. It is also one of few studies that have used a personalized exercise program in a home setting in an LMIC. In addition, few studies in LMICs have used a predictive submaximal exercise test to assess changes in physical fitness. Our study demonstrated that participation in a 12-week home-based exercise was feasible and acceptable. Moreover, preliminary findings point toward significant increases in predicted
Despite a considerable amount of research investigating the impact of exercise on outcomes for patients with BC, studies that focus on home-based interventions that can be embedded in a real-world setting are scarce. 35 In Indonesia, evidence-based interventions that are affordable, accessible, low burden for healthcare professionals and can be delivered as an integrated pathway are needed to improve outcomes for patients with BC. Most countries in low resources settings struggle to deliver exercise interventions due to a lack of resources, space, equipment, and trained professionals. 36 Our study is one of the first studies to identify and analyze indicators addressing the possibility of delivering home-based exercise (e.g., feasibility and acceptability) in the context of cancer care in Indonesia.
The recruitment and retention rates (75% and 89%) in our study are consistent with rates observed in studies conducted in high-income country settings (ranging from 76.5% to 97%).11,15,37 Adherence to resistance exercise in this study (78%) was considered high, supported by a previous review suggesting 71%–88% as high adherence levels for home-based aerobic and resistance intervention in HICs. 16 However, adherence to the aerobic program (53%) was lower than other walking-based interventions,38,39 but followed similar trends as found by Pinto et al., 40 where walking was highest in the first 4 weeks of the intervention and then declined until week 12 due to the increased exercise targets and a reduction in its novelty over time. Previous studies found that education level, BMI, history of multimodal treatment, and physical fatigue were predictors of adherence rate41,42 even though our analyses revealed no association between participants’ characteristics and adherence rate. However, Witlox et al. 41 supported that possible predictors of adherence were not identical across the study population. Our study, as reported elsewhere in the literature, highlights the acceptability of home-based exercise programs during the treatment for BC.43,44 Participants reported that exercises were easy and enjoyable. Overall, the absence of serious adverse events in the present study indicates that home-based aerobic and resistance exercise have an acceptable safety profile. Whilst five patients (13.9%) reported myalgia after participating in resistance exercise, its reported prevalence in this study aligns with similar studies (13.3% and 16.1%).20,45 While myalgia can be caused by caused by unaccustomed exercise 46 and is a common side effect of endocrine treatment. 47 Future research should investigate pain exacerbation with exercise in patients receiving endocrine treatment who have not previously performed resistance exercise.
Our study expands on previous research by exploring the feasibility and acceptability of a home-based exercise program in the context of an LMIC setting and provides new insight into women’s cognitive and emotional responses to an intervention delivered by healthcare professionals in Indonesia. In this study, we found that home-based aerobic and resistance exercise is acceptable, with perceived benefits (including improved physical fitness, arm strength and movement, and psychological well-being), goal-setting, and reassurance feeling as the major enabling factors. On the contrary, we found pain experienced during and after exercising as a barrier that led to low intervention adherence. The inclusion of participant interviews provides insights into the mechanisms that may be underpinning the emotional experience of engaging with exercise, and participants’ perceptions of the burden and effectiveness associated with the intervention. Strategies to mitigate barriers (e.g., offering individualized types of therapeutic exercises) and maintain or enhance participation in exercise are needed in future work to improve adherence and increase intervention uptake.48,49
The home-based aerobic and resistance exercise was beneficial, demonstrating a remarkable increase in the predicted
The UK Medical Research Council intervention development framework consists of four phases to increase the uptake of successfully tested interventions, 53 namely intervention development, feasibility, evaluation, and implementation order. Our study assessed intervention feasibility and acceptability at the patient level and suggested that different outcomes are probably associated with the participant’s physical fitness level at baseline and total exercise dose. Intervention refinement after confirming the dose-response interaction, acceptability from the provider level, and cost considerations are essential before testing the intervention in the evaluation phase. Continuous evaluation before incorporating an intervention into routine care is needed since other BC populations in different hospitals or regions may have different acceptability rates, barriers, or enabling factors. Effective implementation also requires rehabilitation professionals training, public awareness education, and collaboration with other institutions or hospital to facilitate knowledge and resource transfer. 36
This is the first study that evaluates the feasibility and acceptability using theoretical framework analysis on home-based exercise intervention in LMICs. Previous studies in India 54 and Indonesia 55 did not report feasibility data. Measuring and reporting the implementation outcomes are important to maximize the use and impact of an intervention study in real-world setting.35,53 This study has already used mixed methods study to measure feasibility, acceptability, and preliminary effectiveness that reflect intervention appropriateness. 35 Additionally, a predictive submaximal treadmill test was used to assess aerobic capacity, which was perceived to be safer compared to field-based tests and timed up-and-go test 56 and more convenient compared to a cycle ergometer. 57 The modified Bruce treadmill test that we used has proven valid. 58 Furthermore, our study combined aerobic and resistance exercise in a home-based setting and demonstrated a positive effect on the aerobic capacity outcome. Most previous studies have adopted a single training modality, mainly aerobic exercise.55,59,60
Our study has limitations. First, even though implementing home-based exercise intervention was novel for Indonesian BC patients, as well as other LMICs, this kind of study was already conducted mainly in HICs.11,15,26,39,45 In addition, other studies incorporated other aspects alongside exercise intervention, such as nutritional and psychological education, 61 or assessed different outcomes, for example, lymphedema. 62 Second, a self-reported diary was used to capture patients’ adherence that may have introduced recall bias with consequential over- or under-reporting. 58 Weekly phone calls to monitor and document self-reported data from the prior week were conducted to minimize this bias. This study lacked a resistance test despite the use of a combined aerobic and resistance exercise intervention. Handgrip strength, one-repetition maximum, and multiple repetition test are commonly used evaluation methods in resistance exercise 25 , but appropriate equipment and gym facilities were not available to implement these measures. Lastly, even though we already incorporated some implementation outcomes, we have not analyzed the intervention acceptability beyond the patient level, the degree of intervention adoption, and cost-effectiveness. 35 Future studies need to address these concerns to promote home-based aerobic and resistance exercise implementation into cancer routine care in Indonesia.
Conclusion
This first study to implement a home-based combined aerobic and resistance exercise intervention in BC care in Indonesia demonstrates its feasibility, acceptability, safety, and preliminary effectiveness. Our work has begun to identify mechanisms that may be influencing the positive outcomes experienced by participants, but further intervention mapping and testing are required to support its development and understand its delivery and performance when tested in additional sites. Future research is required to determine appropriate approaches to tailoring the content of aerobic and resistance exercise programs in response to baseline levels of physical fitness to avoid ceiling effects.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241272706 – Supplemental material for Feasibility, acceptability, and preliminary effectiveness of implementing a 12-week home-based aerobic and resistance exercise program for breast cancer patients receiving endocrine treatment in Indonesia: A mixed methods study
Supplemental material, sj-docx-1-smo-10.1177_20503121241272706 for Feasibility, acceptability, and preliminary effectiveness of implementing a 12-week home-based aerobic and resistance exercise program for breast cancer patients receiving endocrine treatment in Indonesia: A mixed methods study by Yufi Kartika Astari, Susanna Hilda Hutajulu, Yayi Suryo Prabandari, Bagas Suryo Bintoro, Rakhmat Ari Wibowo, Mardiah Suci Hardianti, Anggoro Budi Hartopo, Katie M Di Sebastiano, Matthew John Allsop and Shaunna Burke in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241272706 – Supplemental material for Feasibility, acceptability, and preliminary effectiveness of implementing a 12-week home-based aerobic and resistance exercise program for breast cancer patients receiving endocrine treatment in Indonesia: A mixed methods study
Supplemental material, sj-docx-2-smo-10.1177_20503121241272706 for Feasibility, acceptability, and preliminary effectiveness of implementing a 12-week home-based aerobic and resistance exercise program for breast cancer patients receiving endocrine treatment in Indonesia: A mixed methods study by Yufi Kartika Astari, Susanna Hilda Hutajulu, Yayi Suryo Prabandari, Bagas Suryo Bintoro, Rakhmat Ari Wibowo, Mardiah Suci Hardianti, Anggoro Budi Hartopo, Katie M Di Sebastiano, Matthew John Allsop and Shaunna Burke in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121241272706 – Supplemental material for Feasibility, acceptability, and preliminary effectiveness of implementing a 12-week home-based aerobic and resistance exercise program for breast cancer patients receiving endocrine treatment in Indonesia: A mixed methods study
Supplemental material, sj-docx-3-smo-10.1177_20503121241272706 for Feasibility, acceptability, and preliminary effectiveness of implementing a 12-week home-based aerobic and resistance exercise program for breast cancer patients receiving endocrine treatment in Indonesia: A mixed methods study by Yufi Kartika Astari, Susanna Hilda Hutajulu, Yayi Suryo Prabandari, Bagas Suryo Bintoro, Rakhmat Ari Wibowo, Mardiah Suci Hardianti, Anggoro Budi Hartopo, Katie M Di Sebastiano, Matthew John Allsop and Shaunna Burke in SAGE Open Medicine
Supplemental Material
sj-docx-4-smo-10.1177_20503121241272706 – Supplemental material for Feasibility, acceptability, and preliminary effectiveness of implementing a 12-week home-based aerobic and resistance exercise program for breast cancer patients receiving endocrine treatment in Indonesia: A mixed methods study
Supplemental material, sj-docx-4-smo-10.1177_20503121241272706 for Feasibility, acceptability, and preliminary effectiveness of implementing a 12-week home-based aerobic and resistance exercise program for breast cancer patients receiving endocrine treatment in Indonesia: A mixed methods study by Yufi Kartika Astari, Susanna Hilda Hutajulu, Yayi Suryo Prabandari, Bagas Suryo Bintoro, Rakhmat Ari Wibowo, Mardiah Suci Hardianti, Anggoro Budi Hartopo, Katie M Di Sebastiano, Matthew John Allsop and Shaunna Burke in SAGE Open Medicine
Supplemental Material
sj-docx-5-smo-10.1177_20503121241272706 – Supplemental material for Feasibility, acceptability, and preliminary effectiveness of implementing a 12-week home-based aerobic and resistance exercise program for breast cancer patients receiving endocrine treatment in Indonesia: A mixed methods study
Supplemental material, sj-docx-5-smo-10.1177_20503121241272706 for Feasibility, acceptability, and preliminary effectiveness of implementing a 12-week home-based aerobic and resistance exercise program for breast cancer patients receiving endocrine treatment in Indonesia: A mixed methods study by Yufi Kartika Astari, Susanna Hilda Hutajulu, Yayi Suryo Prabandari, Bagas Suryo Bintoro, Rakhmat Ari Wibowo, Mardiah Suci Hardianti, Anggoro Budi Hartopo, Katie M Di Sebastiano, Matthew John Allsop and Shaunna Burke in SAGE Open Medicine
Footnotes
Acknowledgements
We are grateful to Norma Dewi Suryani, Refdiana Dewi, Riani Witaningrum, Anton Sudiyanto, Fahmi Baiquni, and Juan Adrian Wiranata for technical assistance. We also gratefully thanked our cardiac rehabilitation nurses, Endang Warijanti and Diah Perwitasari.
Availability of data and materials
The data sets analyzed in the current study are accessible from the corresponding author on fair request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by University of Leeds (2021); The Indonesian Ministry of Research, Technology and Higher Education (grant number 1951/UN1/DITLIT/Dit-Lit/PT.01.03.2022, 2022); and Universitas Gadjah Mada (grant numbers 348/UN1/FKKMK/PPKE/PT/2022 and 3550/UN1.P.III/Dit-Lit/PT.01.05/2022, 2022). All funders did not play any role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethics approval
Ethical approval for this study was obtained from the Medical and Health Research Ethics Committee, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia (reference number KE/FK/0184/EC/2021).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.