
Abstract
Background:
Due to the high sensitivity of their growing tissues to ionizing radiation, pediatric patients are at a greater risk of cancer development.
Objective:
This study aimed to evaluate the level of radiation exposure experienced by pediatric patients undergoing a common CT examination at the three government hospitals in Addis Ababa, Ethiopia.
Materials and methods:
Structured formats were designed for data collection at three government hospitals, and then information about pediatric patients’ demography, CT protocols, and CT systems was retrieved and recorded from March 2018 up to July 2018. CT dose indicators: CTDIvol (mGy) and DLP (mGy.cm) values for abdomen, chest, and head CT scans were recorded based on pediatric patients’ age ⩽1, (1–5], (5–10], and (10–15] years old. The data were analyzed through SPSS version 25 software. Finally, the third quartile values of CTDIvol and DLP were determined and compared with other international DRLs.
Results:
The third quartile values of radiation dose descriptors for abdomen, chest, and head CT scans, respectively, in terms of CTDIvol (mGy): 58, 10, 17, 51; 23, 23, 34, 51; 62, 41, 50, 51; and in terms of DLP (mGy.cm), 377, 314, 624, 664; 523, 571, 406, 739; 927, 806, 929, and 1197 corresponded to pediatric patients of age ⩽1, (1–5], (5–10], and (10–15] years old, respectively.
Conclusion:
There were significant differences in the radiation dosage of some CT examinations between the same age groups, indicating a need for dose optimization. Therefore, this study recommends the need for enhancing radiation safety, ensuring appropriate imaging practices, and prioritizing the well-being of pediatric patients who visit CT examinations in Addis Ababa, Ethiopia.
Introduction
Despite advances in medical imaging’s ability to diagnose and treat a variety of medical problems in children, radiation exposure, particularly with computed tomography, remains a concern for children, who are more susceptible to radiation-related cancer development than adults. 1 A study showed that the radiation risk from CT is highest in diagnostic imaging, accounting for up to 67% of all radiation. 2 Consequently, the increased use of pediatric CT is particularly concerning because children are estimated to be 10 times more radiosensitive than adults. 3 Ionizing radiation’s mutagenic effect is particularly sensitive in growing tissues. 4 The younger the child, the larger the number of growing cells.
Children, compared to adults, are thought to be at a greater risk of acquiring cancer from ionizing radiation, owing to their enhanced radio sensitivity and longer life span following exposure. 5 According to the current risk assessment, the chance of getting a solid tumor following radiation exposure is approximately three times greater for a 1-year-old kid and 1.8 times greater for a 10-year-old child compared to adults. 6 The probable chance of acquiring radiation-induced cancer, which has been estimated to be 5% per Sv at all ages, increases dramatically to 15% if a person is exposed in the first decade of life. 7
When a CT scan is performed under proper clinical guidance that combines the radiation protection concepts of justification and optimization, a procedure requiring radiation exposure will result in a net patient benefit. 8 Research conducted in Finland to investigate the occurrence of inappropriate CT imaging in younger patients discovered that around 30% of all exams were unreasonable. 9
As a result, CT protocol optimization is critical, especially for children, who are more radiosensitive than adults. 10 A study indicated that a lack of information about certain imaging modalities, as well as the use of imaging instead of sufficient clinical assessment (due to time constraints), may lead to incorrect CT use. 11 The primary goal of this research was to assess radiation doses delivered to pediatric patients referred for CT imaging at TASH, Saint Paul Millennium Medical College (SPMMC), and Yekatit 12 Hospital Medical College in Addis Ababa, Ethiopia.
Materials and methods
Study design
A retrospective hospital-based cross-sectional study was conducted between March 2018 and July 2018 on pediatric patients referred for CT imaging at TASH, SPMMC, and Yekatit 12 Hospital Medical College in Addis Ababa, Ethiopia. These hospitals were selected due to their high patient flow.
Sample size and sampling techniques
This study was carried out in three government hospitals in Addis Ababa, Ethiopia, on 302 pediatric patients who had CT examinations of their heads, chests, and abdomens. The study utilized a purposive sampling technique, and the sample size was established by consulting the guidelines for conducting such a study provided by ICRP 135 13 recommendations to conduct such a study.
Data collection
In this study, standardized data collection templates containing patient demography, CT scan parameters, and CT dose descriptors that are in line with the reports of Verdun et al. 10 and Eddy et al. 12 were prepared and utilized. All pediatric patients who were ⩽15 years old with a CT request form evaluated for justification or documented CT acquisition parameters and radiation dose reports for those justified for imaging were included in the study. Pediatric patients were categorized into four age groups: ⩽1, (1–5], (5–10], and (10–15] years old. Based on the research objectives and variables of interest, relevant information was obtained from medical radiological records retrospectively. Data were gathered from past records and images of patients who had previously undergone CT examinations. Data about patient profiles, CT scan parameters, and CT dose indicators from the existing records were collected without the need for new scans or patient interactions.
The study only included pediatric patients who had a CT examination (with or without contrast agent) of the head, chest, and abdomen and whose diagnostic results had been approved by the radiologists at each data source. However, perfusion investigations and CT urography were considered non-frequent CT examinations and excluded from pediatric dose data. Moreover, numerous dose reports on the same pediatric patient and incomplete dose records were ignored from consideration. The values of CT dose descriptors CTDIvol (mGy) and DLP (mGy.cm) were retrieved and recorded from the CT scan console in each data source hospital.
Ethics approval
The Research and Publication Committee of the Department of Radiology, College of Health Sciences, Addis Ababa University, granted ethics approval, with permission number AAURD/159/018. Any piece of patient information was kept confidential by maintaining the anonymity of the study subjects.
Informed consent
The Research and Publication Committee of the Department of Radiology, College of Health Sciences, Addis Ababa University, waived the necessity of informed consent because the data used in the study are anonymous and cannot be traced back to individual participants.
Statistical analysis
In this study, computerized data analysis was conducted using SPSS version 25 software. The recorded values of CTDIvol (mGy) and DLP (mGy.cm) per pediatric age group and CT scan type were coded and entered into SPSS software. The third quartile values were determined from the median distribution values of CTDIvol (mGy) and DLP (mGy.cm) in each anatomical region and each pediatric age group. Finally, the third quartile values of this study were compared with other similar international studies.
Results
Of the total of 302 pediatric patients, 192 (63.6%) were males and 110 (36.4%) were females. The age distribution of the request form showed that 38 (12.6%) were ⩽1 year old, 60 (19.9%) were in the (1–5] year group, 75 (24.9%) were in the (5–10] year group, and 129 (42.7%) were in the (10–15] year group (see Figure 1).

The distribution of pediatric CT performed in each anatomical region.
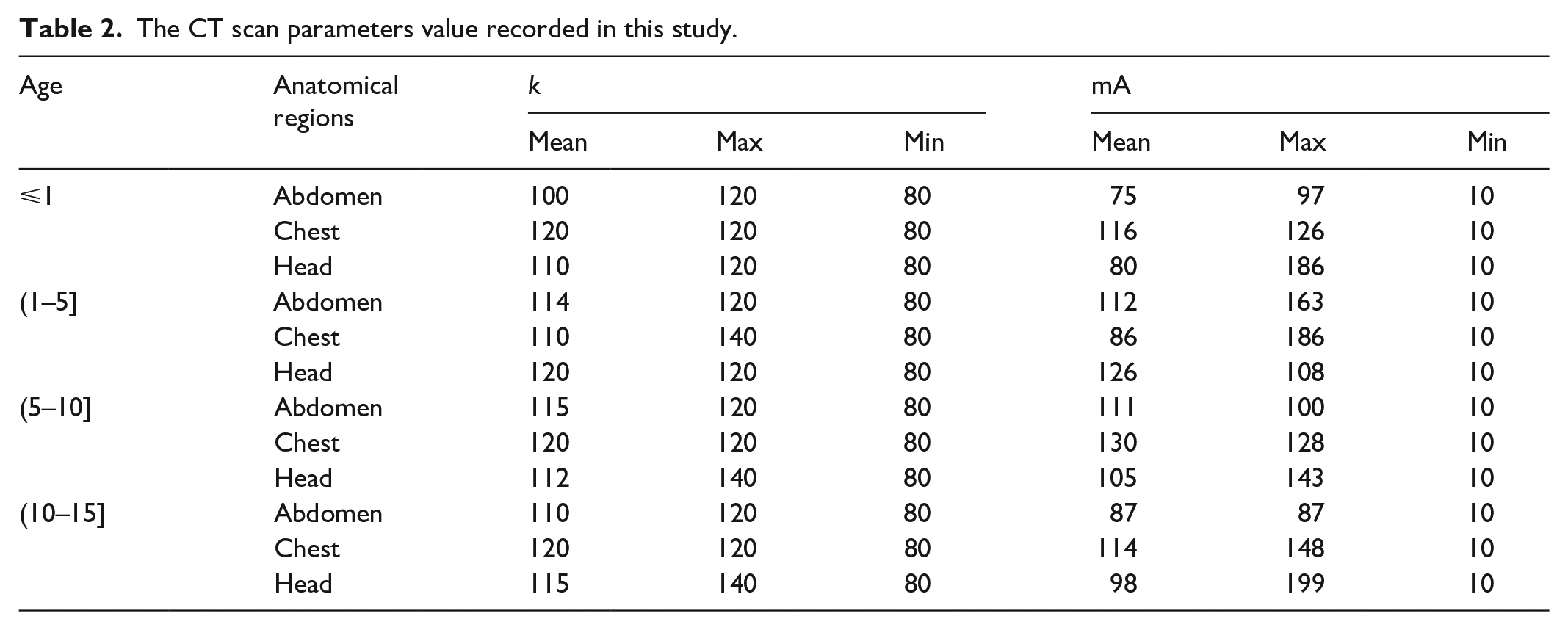
Out of all the instances, 63.66% used a tube voltage of 120 kV, 31.96% applied a protocol of 100 kV, 8 (2.65%) patients had a kV value of 140, and 2.06% employed a low protocol of 80 kV. Table 1 shows patients’ demographic data. Table 2 shows the statistical data for mA and kV. Table 3 displays the third quartile values acquired for each age group and anatomical region in this investigation. The comparison of the determined third quartiles obtained from CTDIvol (mGy) for head, chest, and abdomen CT was expressed in Figures 2–4, respectively. Finally, a comparison of the third quartile values obtained from DLP (mGy.cm) for head, chest, and abdomen CT was expressed in Figures 5–7, respectively.
Patients’ demographic data of this study.

The CT scan parameters value recorded in this study.
The third-quartile value of CTDIvol (mGy) and the DLP (mGy.cm) investigated in this study.

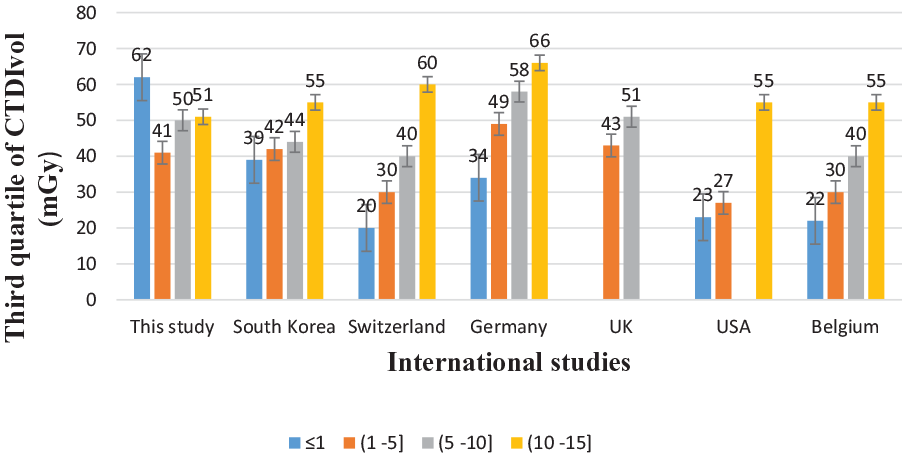
A comparison of the third quartile of CTDIvol for head CT in this study with other similar studies that proposed DRLs.

A comparison of the third quartile of CTDIvol for chest CT in this study with other similar studies that proposed DRLs.

A comparison of the third quartile of CTDIvol for abdomen CT in this study with other similar studies that proposed DRLs.
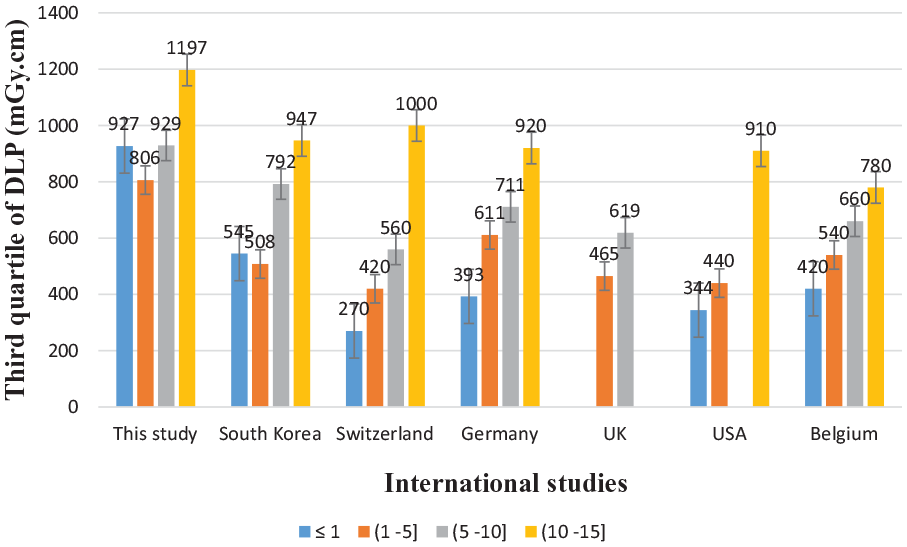
A comparison of the third quartile of DLP for head CT in this study with other similar studies that proposed DRLs.

A comparison of the third quartile of DLP for chest CT in this study with other similar studies that proposed DRLs.

A comparison of the third quartile of DLP for abdomen CT in this study with other similar studies that proposed DRLs.
Discussion
In this study, most of the CT requests were for the head: 150 (49.7%), followed by the abdomen: 79 (26.2%) and the chest: 73 (24.2%), which were more or less comparable with a similar study of the IAEA Survey of Pediatric CT Practice in 40 less-resourced countries, which showed head CT as the most common CT examination in children, amounting to nearly 75% of all pediatric CT examinations 14 (see Figure 1).
The higher frequency of head CT examinations in this study compared with chest and abdomen CT examinations is also similar to the global trend reported by the United Nations Scientific Committee on the Effects of Atomic Radiation, in which the data were largely obtained from developed countries. 15 The mean (kV and mA) protocols used for pediatric patients (age ⩽ 15) were 110, 118, 114 kV; 96, 111, and 102 mA for abdomen, chest, and head CT scans, respectively (see Table 1).
The investigated third quartile values of CTDIvol (mGy) and DLP (mGy.cm) showed that pediatric patients (age ⩽ 1 year old) were exposed to higher radiation doses in each anatomical region, particularly in chest CT scans. As seen in Figure 3, the third quartile value of the CTDIvol (mGy) of chest CT in this age group was almost 5 times, 10 times, and 20 times higher than the CTDIvol (mGy) found in Switzerland, 10 the USA, 16 and Belgium, 17 respectively.
Similarly, the third quartile value of DLP (mGy.cm) in this study was higher by far, which was 10-fold and 20-fold higher than the DRL values reported in South Korea 12 and Belgium 17 respectively, see Figure 6. In addition, the investigated third quartile values of CTDIvol (mGy) and DLP (mGy.cm) for all age groups were higher than the reports in Germany, 18 Japan, 19 and Hawassa. 20 This is due to the fact that the higher kV value used can yield a higher radiation dose. 21
For a head CT scan, the determined third quartile values of CTDIvol (mGy) for three pediatric age groups were comparable to other international DRL values: Switzerland, 10 Germany, 22 South Korea, 12 the USA, 16 and Belgium. 17 The obtained third quartile value of CTDIvol (mGy) for pediatric patients (age ⩽ 1 year old) was nearly threefold the reported value in Switzerland, 10 the USA, 16 and Belgium, 17 see Figure 2. Similarly, for pediatric patients (ages (1–5] years old), the investigated third quartile value of DLP (mGy.cm) was threefold and twofold the reported values in Switzerland and Germany, respectively (see Figure 5). Moreover, the results of this study were higher than the reported values in Germany, 18 Japan, 19 the USA, 16 and Belgium. 17
For the abdomen CT scan of pediatric patients, huge variations in the third quartile values of CTDIvol (mGy) were also observed. For pediatric patients (age ⩽ 1 year old), the investigated third quartile value (58 mGy) was nearly 30-fold the reported DRL in the USA. Also, variations in the third quartile of CTDIvol (mGy) for pediatric patients of age grouped as ⩽1 and (10–15] were investigated with the reports of Germany, South Korea, Switzerland, Belgium, Japan, and Hawassa. However, for pediatric patients aged between 1 and 10 years old, their third quartile values of CTDIvol (mGy) were comparable to the reports of others (see Figure 4).
For the pediatric patients (age ⩽ 1 year old), the obtained third quartile value of DLP was sixfold and threefold higher than the reported values in Belgium and Switzerland, respectively. However, the obtained third-quartile values of DLP for pediatric patients aged between 1 and 15 were comparable to the reported values in South Korea, Switzerland, and Germany (see Figure 7).
Generally, when compared with other international studies, 23 Germany, and Japan, large variations in the third quartile values of CTDIvol (mGy) and DLP (mGy.cm) for chest CT, abdomen CT, and head CT scans were observed, respectively. Significant variation in radiation doses among pediatric patients was observed. Therefore, an optimization process should be initiated to reduce this higher radiation dose, and a consensus on DRLs should be maintained. Lowering the kVp can limit the radiation output of the CT scanner and can be a suitable choice for lowering the radiation dose, according to a survey done at South Korean hospitals to optimize the radiation dosage for pediatric CT scanning. 24 ICRP suggested that 100 kV can be used in the routine for children weighing between 5 and 50 kg. 25 In addition to this, lowering the kV from 120 to 80 decreases the dose delivered by half; choosing a relatively low value (80 kV for neonates) should be favored. 26 However, a maximum peak tube voltage of 140 kV was observed in this study.
Energy consumption in CT imaging can be impacted by the scan methods selected. 27 Scan periods can be shortened, and needless radiation exposure can be avoided by optimizing scan parameters according to the medical indication. Clear images obtained through well-optimized scan techniques may improve radiologists’ assessments. 28 Pitch, slice thickness, and reconstruction techniques are examples of scan parameters that can be changed to enhance image quality and diagnostic precision. Accurate diagnosis can be aided by improving visualization of vascular structures and lesions with appropriate contrast agent delivery and scan timing.29,30
The kilo voltage (kV) settings used in CT imaging affect the ratio of photoelectric absorption to Compton scattering. Higher kV settings decrease photoelectric absorption and increase the frequency of Compton scattering interactions. 31 Therefore, when adjusting the kV settings, the radiologist and radiology technologists should consider the imaging requirements, the patient’s body composition, and the desired ratio of contrast to image noise.
This study has some limitations. First, the study was conducted at three government hospitals in Addis Ababa. A multi-center study involving a broader range of healthcare facilities could enhance the study’s external validity. Second, the study focused on CT imaging in pediatric patients for abdomen, chest, and head examinations. Including other types of imaging in a region of interest could provide a more comprehensive assessment of radiation exposure. Third, data about the weight and height of pediatric patients were not available in the medical radiology database system; as a result, the study was obliged to exclude these CT scan parameters that could provide valuable insights into radiation exposure assessments.
Conclusion
The findings of this study implied that pediatric patients were exposed to high radiation doses. Particularly, pediatric patients (age ⩽ 1) were exposed to high radiation burdens. This finding is likely to contribute valuable insights into the current state of radiation exposure among pediatric patients undergoing CT imaging in government hospitals in Addis Ababa, Ethiopia. The investigated third quartile values of this study showed standardization and optimization within the departments for subsequent measurements should be taken.
In addition, a similar kind of extensive survey ought to be conducted to determine national DRLs for pediatric computed tomography examinations. Generally, protecting pediatric patients from unnecessary diagnostic radiation doses should be the primary goal of radiation experts who work in these hospitals. Therefore, adopting local diagnostic reference levels should be practiced until national DRL values are prepared.
Footnotes
Acknowledgements
We great fully acknowledge the hospitals that participated in this study and the radiology technologists for their cooperation during the data collection process.
Author contribution
AF and ST contributed to the data analysis, interpretation, and preparation of the manuscript; AN collected the data; and TK and YG evaluated the CT request form for justification. All authors reviewed the results and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Research and Publication committee of the Department of Radiology College of Health Sciences Addis Ababa University granted ethics approval with permission number AAURD/159/018. Any piece of patient information was kept confidential by maintaining the anonymity of the study subjects.
Informed consent
The Research and Publication committee of the Department of Radiology College of Health Sciences Addis Ababa University waived the necessity of informed consent because data used in the study are anonymized and cannot be traced back to individual participants.
Trial registration
Not applicable.