
Abstract
Objectives:
Health hazards such as adverse drug reactions and prolonged morbidity are fallouts of self-medication among young people in sub-Saharan Africa. The aim of this study was to assess the prevalence, practice, determinants, and adverse effects of self-medication among young people living in a suburban community of Ekiti, Nigeria.
Methods:
This survey was a descriptive, cross-sectional study of 602 young people aged 16–24 years., who were randomly selected in the community. A predesigned self-administered questionnaire was used for data collection. The study was conducted from 1st March to 31st May 2023. The independent variables measured include the sociodemographic characteristics, while the dependent variables are the practice of self-medication and factors that predisposes to self-medication. The general characteristics of the participants were analyzed using descriptive statistics. The categorical variables were reported as frequency distribution and proportions with 95% confidence intervals and were compared using the Chi-square test or Fisher’s exact test. A p-value of <0.05 was considered statistically significant.
Results:
Over 30% (31.7%) of the participants engage in self-medication. A larger proportion of the people who practiced self-medication lived a trekking distance of less than 1 km from the nearest health facility with a doctor (p = 0.044). The practice of self-medication was statistically related with being a student when compared with gainfully employed and unemployed people (p = 0.006). Fever (39.8%), abdominal pain (17.3%) and headaches (16.2%) were the topmost three ailments that necessitated self-medication. Antimalarials (44.0%), antibiotics (25.1%), and antipyretics (16.8%) were high on the list of drugs used for self-medication. Headache (34.0%) was the most common adverse reaction from self-medication among the participants studied.
Conclusion:
Adverse reactions and drug addiction were negative fallouts of self-medication, which can affect the health of young people as they grow into adulthood. Therefore, monitoring of drug outlets must be taken seriously by government agencies to prevent the worsening of the negative effects of self-medication.
Introduction
Self-medication is the use of one or more drugs that are not prescribed by a physician or controlled by medical health organization. 1 This includes herbal or chemical medications, previously prescribed medicine for similar cases, extra medicines at home, or not using medicine completely. 2 It also involves the sharing of previously prescribed medicines with relatives, friends, or members of one’s social circle or the use of leftover medicines stored at home. 3 Some of these drugs are used indiscriminately as long as the perceived symptoms are not abating thus leading to misuse and abuse of such. Such abuse and misuse could mask underlying symptoms and signs hence complicating the medical condition(s) leading to drug resistance and possibly delayed diagnosis. 4
Worldwide, self-medication is a public health challenge and is common in developing countries.5,6 The prevalence of self-medication among Northern Indian adults was 66.4%. 7 Among the Indians, convenience and lack of time were the topmost reasons why they self-medicate. 7 Among the adult population of Bangladesh, it was reported that about 41.5% and 61.8% were involved in the practice from studies in Chattogram and Thimphu, respectively. 8 Participants from these two cities cited lack of perceived seriousness of the disease and no hospitals in nearest places as reasons for self-medication. 8 In Nigeria, while about 41% of the population was reported to be involved in self-medication during the COVID-19 pandemic, the commonest reason for self-medication was fear of stigmatization and discrimination. 9 This has been attributed to increased uncontrolled availability of drugs usage without prescription in these countries. 10 Other reasons that have been reported as reasons for self-medication include convenience, lack of time and cost saving. 7
Most times, these self-medicated drugs are gotten over the counter either from drug shop owners, who administer pharmaceutical products from chemists and pharmacy outlets within the community otherwise known as community pharmacies. 11 In Nigeria, these vendors are known as Patent and Proprietary Medicine Vendors (PPMVs). 12 Although they lack formal pharmacy training, but in order to achieve Universal Health Coverage in Nigeria, the PPMVs are registered and regulated by the Pharmacy Council of Nigeria to sell orthodox pharmaceutical products for common illnesses on retail basis to Nigerian populace. 12
Problems associated with self-medication range from irrational use of drugs, wastage of health resources, and increased resistance of pathogens to antimicrobials. 13 Others are serious health hazards such as adverse drug reactions and prolonged morbidity. 13 In spite of these hazardous consequences of self-medication, the practice is common in many countries including Nigeria.10,13–16 Adolescents and young people are a group of people who are prone to self-medication because of their poor risk perception about drug usage, and easy access to social media and internet facilities where unverified information about medical conditions often influences their actions.17,18 They are also prone to this practice because of the ready access to over-the-counter medications, and their level of education with increased proliferation of topics on health-related issues on media platforms. 18 Easy access to roadside drug hawkers and patent medicine stores has been associated with the practice of self-medication in this age group, especially in low and middle-income countries.19,20
Some previous studies concentrated on the self-medication practice among adults in the general population.8,21,22 However, there is paucity of information on self-medication among young people in a developing country like Nigeria. Having baseline information about the practice and determinants of self-medication among this age group is vital to the development of necessary interventions. This study therefore assessed the prevalence, practice, determinants, and adverse reactions of self-medication on the health of young people living in a suburban community of Ekiti, Nigeria.
Methods and materials
Study design
This was a descriptive, cross-sectional study of prevalence, determinants, practice, and adverse effects of self-medication conducted among young people living in a suburban community of Ekiti State, South-West Nigeria.
Study area
Iworoko Ekiti is a community populated majorly by students of a government-owned tertiary institution in Ekiti State. The population of the town was classified into four; farmers, artisans, civil servants, and students (essentially students of Ekiti State University (EKSU)). Ekiti State University is located in the neighborhood of Iworoko Ekiti. The university is about 15 km from the state capital Ado Ekiti and less than 1 km from Iworoko Ekiti thus making it the closest community to the students. 23 Many students live in the town because of the limited accommodation within the university campus. 23 There are two major streets that branched off from the major road that traversed the town.
Inclusion criteria
Young people aged 15–24 living in this area were randomly approached by researchers to fill the predesigned questionnaires on self-medication. Consenting participants who met the inclusion criteria over a three-month period from 1st March to 31st May 2023 were enrolled in the study.
Exclusion criteria
Young people who lived in the area for less than 1 year or were severely disabled were excluded from the study.
Sampling size and technique
Sample size was calculated using the formula; n = (Zα)2 p q/d2, where p = 53.1% (the proportion of the target population estimated to have practiced self-medication according to a previous study done in the University of Ghana). 24 A minimum sample size of 383 was arrived at. A total of 660 questionnaires was distributed out of which 602 were completely filled. This was based on previous study that stated the high possibility of low response rate among similar age group. 11 The questionnaires were distributed to as many as met the inclusion criteria through simple random technique.
Study instrument
The instrument was developed from existing literature on self-medication among young people.5,6,13–16,25 The questionnaire consists of three segments: the first segment consists of socio-demographical information about the respondents, section B includes questions assessing self-medication practices and section C assessed the health status of the participants. Face and content validity were done by two specialists in Family Medicine and Clinical Pharmacology departments to ascertain the inclusiveness of the questions in the questionnaire with respect to the objectives of the study. A pretest of the questionnaire was done with 50 young people (which amount to less than 1% of the total population) among students among students of a polytechnic in a nearby town to rule out any misleading or confusing questions. The instrument was then revised based on the pretest outcomes before being administered. To evaluate the reliability of the questionnaire, 20 students of the College of Nursing Sciences, Ekiti State University Teaching Hospital (EKSUTH) had the questionnaires administered to them on two different occasions with an interval of 1 month which showed moderate-to-high reproducibility.
Data collection
Self-administered questionnaires were administered to consenting young people, who resides within the study area. The respondents were assured of confidentiality and to guarantee response anonymity, their names and addresses were excluded from the questionnaires. In order to prevent multiple filling of the questionnaires and duplication, each questionnaire was coded to differentiate the major streets from each minor arterial streets where the participants reside. Participants who were 18 years and above filled and signed the consent form. Accent was obtained from those who were less than 18 years and written informed consent was obtained from their parents or guardian or legally authorized representative before these participants had the questionnaires administered to them. All the participants had formal education and could read and write.
Variables studied
The sociodemographic characteristics (age, gender, highest educational status, socioeconomic status of the family, and mother’s highest educational level) of the respondents were considered the independent variables while self-medication prevalence, practice, and adverse effects were the dependent variables.
Study procedure
Individuals who met the inclusion criteria were randomly approached and written informed consent was obtained from the participants who were 18 years and above before the administration of the questionnaire. Prior to the administration of the questionnaire to the subjects who were less than 18 years old, written informed consent was obtained from their legally authorized representatives. A semi-structured questionnaire was administered to each of the participants and they were encouraged to fill them while the researchers and assistants waited to collect the completed responses. The time frame for administering the questionnaire was an average of about 7–10 min.
Ethical consideration
Written informed consent was obtained from participants who were 18 years and above. Accent was obtained from those who were less than 18 years and written informed consent was obtained from legally authorized representative of the minor subjects before they had the questionnaires administered to them. All the participants had formal education and could read and write. Ethical approval with protocol number EKSUTH/A67/2023/03/005 was obtained from the Ethics and Research Committee of the Ekiti State University Teaching Hospital, Ado Ekiti.
Statistical analysis
The information obtained from the general questionnaire was cleaned, coded, and entered using SPSS version 25 developed by IBM. The general characteristics of the patients were analyzed using descriptive statistics. Demographic variables, which were normally distributed, were described as mean and standard deviation. Categorical variables were reported as frequency distribution and proportions with 95% confidence intervals and were compared using the Chi-square test or Fisher’s exact test as appropriate. Logistic regression was done using the SPSS to determine the predictors of self-medication in the study.
Results
A total of 602 participants completed the questionnaire out of 660 that were administered, 91%.
Sociodemographic characteristics of participants
The mean age of the participants was 21.34 ± 2.00 years. Over 70% were females with close to 90% of them being students. More than three-quarters of them were from low socioeconomic class (Table 1).
Sociodemographic distribution of the participants (N = 602).

Prevalence of self-medication
Over 30% (191, 31.7%) (Figure 1) of the participants engage in self-medication with 81.7% of them in the 20–24 age group (Table 2). More of the participants who were secondary school students (68%) engaged in self-medication.
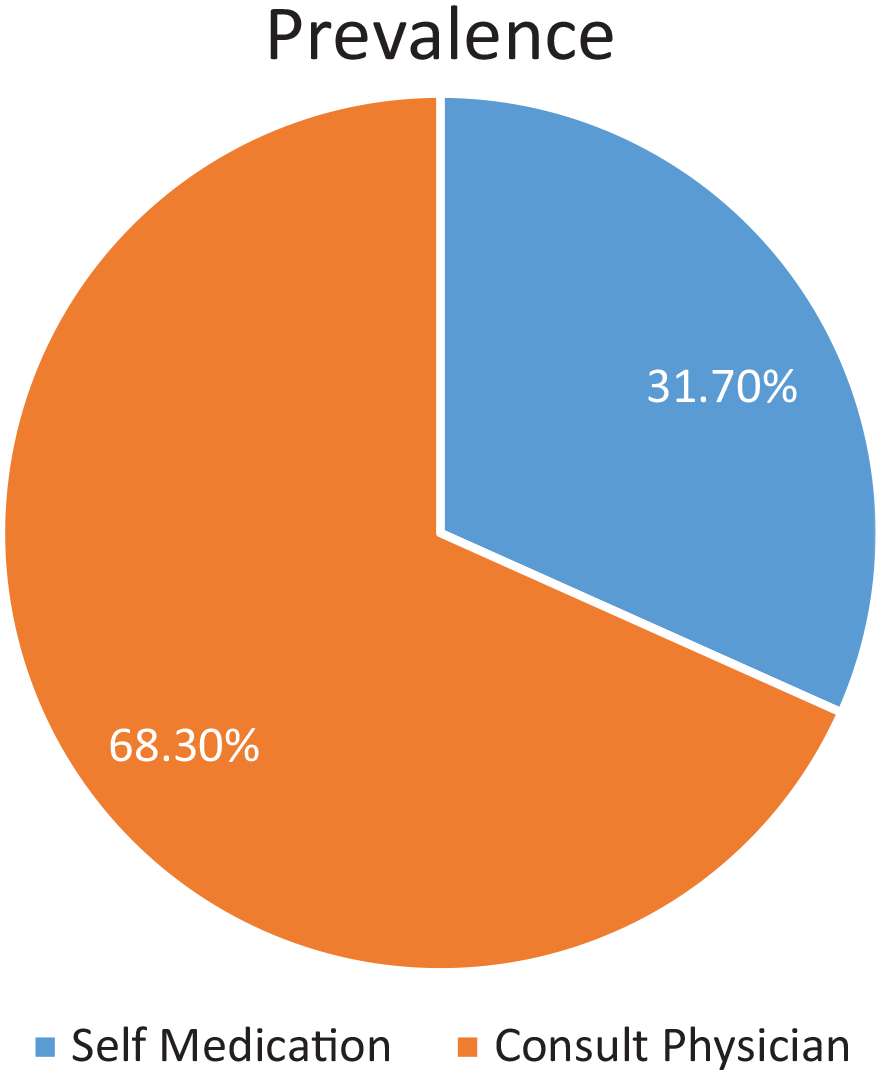
Overall prevalence of self-medication among participants studied.
Sociodemographic characteristics of respondents who practiced self-medication (N = 191).

Determinants of self-medication among the participants studied A larger proportion of the people who practiced self-medication lived a trekking distance from healthcare facility with a doctor when compared with those who usually consult a physician (p = 0.044). Being a student, when compared with gainfully employed or unemployed was also statistically related with the practice of self-medication (p = 0.006) (Table 3).
Determinants of self-medication among participants (N = 602).

Reasons for taking drugs without prescription
The three most common reasons why participants engage in self-medication were minor illnesses, involvement in hectic schedules, and costly doctors’ consultations (Figure 2).

Reasons for self-medication N = 191.
Practices of self-medication among respondents, N = 191
Close to three-quarters (73.8%) of the participants practiced self-medication more than once in the 6 months prior to the study with 8.9% of them visiting a chemist store more than four times within the same duration (Table 4). Fever, abdominal pain and headaches were the most common symptoms that necessitated self-medication (Table 4). Antimalarials, antibiotics and antipyretics were the drugs commonly used for self-medication (Table 4). Headaches, followed by allergic reactions were the adverse reactions experienced by respondents while paracetamol was the drug usually stored at home (Figure 3).
Practices of self-medication among respondents (N = 191).

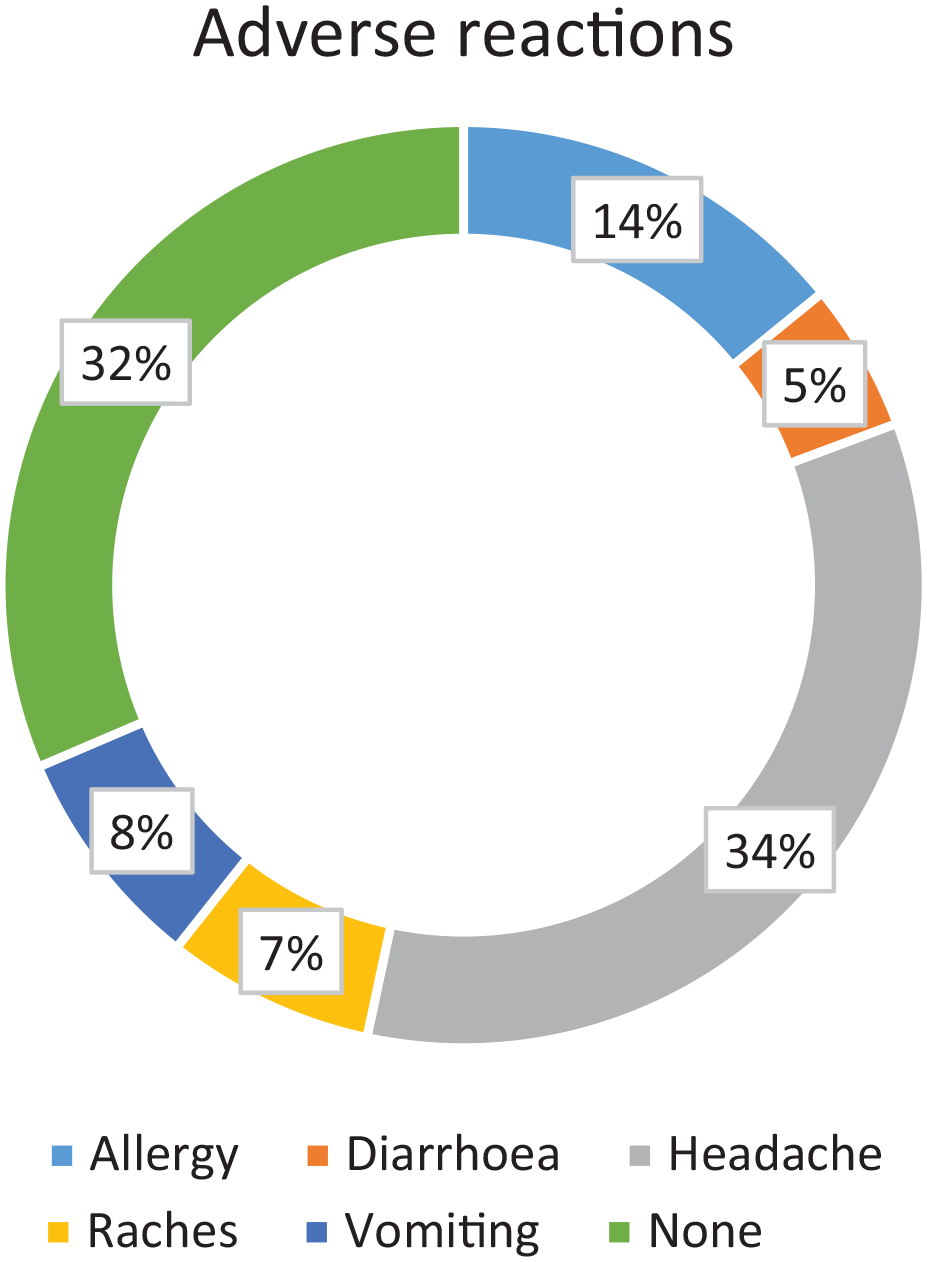
Adverse effects of self-medication from the participants.
History of possible drug dependence among the respondents
About 10% of those who engage in self-medication had history of drug usage which they found difficult to stop.
Relationship between self-medication in previous 6 months and compulsive use of drugs
Over 80% of those who prefer to consult a doctor in the event of a future health challenge were engaged in self-medication when compared to less than 20%, who might prefer to continue self-medication (Table 5).
Relationship between self-medication in previous 6 months and compulsive use of drugs.

Logistic regression showing predictors of self-medication
Logistic regression showing predictors of self-medication was done to control for confounders. Out of all the variables examined for predicting self-medication, low and middle socioeconomic classes were statistically significant with p = 0.026, CI = 1.179–12.734 and p = 0.03, CI = 1.129–10.323 respectively (Table 6). The respondents from low socioeconomic class are 3.9 times more likely to engage in self-medication compared to those from high socioeconomic status (Table 6).
Logistic regression for predictors of self-medication among the participants.

B—values for logistic regression equation for predicting the dependent variable from the independent variable.
Exp (B)—odds ratio.
Sig.—p-values.
Discussion
Prevalence of self-medication
The overall prevalence of self-medication in this study was 31.7% (Figure 1); out of which 156 (81.7%) of them were in the 20–24-year age group and 140 (73.3%) were females (Table 2). This overall prevalence was lower than what was reported among similar age group in some other studies.26–29 However, lower prevalence were reported in Umuahia, Nigeria (30.3%) and Puducherry, India (11.9%),18,30 This difference might be attributable to recall bias from our study participants who needed to response to questions about self-medication in the previous 6 months. The high prevalence in our environment might be related to weak enforcement of legislations against uncontrolled sales of prescribed medications. Poor perceptions of dangers associated with self- medications by the young people, high poverty rate in our country coupled with high rate of paying out of pocket for health expenditures might also be contributory.
Indications and reasons for self-medication
In this study, minor illness (17.8%), hectic schedule (15.7%) and costly doctors’ consultation were the most common reasons why participants engage in self-medication (Figure 2). This is comparable to similar findings of minor ailments like headache, menstrual pain, and cough among undergraduate healthcare students in a Nigerian university as reported by Akande-Sholabi et al. 31 In a similar manner, Kethiswar and Karthik 32 in their study among young adults in India also reported that feverish medical conditions and pain-causing activities as common reasons for engaging in self-medication. Fever (39.8%), abdominal pain (17.3%), and headache (16.2%) were the three most common complaints that necessitated the use of self-medication in this study. This is comparable to reports from some other studies.26,31,33,34 Antimalarials (44.0%), antibiotics (25.1%), and antipyretics (16.8%) were the three groups of medication frequently used in the practice of self-medication in this study. The study location is within a holoendemic malaria region, hence the frequent use of antimalarial drugs. Other studies have also reported that self-medication with antimalarials was common in endemic areas like ours and these were associated with drug resistance, inappropriate treatment, and polychemotherapy. 27,31,35–37
A larger proportion of those who engaged in self-medication lived within a trekking distance (28.8%) from the nearest medical facility (Table 3) when compared to those who consulted a physician for medical health care (19.5%). This showed that there might be other factors influencing the practice of self-medication among this cohort aside from the distance to the health care facility. Abiodun et al. 38 reported that there were some structure and process indicators that influenced the use of health centers among students and staff of a tertiary institution. Participants from low socioeconomic status were about four times more likely to engage in self-medication when compared to those from high social class (Table 3). This is similar to what was reported in some studies where people from lowest income group were more likely to self-medicate when compared to people from high social class.7,39 Possible high cost of hospital bills and high rate of paying out of pocket might be responsible for this finding.
Self-medication practices and adverse reactions
Among those who engaged in self-medication in this study, almost three-quarters of them (73.8%) were involved in the practice more than once in the previous 6 months. In addition to this, close to 10% of them visited the chemist/pharmacy store four or more times within the same period. This is a pointer to how habitual this practice was among the study participants. In this study, four (2.1%) and 13 (6.8%) practiced self-medicated with antitussive and analgesics. Some of these classes of drugs are derived from opioids which may make the body dependent in nature.40–42 Continuous use of these prescription drugs without monitoring has been associated with academic failures, mental health conditions, difficulties in maintaining healthy relationships, and increased physical and sexual assaults. 43
Moreover, about 10% of the participants who practiced self-medication have a history of continuous usage of drugs, which they could not do without. This further buttressed the possibility of drug dependence among these participants. It was reported that self-medication is associated with increased health risk behaviors among young people. 44 This might be a pointer to the possibility of drug dependence as observed in this study with over 40% (40.8%) of those who practice self-medication having history of continuous usage of drugs for over a week. Over 15% (16.8%) of them gave similar history for over a month. Moreover, headaches and allergic reactions were also found to be common adverse reactions to drugs used for self-medication in study participants. While headache might be a continuous symptom of worsening ill health, allergic reaction may be a form of adverse reaction to the used medication. Mwita et al. 35 reported that one of the fallouts of antimalarial self-medication usage is lack of improvement in symptoms while Kassie et al. 45 noted that one of the side effects of self-medication practice is allergy.
Strength and limitation of the study
The strength of the study lies in the use of random sampling technique for data collation, which provides the data analysis done to have a lower risk of error and also guarantees a reduced researcher bias in the study. The limitation of the study lies in the recall bias that is associated with self-reported questionnaires. In addition, the inability to study the behavior of the participants over a period of time also constitutes a limitation. Caution should be exercised in generalizing the findings from this study to the general population because the study area might not be a true reflection of what happens in the community. The reliability analysis of the instrument was not done thus caution is needed when reproducibility of the instrument is concerned.
Conclusion
Minor health challenges, lack of time, or perceived costly consultation of doctor’s consultation were the main reasons for the practice of self-medication in this study. Adverse reactions and potential drug addiction were negative outcomes of self-medication which can affect the health of these young people as they grow into adulthood. Therefore, it becomes imperative that monitoring of drug outlets must be taken seriously by government agencies to prevent the worsening of the negative fallout of self-medication. This study has provided baseline information about the practice and determinants of self-medication among young people which is vital to the development of necessary interventions to curb the menace of this practice.
Recommendation
We recommend further studies to explore the effectiveness of providing free/subsidized health services in the residential area, where young people aggregate and reside. The introduction of community-based health insurance will ameliorate the possible burden of out-of-pocket expenses from these age groups while on campus. Increased public awareness campaigns and education on the danger of self-medication will reduce the negative fallout from self-medication. In addition, relevant government health agencies need to enforce relevant legislative laws to limit the sales of drugs without prescription over the counter. Consequent to the possible high rate of paying out of pocket, enrollment of the populace in health insurance might reduce the practice of self-medication among young people.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241261002 – Supplemental material for Prevalence, practice, determinants and adverse effects of self-medication among young people living in a suburban community of Ekiti, Nigeria: A community-based cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121241261002 for Prevalence, practice, determinants and adverse effects of self-medication among young people living in a suburban community of Ekiti, Nigeria: A community-based cross-sectional study by Agbesanwa Tosin Anthony, Aina Felixelix Olukayode, Solomon Olusoji Abidemi, Ibrahim Azeez Oyemomi, Babatola Olarinre Adefunke, Owoyemi John Ayodeji, Awelewa Babatope Ebenezer, Inubile Adekoya Joshua and Fadare Joseph Olusesan in SAGE Open Medicine
Footnotes
Acknowledgements
The authors acknowledge the support of all our research assistance in the persons of Miss Jumoke Agunbiade, Miss Olamide Agbesanwa, Miss Ayomide Agbesanwa, and Miss Ope Badmus. Appreciation also goes to the assistance of Dr Mrs Adegbilero-iwari in the statistical analysis.
Authors contribution
The study was conceived and designed by AAT and AFO. SOA, IAO, BAO, and OJA assisted with the data collection. IAJ, ABE, and FJO analyzed the data. ATA wrote the initial draft. AFO, SOA, IAO, BAO, OJA, ABE, IAJ, and FJO critically reviewed the manuscript. FJO and AFO did the supervision for final manuscript. All authors read and approved the final draft of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Ethics and Research Committee of the Ekiti State University Teaching Hospital, Ado Ekiti (EKSUTH/A67/2023/03/005).
Informed consent
Written informed consent was obtained from participants who were 18 years and above. Accent was obtained from those who were less than 18 years and written informed consent was obtained from legally authorized representatives of the minor subjects before they had the questionnaires administered to them. All the participants had formal education and could read and write.
Trial registration
This was not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.