
Abstract
Objective:
Approximately 178.5 million new cases of treatable sexually transmitted infections are thought to be diagnosed each year among young people worldwide who are between the ages of 15 and 24 years. The results regarding sexually transmitted infection prevention studies in Ethiopia are not consistent. Therefore, the objective of this systematic review and meta-analysis was to determine the pooled prevalence of sexually transmitted infection prevention methods among young people in Ethiopia.
Methods:
The systematic review was developed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Between 5 January and 18 May 2022, published studies were searched using online databases such as PubMed, CINAHL, African Online Journal, and Google Scholar. The quality of the study was evaluated using the Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument. A random-effects model was used for the statistical analysis using STATA version 14 software.
Results:
A total of 3331 studies were searched, and five studies with a total of 1925 participants were included in the final meta-analysis. The pooled prevalence of preventive practice toward sexually transmitted infections was 54% (95% confidence interval: 44, 64). According to a subgroup analysis based on regional state, the prevalence was highest in the southern region, at 66% (95% CI: 59, 73), and lowest in the Amhara region, at 42% (95% confidence interval: 38, 45). Institution-based studies had high heterogeneity, according to a subgroup analysis based on study setting (I2 = 95.39%, p value 0.001).
Conclusion:
Almost one in every two young people is engaged in preventive practices. This is lower than the World Health Organization global health sector strategy target (70%) for sexually transmitted infections. A subgroup analysis based on regional state and study setting showed a variation in the prevalence of preventive practices and significant heterogeneity among the regions.
Keywords
Introduction
Sexual contact is the primary method of transmission for sexually transmitted infections (STIs), such as chancroids, lymphogranuloma venereum, gonorrhoea, syphilis, and a variety of viruses, germs, and parasites. Additionally, it may be passed on nonsexually from mother to fetus during pregnancy, childbirth, nursing, and the use of blood products. Neonatal conjunctivitis, genital ulcers, vaginal discharge, urethral discharge, inguinal bubo, lower stomach pain, and scrotal enlargement are among the frequent symptoms of STIs.1–4
Approximately 357 million new cases of STIs are thought to occur annually among people aged 15 to 49 years throughout the world, with nearly half of those instances occurring in people between the ages of 15 and 24 years.5,6 Approximately 1 million STIs are contracted each day. 1 The incidence of STIs is higher in developing countries than in developed countries. 6 Prevention strategies recommended by the WHO in many countries include the integration of STIs with routine healthcare services; logistics supply; screening; training and supervision of healthcare providers; and strengthening surveillance systems. 6 Because of limited resources and a lack of adequate laboratory services, syndromic management of STIs based on the patient’s presenting symptoms has been the mainstay of STI care in many developing countries, including Ethiopia. However, in developed countries, case-specific management has been implemented due to the availability of resources to detect asymptomatic STIs, antibiotic susceptibility testing, and improved surveillance.6,7 STIs are a public health concern for adolescents and young people in both high- and low-income countries.4,8–12 In Ethiopia, 3% and 1% of female and male teenagers aged 15–24 years, respectively, reported having a STI. 13 Moreover, the prevalence of STI ranges from 41.7% 14 to 66.1% 15 among primary studies performed in Ethiopia. An increased chance of HIV infection, low birth weight, pneumonia, neonatal mortality, sepsis, stillbirth, newborn conjunctivitis, or neonatal blindness are major health issues caused by STIs. 1
Young adulthood is also a crucial developmental stage as youth start to understand and justify their behaviors and sexual beliefs. Young individuals are more vulnerable to unsafe abortions, risky sexual conduct, unintended pregnancies, poor academic performance, economic downturns, and psychosocial issues.1,16 Furthermore, young people’s quick growth and development may result in hazardous sex, resistance to the use of contraceptives, and early sexual beginning.17–20
Young people’s sexual behavior is also influenced by predictors such as having multiple partners, using alcohol and illegal drugs, having sex without using condoms, peer pressure, watching porn, being single, cultural, religious, not disclosing one’s HIV status, engaging in risky sexual behavior, having sex with older partners, and family disputes.4,9,11,21–27
In Ethiopia, although sustainable development goals continue to include STIs on their agenda 28 and the development of national STI management, which includes prevention strategies such as STI syndromic management, improving health worker attitudes, integrating STI into routine healthcare services, logistics supply and chain management, screening and programmatic implementation, training and supervision of healthcare providers, and strengthening the surveillance system, 29 there are not enough studies or surveillance reports on STIs in young individuals. 30 Additionally, despite studies on STI prevention techniques for young people conducted across the nation,14,15,31–33 the prevalence data are not consistent. Moreover, as far as we know, there is no systematic review and meta-analysis study on the pooled prevalence of preventive practices for STIs among young people in Ethiopia. As a result, the objective of this systematic review and meta-analysis was to determine the pooled prevalence of STI prevention behaviors among young Ethiopians.
Methods
Protocol and registration
The protocol for this systematic review and meta-analysis of preventative measures for STIs among young people in Ethiopia was published in a peer-reviewed journal and registered on PROSPERO. 34
Search strategies
The systematic review was developed using “The Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guideline.” 35 The systematic review and meta-analysis methodologies were reported using the PRISMA-P 2009 checklist.
CoCoPop search guide
Condition: STI prevention methods
Setting: Ethiopia
Population: Young people (10–24 years old) 36
Outcome: The pooled prevalence of STI prevention strategies among young Ethiopians was the study’s main finding. For young people, STI prevention strategies were taken into consideration in the primary studies whether young people received partner notification, screening, condom use/distribution, self and partner STI testing/treatment following sexual contact, preexposure prophylaxis, the use of STI services, having sex with only one partner, being vaccinated for human papillomavirus and hepatitis B vaccines, cervical screening for human papillomavirus, and being transfused with screened blood.
Data source and search strategies
From January 5 to May 18/2022, studies were searched using databases such as PubMed/Medline, CINAHL, African Journals Online, Google, and Google Scholar. Boolean operators (OR, AND) were used to search studies from databases using a MeSH term and entry terms, and modifications were made based on the types of databases (Supplemental File 1). The studies retrieved using End Note Reference Manager (version 8.1). 37 The studies were retrieved by the two authors (EW and DK). Additionally, a cross-reference search was performed on the final studies that were included.
Eligibility criteria
Inclusion criteria
❖ The following criteria were included:
Study area
Ethiopia
Study scope
Institutional and community-based studies
Quantitative results of the qualitative study design
Study design
Cross-sectional and cohort study designs.
Language
Articles in English
Population
Young people
Publication year
No restriction on the date
Exclusion criteria
Studies were excluded if
Articles other than English
Studies that did not detail particular results for the STI prevention strategy
Qualitative results
Conferences, reviews, case studies, and expert opinions
Selection of studies
The studies were evaluated independently by the two authors (EW and DK). Abstract articles and duplicate, unrelated titles were deleted. Any discrepancies between reviewers were discussed with the third author (ME). The PRISMA chart was used to depict the selection process.
Quality assessment
The “Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument (JBI-MAStARI)” 40 was used to evaluate the studies’ quality. The study subjects and settings, distinct inclusion criteria, exposure and outcome measurements, suitable statistical analysis, and accepted measurement criteria were the main areas of focus for the quality assessment. The two authors separately evaluated the studies’ quality. Studies were taken into consideration for the final systematic review if they received a quality score of 50% or above. Reviewers’ disagreements were settled by the third author (ME).
Data extraction
Pilot data extraction using Microsoft Excel was performed before the actual data extraction started. The data extraction template contained the first author’s name, publication year, study location, design, sample size, response rate, prevalence, and study subjects. The data were independently extracted by the two authors (EW and DK). Discussions were made about any differences with the third author (ME). The corresponding author of the study in case of incomplete reports was contacted.
Statistical analysis
The statistical analysis was performed using STATA version 14. For the included articles, a narrative synthesis of the data was performed. To summarize the results of the included studies, summary tables and graphs were used. A random-effects model was carried out to measure the effect size. 38 The I 2 statistics were used to examine statistical heterogeneity. 39 According to I2 values, there is 25% low, 50% moderate, and 75% substantial heterogeneity. To pinpoint the sources of heterogeneity, subgroup analysis based on region and study setting was performed.
Results
Study selection
Using various electronic database searches, including PubMed, Google Scholar, CINHAL, and African Journals Online, a total of 3331 articles were retrieved. Thirty-seven articles were removed due to duplication. A total of 3281 articles were also removed because they were not related to the title, were not conducted in Ethiopia, and were duplicated. A total of 13 full-text papers were evaluated for eligibility based on the inclusion criteria, and 8 were disqualified due to inadequate methodology or being unrelated to the intended audience. Finally, the systematic review and meta-analysis included five studies (Figure 1).
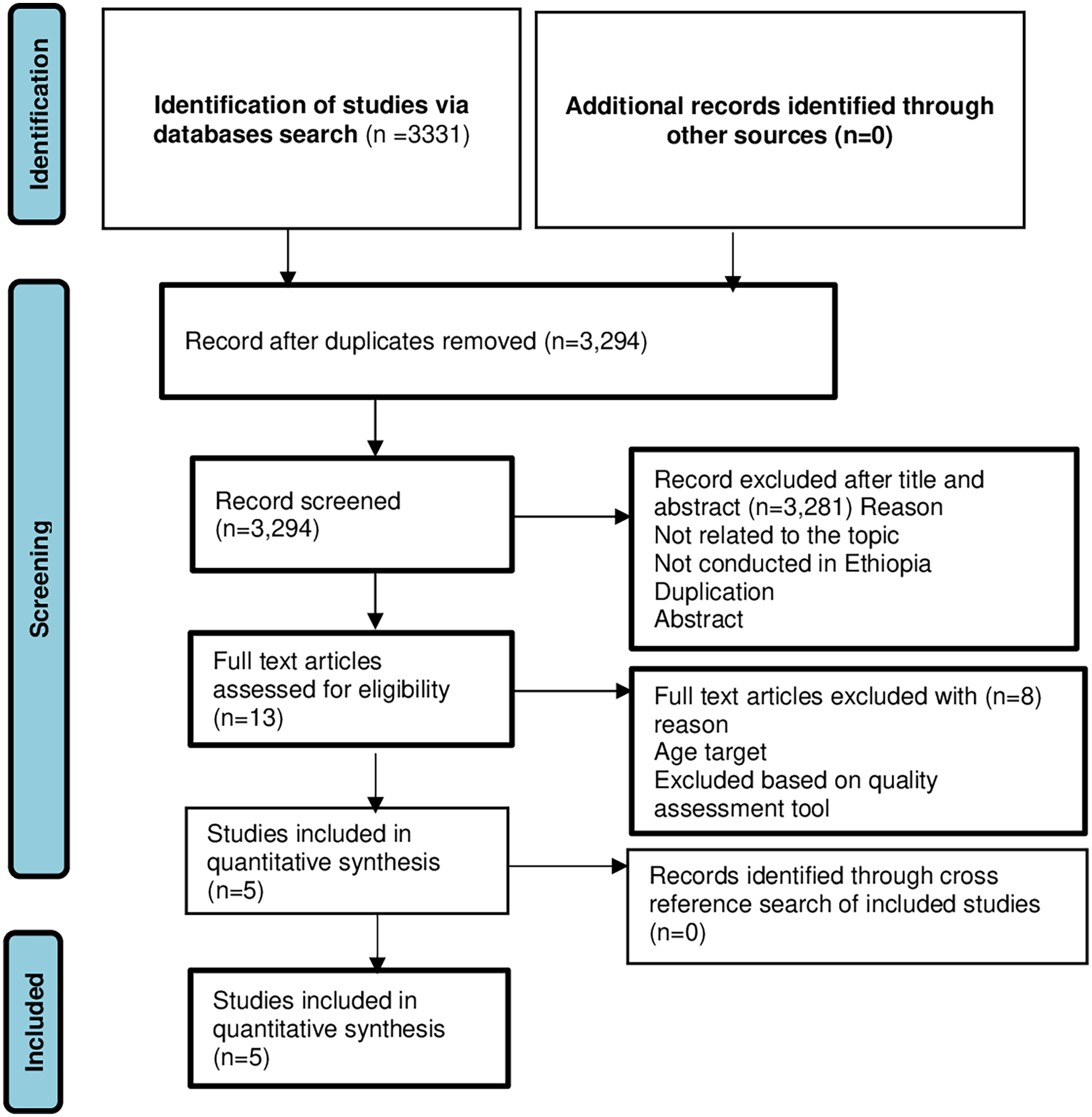
Flow chart of study selection for meta-analysis of preventive practices toward STIs among young people in Ethiopia, 2022.
Characteristics of included studies
This systematic review and meta-analysis only included cross-sectional studies. One study in Amhara, 14 one study in Oromia, 31 one study in South, 15 one study in Addis Ababa, 33 and one study national survey. 32 A total of 1925 young people were included. The sample size ranged from 64 in Oromia 31 to 815 in the Amhara region. 14 Moreover, four studies conducted an analysis to find variables linked to STI preventive methods, such as good knowledge, favorable attitude, sex, rural residence, having ever had sex, living closer to a youth-friendly service (YFS), and chat chewing. The types of preventive practices were confidence to hold a condom on hand, condom use, protected sex, single partner, not having sex after drinking alcohol, confidence to discuss condom use, and the habit of washing genitals after sexual intercourse (Table 1).
Characteristics of included studies in the meta-analysis of preventive practices toward STIs in Ethiopia, 2022.

The pooled prevalence of STI prevention methods in Ethiopia
The pooled prevalence of STI preventive practices was 54 (95% CI [44–64]). The lowest proportion of included studies was 42% (95% CI: 38, 45) in the Amhara region, 14 and the highest was 66% (95% CI: 59, 73) in the southern region. 15 The I 2 test revealed that the included studies were heterogeneous (I2 = 94.04%, p value 0.001). The Amhara region produced studies with the highest weight (21.60), 14 and Addis Ababa had 21.42, 33 while the smallest weight was in the Oromia region 16.54 31 (Figure 2).

Forest plot showing the pooled prevalence of preventive practices toward STIs in Ethiopia, 2022.
Subgroup analysis
A subgroup analysis based on study settings and regional states was conducted. According to a subgroup analysis based on regional states, the southern region had the highest prevalence of preventative behaviors for sexually transmitted illnesses, with 66% (95% CI: 59, 73), 15 while the Amhara region had the lowest rate at 42% (95% CI: 38, 45). 14 The Amhara region had the highest weight, with a weight of 21.6, 14 and the size of the sample can be the cause; the lowest weight was the Oromia region 16.54. 31 Subgroup analysis based on study setting showed that institution-based studies had significant heterogeneity (I2 = 95.39%, p value < 0.001) (Table 2).
Subgroup analysis for the prevalence of preventive practices toward STIs in Ethiopia, 2022.

Discussion
In this systematic review, we evaluated the pooled prevalence of preventative measures against STIs in Ethiopia, and it was 54% (95% CI: 44, 64). It was in line with a study performed in the USA, 63.8%. 40 However, the pooled prevalence was lower than the WHO global health sector strategy target on STIs (70%), 6 Portugal (86.7%), 41 Nigeria (74.9%). 42 The pooled prevalence was higher than that in a study performed in Nigeria (34.0%), 43 Malaysia (41%), 44 and Tanzania (42.2%). 45 The variation may result from variations in the study period, sample size, study location, sociocultural variance, and accessibility to high-quality healthcare services. The low prevalence of preventive practices for STIs among young people might have an effect on cervical cancer, infertility, HIV risk, and physical, psychological, and social problems that severely compromise the quality of life of young people. 6 The combination of behavioral, biomedical, and structural approaches, such as primary prevention methods, HIV combination prevention efforts, access to vital information, commodities, and services (such as vaccination, testing, treatment, and care), the promotion of consistent use of male and female condoms, awareness of STIs, a reduction in the number of sexual partners, and increased uptake of testing for STIs, are important prevention strategies. 6
Good knowledge, a positive attitude, being male, and living closer to a YFS were linked to an increased likelihood of STI prevention14,15,32; however, being female, residing in rural areas, ever having sex, and chat chewing were associated with lower odds of STI prevention practice.14,15,33 The types of preventive practices in the included studies were condom use, protected sex, single partner, not having sex after drinking alcohol, confidence to discuss condom use, and the habit of washing genitals after sexual intercourse.14,15,31–33
Subgroup analysis based on regional state and study setting showed a variation in the prevalence of preventive practices and significant heterogeneity among the regions. This might be due to differences in the study period, sample size, study setting, and level of awareness.
This study has the following limitations, including heterogeneity and articles published only in English. It is difficult to conclude the temporal relationship, as the studies were cross-sectional. This study was reported from four regions and one national survey, which might lack representativeness. Despite this limitation, an extensive search was conducted to minimize all possible risks of bias.
Conclusion
Almost one in every two young people is engaged in preventive practices. This is lower than the WHO global health sector strategy target (70%) for STIs. A subgroup analysis based on regional state and study setting showed a variation in the prevalence of preventive practices and significant heterogeneity among the regions. Thus, behavioral change strategies for preventive practices toward STIs are important interventions.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221145640 – Supplemental material for A systematic review and meta-analysis of sexually transmitted infection prevention practices among Ethiopian young people
Supplemental material, sj-docx-1-smo-10.1177_20503121221145640 for A systematic review and meta-analysis of sexually transmitted infection prevention practices among Ethiopian young people by Etsay Woldu Anbesu, Setognal Birara Aychiluhm, Mussie Alemayehu, Dejen Kahsay Asgedom and Mearg Eyasu Kifle in SAGE Open Medicine
Footnotes
Acknowledgements
We acknowledge Samara University for providing free access to the HINARY database websites and the internet.
Author contributions
All authors have made substantial contributions to the development of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.