
Abstract
Background:
In developing countries as well as Ethiopia, stunting continues to be a major public health burden. Thus, the aim of this systematic review and meta-analysis is to synthesize the updated pooled prevalence and its determinants of stunting in Ethiopia.
Methods:
This systematic review and meta-analysis follow the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. The protocol has been registered with the International Prospective Register of Systematic Reviews, University of York Center for Reviews, and disseminated at https://www.crd.york.ac.uk/, with the registration number (CRD42024542984). A wide-ranging literature search was carried out using PubMed/Medline, Science Direct, Hinari, AJOL, and Google Scholar. All lists of qualified study references from 2013 to 2023 were recovered. The pooled estimate with a 95% CI was calculated using a random-effects model in STATA version 13 software. I2 and meta-bias statistics were used to assess the heterogeneity of the incorporated studies.
Results:
This study included 29 articles with a total of 23,511 participants from 29 qualified studies. The current study found that the pooled prevalence of stunting among children aged 6–59 months was 43% (95% CI: 42–44). Children who were not exclusively breastfed (OR = 2.39; 95% CI: 1.61–3.54), male children (OR = 1.61; 95% CI: 1.13–2.31), children whose mothers had no antenatal care follow-up (OR = 3.03; 95% CI: 1.36–6.76), and women who had no formal education (OR = 4.55; 95% CI: 2.29–9.05) were significantly associated with stunting.
Conclusions:
In Ethiopia, nearly half of the children suffer from stunting, with those who are not breastfed, the sex of the child, children whose mothers had no antenatal care follow-up, and had no formal education having higher odds of stunting. To reduce the burden, strategies must be designed to intervene and improve maternal health literacy, focusing on children’s nutrition and health-care utilization.
Introduction
In developing countries, people frequently experience nutritional problems, which are a public health issue that persists due to several important social and economic factors. These include a lack of education, inadequate access to healthcare, cultural practices, severe food shortages, illness, inappropriate child care or feeding practices, or a combination of these factors. 1 According to the World Health Organization (WHO) Child Growth Standards median, children aged 0–59 months are classified as stunted (moderate and severe) when their height-for-age falls below −2 standard deviations for moderate stunting and below −3 standard deviations for severe stunting. 2
A low wealth index, poor dietary diversity, poverty level, education status, employment, household food insecurity, and dietary regimens are among the risk factors that increase the incidence of stunting. 3 Severe, irreversible physiological, physical, and cognitive impairments due to chronic undernourishment in early life are manifestations of stunting.4,5
In Ethiopia, a study showed that children who stopped exclusive breastfeeding experienced episodes of diarrhea, increased symptoms of acute respiratory infections (ARI), and poor nutritional outcomes because earlier termination of exclusive breastfeeding is associated with a higher incidence of childhood stunting or wasting, and this may be due to the fact that infectious diseases such as diarrhea and ARI cause children to lose their appetite and grow more slowly. 6
A review conducted in low- and middle-income countries (LMICs), where stunting is more common, found that interventions aimed at reducing the incidence of stunting include micronutrient or nutrition education for pregnant women, strengthening nutrition systems targeting children, families, and communities, and supplementation of zinc or macronutrients in children. 7
Stunting is a persistent problem for young children in sub-Saharan Africa; it affects a high proportion of undernourished children who fail to reach the normal international standard of height for their age and subsequently become stunted. 7
In Eastern and Southern Africa, the number of stunted children has increased from 23.6 million to 26.8 million, and this increase is attributed to the slow rates of stunting reduction and a rapidly growing child population, bucking a global trend where the figure of stunted children has been declining over the last 25 years. 8
Worldwide, children under 5 years of age face multiple undernutrition burdens: about 144 million are stunted, and 47 million are wasted. In Africa (with 40% of children under five stunted and 27% wasted) and Asia (with 54% of children under five stunted and 69% wasted), the greatest problem lies in all forms of malnutrition among under-5 children. 9
According to the Ethiopian Demographic and Health Survey 2016 (EDHS), 38% of children were reported to be stunted, 10 while the Mini Ethiopian Demographic Health Survey in 2019 also showed that the prevalence of stunting in Ethiopia was 37%, 11 indicating no significant decrease over the preceding 4 years.
In Ethiopia, the population of mothers and children faces multi-layered challenges rooted in socioeconomic disparities, prevalent food insecurity, limited access to healthcare services, inadequate sanitation, poor nutrition, and insufficient maternal healthcare. These factors contribute to high rates of maternal and child mortalities. 12
Stunting is a sign of chronic malnutrition but also represents problems with poverty, food insecurity, poor access to hygienic conditions, and healthcare. 13 In order to address stunting, the Ethiopian government has launched a number of initiatives, such as the National Nutrition Program, which aims to improve nutrition for both mothers and children by boosting access to nutrient-dense foods, encouraging exclusive breastfeeding, and bolstering healthcare services. 14 Furthermore, community-based programs such as the Health Extension Program have played a crucial role in providing basic nutrition education and services at the grassroots level. 15
Despite these initiatives, challenges persist, and Ethiopia remains extremely exposed to poverty, household food insecurity, and child undernutrition due to social differences, a lack of funding, and physical constraints. 16 This underscores the difficulty of addressing stunting in Ethiopia.
Providing evidence that the updated pooled prevalence and its determinants of stunted children aged 6–59 months are significant to achieving the action plan and interventions needed to reach the global targets for the Sustainable Development Goals of child health. While individual, convincing published studies have been conducted in Ethiopia to generate information regarding the prevalence and determinants of stunting among children aged 6–59, regional variations in prevalence have been observed in these studies. However, discrepancies have not been adequately documented at the national level. The findings of this review will also reveal trends in stunting and assist health planners, policymakers, and the community in reducing stunting among children in Ethiopia. Therefore, the objective of this systematic review and meta-analysis is to synthesize the updated pooled prevalence and its determinants of stunting in Ethiopia.
Methods
Protocol and registration
The protocol titled Epidemiology of stunting in children aged 6–59 months: an unresolved chronic nutritional problem in Ethiopia: a systematic review and meta-analysis has been registered with the International Prospective Register of Systematic Reviews (PROSPERO), University of York Center for Reviews, and can be found at https://www.crd.york.ac.uk/, with the registration number (CRD42024542984).
Search strategy
A broad literature search was conducted using the biomedical electronic databases PubMed/Medline, HINARI, African Journal Online (AJOL), Science Direct, and Google Scholar. Additionally, the reference lists of eligible studies were examined to obtain additional literature. All published articles from 2013 to 2023 were included in the search. This study is aimed at finding updated, comprehensive pooled information about stunting and its risk factors in Ethiopia because previous studies failed to come up with results that can be used as policy and practice input. The following search terms were used either alone or in combination with the Medical Subject Headings (MeSH terms): keywords, as the search terms, we included alternative terms for stunting and combined them by using Boolean operators. Search terms. Search (“Stunting” OR “Stunt” OR “Growth and Development” OR “Growth” OR “Body Size” OR “Body Height” AND “school-age children” OR “6–59-month-old children”) AND (Prevalence OR burden OR magnitude OR incidence) AND (“determinants OR risk factors” OR “predictors OR associated factors”) AND Ethiopia.
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) checklist guideline. 17
Inclusion and exclusion criteria
Studies were selected for the meta-analysis if they were conducted in Ethiopia, written in English, and reported the prevalence of stunting and/or risk factors. After preliminary screening of all the titles obtained from our searches, all abstracts were then assessed for eligibility by two authors (SAA and MOO) independently based on the inclusion criteria; disagreements between the two investigators were resolved through discussion and consensus. Finally, studies that met the following criteria were included in the meta-analysis: all observational studies conducted on this case in Ethiopia, featuring a response rate of 80% or higher, were included in the study. Studies that lacked quantitative reporting of outcomes were excluded. This review does not include reviews, grey literature, or studies with methodologically poor design, such as case reports or interventional studies.
Data extraction/abstraction
The data extraction was conducted by two independent researchers (SAA and MOO) using a standardized format for prevalence studies. Data extraction included the title, first author, publication year, study design, sample size, study region (site within the country), sampling methods, and the definition used for stunting. The overall prevalence rate, as well as the prevalence of stunting by region subcategories, was also extracted. Additionally, we extracted the adjusted odds ratios with corresponding 95% confidence intervals to measure the strength of the effects.
Operationalization of outcome measures
The main outcome assessed was the prevalence of stunting among the individual studies. This was determined by dividing the number of children with stunting by the total number of participants in the study, then multiplying by 100 to obtain a proportion. To analyze factors associated with stunting, data were gathered using the two-by-two table method from various studies. The crude odds ratio (OR) was calculated to identify the relationship between each independent variable and the dependent variable. The investigated factors associated with stunting included in this study were exclusive breastfeeding, maternal antenatal care (ANC) attendance, maternal education level, gender of the child, and the availability of latrines.
Synthesis of results/statistical analysis
The main outcome assessed was the prevalence of stunting among the individual studies. Information about the studies, including study sample size, events, and region, was summarized using Microsoft Excel and then exported to STATA version 13 software (Stata-Corp. LP, College Station, TX, USA). This software was selected due to its comprehensive functionalities for synthesizing data from multiple studies, which is a fundamental necessity for conducting meta-analytical research. A meta-analysis of pooled proportions was carried out using a random-effects model, generating a pooled proportion with a 95% confidence interval. A forest plot was used to present the pooled prevalence with a 95% CI. The odds ratio was used to determine the association between risk factors and stunting among the subjects included in the studies. The weights of the articles were measured to identify how much each study contributes to the overall results of the meta-analysis. Heterogeneity between studies was assessed using I-squared (I2) statistics, and cutoffs of 25%, 50%, and 75% were used to designate heterogeneity as low, moderate, and high, respectively. 18 For meta-analyses with a minimum of 10 studies, publication bias was determined based on the visual appraisal of the funnel plot 19 and Egger’s test. 20
Sub-group analyses
Sub-group analyses were performed based on the region in which these studies were conducted (Afar, Amhara, Benishangul-Gumuz, Oromia, SNNP, Sidama, Somali, and Tigray) and the gender of the study subjects (Male and Female).
Quality assessment for studies
Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument (JBI-MAStARI) 21 was applied for critical appraisal of incorporated studies prior to data extraction. Random selection of the study sample, comprehensible definition of the criteria for the inclusion of the sample in the study, identification and addressing of confounding factors, use of objective criteria to appraise the outcome of interest, reliable measurement of the outcome variable, and use of appropriate statistical analysis methods were included in the appraisal tool. After quality assessment, studies that scored five and above out of nine criteria set by the JBI for prevalence studies were included in this review and meta-analysis.
Results
Search result and description of studies
The database search and desk review were conducted using PubMed/Medline, HINARI, African Journal Online (AJOL), Google Scholar, Science Direct, and other electronic databases. A preliminary search yielded 137 articles, of which six were excluded due to duplication. Subsequently, 52 articles were excluded because the studies were conducted outside Ethiopia or were not related to the topic outcome. Additionally, 30 articles were excluded because the outcome of interest was not reported. Therefore, 49 full-text articles were accessed, and seven new studies included in the review were assessed for eligibility based on predetermined criteria, resulting in further exclusions. Finally, 29 articles were included in this study, demonstrated in Figure 1.
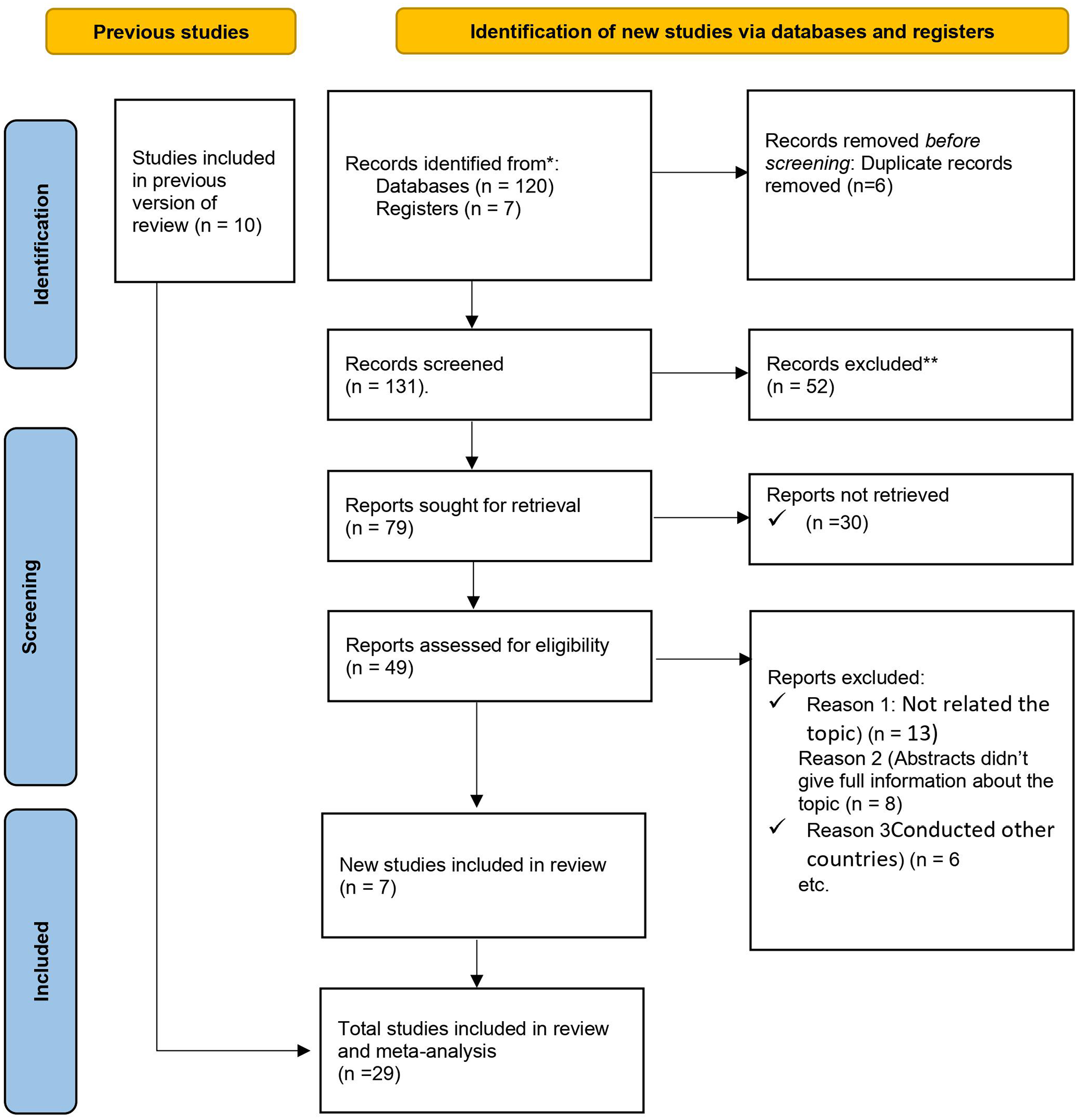
PRISMA flow diagram showing the process for selecting studies for meta-analysis, stunting associated factors and children aged 6–59 months in Ethiopia.
This review was made by applying the PICO (population, intervention, comparison, and outcomes) to the search engine:
Population: All children aged 6–59 months in Ethiopia.
Intervention: Predictors of stunting such as antenatal care, exclusive breast-feeding, sex of the child, maternal education, and latrine available.
Comparison: Reported reference group for each factor in each individual study.
Outcome: Prevalence of stunting among children aged 6–59 months in Ethiopia.
Characteristics of included studies
In this systematic review and meta-analysis, 23,511 children aged 6–59 months were included to estimate the pooled prevalence of stunting and associated risk factors among children aged 6–59 months in Ethiopia. All included studies were both cross-sectional and case-control. Among the included studies, three were conducted in the Afar region,22–24 10 studies from the Amhara region,25–34 one study from Benishangul-Gumuz, 35 and one study from the Sidama region, 36 and along with five studies, research was conducted in the Oromia region.3,37–40 Additionally, five studies were carried out in the SNNP of Ethiopia,27,41–44 with two studies each from the Somali region45,46 and the Tigray region,47,48 respectively. The largest and smallest studies were from the Amhara region 29 with 1287 participants and from the SNNP 36 with 237 participants, as depicted in Table 1.
Characteristics of the included studies.

Proportion of stunting among children aged 6–59 in Ethiopia
In the descriptive analysis, which included 27 articles, the estimated pooled prevalence of stunting among children aged 6–59 months in Ethiopia was 43% (95% CI: 42–44). The lowest proportion was 22% (95% CI: 18–27), 33 and the highest 60% (95% CI: 56–63). 44 The I2 test showed that there was no heterogeneity among the included studies (I2 = 0.00%) (Figure 2).

The pooled prevalence of stunting among children aged 6–59 months in Ethiopia sub-group analysis.
Sub-group analysis based on administrative regions of the country found stunting among children aged 6–59 months in Ethiopia to be 47% (95% CI: 46–49) in the Amhara region, 43% (95% CI: 41–44) in the Oromia region, and 43% (95% CI: 41–44) in the SNNP, followed by 41% (95% CI: 38–44) in the Afar region. Similarly, 42% (95% CI: 38–45) was reported in Tigray. The lowest sub-group prevalence of stunting was reported in Somali (33%, 95% CI: 30–35) and Benishangul-Gumus (33%, 95% CI: 29–37) (Figure 3).

Forest plot showing sub-group analysis on prevalence of stunting among children aged 6–59 months in Ethiopia.
Sub-group analysis based on sex of the child
Sub-group analysis based on the sex of the child. Table 2 provides insight into the prevalence of stunting among males and females, allowing for a comparison of the percentages of stunted individuals within each gender category. Among the females included, there were 1462 (46.59%) children who were stunted (Table 2).
Sub-group analysis based on sex of the child.

Publication bias and heterogeneity test
In this systematic review and meta-analysis, the funnel plot shows no considerable publication bias, as the visual presentation demonstrates a symmetric distribution of studies (Figure 4).

Meta-funnel showing of stunting among children aged 6–59 months in Ethiopia.
Associated factors associated with stunting
In this systematic review and meta-analysis, five factors were included from different studies. Specifically, four of them showed significance, namely lack of ANC follow-up, male sex of the child, informal education, and not exclusively breastfeeding. However, one factor, the absence of a latrine, did not show significance regarding its association with stunting among children aged 6–59 months in Ethiopia.
This study found that children who were not exclusively breastfed had 2.4 times the odds of having stunting compared to those who were exclusively breastfed, with an odds ratio of 2.39 (95% CI: 1.61–3.54) (p-value < 0.001).23,27,32,44
According to this meta-analysis study, it was found that the sex of the child influences growth problems. Male children are 1.8 times more likely to be stunted compared to their female counterparts (OR = 1.61, 95% CI: 1.13–2.31, p-value < 0.001).22,25,31,36,42,46
However, studies were assessed for the association between lack of ANC follow-up and stunting among children aged 6–59 months.24,26,31 This study found that children whose mothers had no ANC follow-up were 3.1 times more likely to be stunted compared to children whose mothers had ANC follow-up (OR = 3.03, 95% CI: 1.36–6.76, p-value < 0.001).
Five studies were assessed for the association between maternal education and stunting among children aged 6–59 months in Ethiopia.24,25,32,36,45,46 Women with no formal education were 4.6 times more likely to have stunted children compared to those with formal education (OR = 4.55, 95% CI: 2.29–9.05, p-value < 0.001). Egger’s regression test result was (p > 0.091), indicating no publication bias (Figure 5).

Analysis on factors associated with stunting among children aged 6–59 months in Ethiopia.
Strengths of the review
The use of a standardized height-for-age z-score (HAZ) measure for stunting, large sample sizes, utilization of multivariate analysis, evaluation of methodological quality, studies conducted over several years, and the publication of findings in peer-reviewed journals make the results generalizable and representative of the entire country.
The limitation of the review
This analysis did not attempt to synthesize trends in stunting over the years. Only observational studies and English-language articles were included, and the limited data by region may not provide a comprehensive representation of the area.
Discussion
Child stunting is a public health burden in developing countries, including Ethiopia. Under-five children, particularly those in Africa, are at a greater risk of stunting. Therefore, this systematic review and meta-analysis was conducted to determine the overall prevalence of stunting and identify its determinants among children aged 6–59 months in Ethiopia.
This systematic review and meta-analysis included 23,511 research participants from 29 qualified studies. In Ethiopia, the pooled prevalence of stunting among children aged 6–59 months was 43% (95% CI: 42–44). This result is consistent with the multi-level analysis study in Ethiopia, which reported that 41.20% of all children were stunted. 49
The findings of this review and meta-analysis were higher than those of the study from Pakistan DHS 50 and the multicounty meta-analysis. 51
The inconsistency in the studies’ findings could be explained by differences in sample sizes, socio-demographic factors, or geographic locations. It could also be because none of these countries has adopted the recommendation to provide comprehensive maternal and healthcare services.
According to the pooled results of this study, children who were not exclusively breastfed had a higher risk of being stunted than those who were breastfed. Similar findings from studies suggest that exclusive breastfeeding may prevent youngsters from being stunted.52–54 This may pertain to breastfeeding initiation and exclusivity for 6 months, which offer prevention against gastrointestinal illnesses that can cause severe nutritional deficiencies and stunting. 55 Breastmilk is easy to metabolize and supplies vital nutrients and vitamins required for optimal growth and development.
According to this meta-analysis, children whose mothers did not receive follow-up antenatal care are more likely to be stunted than those whose mothers did. Several studies support this claim, indicating that children whose mothers had not visited prenatal clinics had a higher risk of stunting than children whose mothers had received ANC follow-ups.56–58 These results strongly support the idea that parental guidance and dietary interventions during pregnancy have a significant impact on fetal growth and contribute to various causes of stunting. This involves the prevention and management of infections as well as underlying health problems that limit children’s growth and promote early child development. Additionally, during ANC follow-up, mothers receive counseling from medical professionals on subjects such as breastfeeding, child nutrition, and infection prevention, which may help reduce the prevalence of stunting in their children. 59
According to this meta-analysis study, it was found that the sex of the child influences growth problems. Hence, the current study, which is supported by several studies carried out in Ethiopia and outside, indicates that male children under the age of five have a higher risk of stunting than female children.31,60,61 There’s evidence to support the idea that boys are more susceptible than girls to environmental stress. Additionally, epidemiological data demonstrated that males have a higher biological susceptibility to morbidity.62,63
This study found that, compared to mothers with formal education, children whose mothers had no formal education were more likely to be stunted. Ethiopian women often lack formal education due to cultural norms, economic constraints, and residing in rural areas. This lack of education hinders access to nutrition and healthcare information, affecting child development. Children without mothers with formal education experience stunted growth, emphasizing the importance of education for making informed health decisions. 64
This finding is consistent with research conducted in Nigeria, Kenya, and Ethiopia.49,65–67 Maternal education sets the stage for better healthcare practices, acceptance of contemporary health practices, and greater female autonomy, all of which influence decisions about one’s own health and, once again, have a greater nutritional impact. 68 Ethiopian mothers initiate early breastfeeding for their children, with complementary patterns mostly aligning with WHO recommendations. This is attributed to cultural norms, robust community support, and healthcare initiatives that promote breastfeeding.69,70 These findings emphasize the importance of culturally sensitive breastfeeding interventions in supporting maternal and child health in Ethiopia.
This may be due to the possibility that mothers’ formal education provides them with the knowledge necessary to engage in nutritional and other associated behaviors that help prevent chronic malnutrition and stunting. The education of mothers has an impact on parents’ knowledge and attitudes, which, in turn, affects their use of health-care services, access to nutrition-related information, and behavior around conception.
Limitations of the study
This review considered only observational studies. Some of the studies included were cross-sectional, which meant they could not determine a temporal relationship between exposure and outcome. All the articles that were included in this review were written as English-language articles.
Conclusions
The study identified a high proportion of stunting (43%; 95% CI: 42–44) among children aged 6–59 months in Ethiopia. Among the regions of the country, Amhara, Afar, and Tigray regional states carry the highest burden. Factors such as not exclusively breastfeeding, the sex of the child, a lack of ANC follow-up, and mothers without formal education were significantly associated with the prevalence of stunting in Ethiopia.
Therefore, determined efforts are required from healthcare providers and local health planners to improve maternal healthcare services, especially in early identification of complications and appropriate management by providing nutritional health information with a focus on ANC and the postnatal period. These are crucial for promoting exclusive breastfeeding and avoiding preventable causes of child stunting.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241259862 – Supplemental material for Epidemiology of stunting in children aged 6–59 months, an unresolved chronic nutritional problem in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121241259862 for Epidemiology of stunting in children aged 6–59 months, an unresolved chronic nutritional problem in Ethiopia: A systematic review and meta-analysis by Sahardiid Ali Abdilahi, Mohamed Omar Osman and Kalkidan Hassen Abate in SAGE Open Medicine
Supplemental Material
sj-xlsx-2-smo-10.1177_20503121241259862 – Supplemental material for Epidemiology of stunting in children aged 6–59 months, an unresolved chronic nutritional problem in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-xlsx-2-smo-10.1177_20503121241259862 for Epidemiology of stunting in children aged 6–59 months, an unresolved chronic nutritional problem in Ethiopia: A systematic review and meta-analysis by Sahardiid Ali Abdilahi, Mohamed Omar Osman and Kalkidan Hassen Abate in SAGE Open Medicine
Supplemental Material
sj-xlsx-3-smo-10.1177_20503121241259862 – Supplemental material for Epidemiology of stunting in children aged 6–59 months, an unresolved chronic nutritional problem in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-xlsx-3-smo-10.1177_20503121241259862 for Epidemiology of stunting in children aged 6–59 months, an unresolved chronic nutritional problem in Ethiopia: A systematic review and meta-analysis by Sahardiid Ali Abdilahi, Mohamed Omar Osman and Kalkidan Hassen Abate in SAGE Open Medicine
Footnotes
Acknowledgements
The authors are thankful to all the individuals who contributed to the research.
Author contributions
The data analysis, drafting, and revising of the manuscript were all carried out by all of the authors. SAA and MOO planned and conducted the study, including the literature review, study selection, quality assessment, data abstraction, statistical analysis, data interpretation, and drafting of the original paper. Additionally, SAA, MOO, and KHA reviewed, edited, and compiled the paper. The final manuscript was read and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Not applicable: As evidence, systematic reviews and meta-analysis rely on publicly available records as evidence. Consequently, there is no need for ethical approval beforehand conducting a systematic review and meta-analysis.
Informed consent
Not applicable because the data included can be access and available online.
The data sharing statement
The resources reviewed in this study can be retrieved from online data sources using the provided references.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.