
Abstract
Introduction:
Healthcare facilities generate medical waste, also known as healthcare waste or health facility waste, during the healthcare delivery process, which is improperly managed as a result of underfunded healthcare systems, poor training, and lack of awareness of policies and legislation on handling medical waste as well as do not have national guidelines in place to adhere to the correct disposal of such wastage in developing countries like Ethiopia.
Objectives:
To estimate the healthcare waste generation rate among selected public hospitals in eastern Ethiopia.
Methods:
A cross-sectional study design was conducted in eight public in eastern Ethiopia from 1st June 2023 to 30th July 2023. The “Bed-Patient-healthcare wastes” model was used to estimate the healthcare waste generation rate based on WHO and empirical evidence. HCW generation rate = No of (Inpatients (Inpts) + Outpatients (Outpts))/day*0.53 kg/day. Meanwhile, general (GW), infectious (IW), pharmaceutical (PW), sharps (SW), and pathological (PtW) are computed as follows: GW = No. of (Inpt + Oupt)/day*0.53 kg/day and IW, PW, SW, and PtW = No. of Inpts/day*0.53 kg/day. In contrast, for hazardous and non-hazardous healthcare wastes, No of HCWs/day*0.8 and no. of HCWs/day*0.2 were utilized, and Key informant interviews and field observational were also applied. Descriptive analysis such as percentage, mean, and standard deviation were presented.
Result:
According to the current assessment, 105.1-142.8 kg/day healthcare waste was generated from outpatient and 167.3-244.2 kg/day from inpatients of public hospitals. From these, the Mean ± SD of daily healthcare waste generation rate estimated by non-hazardous and hazardous waste were 164.6 ± 80.9 kg/patients/day and 41.2 ± 20.2 kg/patients/day, respectively. In daily generation, the mean and standard deviations (Mean ± SD) of general wastes, infections waste, pharmaceutical wastes, sharp wastes, and pathological waste/patient were 62% (521.9), 23% (194.8), 4% (35.4), 2% (17.7), and 9% (70.9), respectively.
Conclusion:
The current assessment concluded that a large volume of healthcare waste is generated from selected public hospitals, which were not effectively segregated, separated at the source, and haven’t conventional or standard treatment. As a result, the study advised that regional and global collaboration in hospital waste and wastewater management be encouraged.
Introduction
Healthcare facilities generate byproducts known as healthcare waste (HCW), or health facility waste, clinical waste, healthcare waste, and medical trash throughout the healthcare delivery process, and HCWs were often utilized in this study. Over the past few years, there has been rising production of hazardous byproducts, including dioxins, furans, and mercury, from indiscriminate handling and treatment of HCW. 1 This situation is worse in developing countries, where there is a serious lack of reliable data on factors such as generation waste. 2 In this study, we used the term HCWs to represent the total waste generated from the Healthcare facilities (HCFs). HCWs are categorized as general and hazardous waste types. 3 Currently, HCW management is a public health and environmental concern worldwide, particularly in developing countries. 4 It is known that poor management of HCWs is a potential health risk to patients, workers, general public, as well as to the environment. 5 A systematic review of 150 articles published since 2000 revealed that at least 50% of the world population is threatened by environmental, occupational, and public health risks due to poor HCW management. 6
Of type of HCWs, hazardous waste mismanagement affects all individuals, particularly healthcare providers. The general and hazardous waste types should be properly segregated at their source of generation; 3 however, the absence of waste segregation practices at source was observed in low-income countries. 7 Probably, this could be due to lack of appropriate waste segregation utilities, lack of awareness or lack of enforcing laws and/or regulations. It is also a continentwide problem by which a systematic review in the African region indicated that 47% of the studies reported that there was absence of waste segregation. 8 The proportion of hazardous HCWs varied in Ethiopia ranged from 21% to 70%,2,9 and this proportion is higher than the hazardous waste threshold (10%–25%) predicted by the WHO. 10 In one study, even the amount of hazardous waste was higher than the general waste. 2 This could be due to the fact that during the segregation process, even a very small amount of hazardous waste is added to the general waste category, and then the entire mass of the general waste can be unnecessarily polluted by the hazardous waste. 7 Healthcare institutions, including hospitals, employ 12% of the world’s workforce and operate in an atmosphere regarded as one of the most dangerous occupational environments, with hospital-acquired infections/HAIs being the most frequent.11,12
Globally, every year, 1 in 10 of the world’s population visits healthcare institutions and is infected with HAIs due to improper HCWs management. 13 As several research and theories have been applied to describe the course of execution, certain variables worsening these difficulties are attributable to poor infection prevention and control practice compliance.14–16 The theoretical framework of medical waste management system that meets international standards is shown in Figure 1.

Adapted theoretical framework of medical waste generation and management system.
Despite the fact that the previous assessment conducted in Africa demonstrated that inadequate funding for healthcare systems, inadequate training, and a lack of knowledge about laws and policies pertaining to the handling of medical waste have resulted in a rise in improper waste management within hospitals and healthcare facilities, as well as in the transportation and storage of medical waste as well as lack national guidelines governing the proper disposal of HCWs in developing countries like Ethiopia. 17 Even such, no research has been done on the measurement of these wastes in healthcare settings, especially in public hospitals in that region of Ethiopia. Thus, the objective was to assess the medical waste generation rate and management practices among government hospitals in eastern Ethiopia. This is because significance or necessity of improving medical waste management in public hospitals, including both liquid and solid waste management. As a result, this evidence could be used to shift to a hospital circular economy, in which the multidimensional value of resources encompassing the political, social, environmental, and economic towards decision-making on medical or HCW management across developing countries, particularly Ethiopia, including study areas, which could also be illustrated as below. The first is that throughout the evaluated public hospitals, a specific regulatory structure for controlling healthcare waste and wastewater management is necessary. Second, healthcare institutions must improve their ability to plan and allocate resources for waste and wastewater management, including infrastructure maintenance and upgrades. Third, regional and worldwide collaboration in hospital waste and wastewater management should be fostered in order to reduce impact of HCWs.
Materials and methods
The study was conducted in Eastern Ethiopia on eight selected public hospitals from 1st June 2023 to 30th July 2023. Fortunately, public hospitals aimed at Eastern Ethiopia are found in three regional states and one administrative city. It was limited to Harar city, Dire Dawa city, Jigjiga city, Chiro town, and Bisidimo town. According to Central Statistical Agency Census (2007), Harari city (Total: 99,368, Male: 49,727, and Female: 49,641), Jigjiga city (Total: 125,876, M: 67,128, and F:58,748), Chiro (Total: 33,670, M: 18,118, and F: 15,552), Dire Dawa city (Total: 341, 834, M: 171,461, and F: 170, 461). 18 Meanwhile, the population of Bisidimo was (Total: 23,633, M: 12,121, and F: 11,512). 19 Recently, according to current projection population growth rate (2023), these reach a total population of 934,157.95 with 476601.12 males and 457688.49 females. In terms of study areas, cities, and towns with corresponding hospitals within a 200 km radius of Harar were chosen based on resource availability and proximity to the investigators (Figure 2).

Selection of hospitals within radius of 200 km from Harar (Harar city as the reference).
As shown in the above figure, a 200 km radius of the study, Harari Regional State, Hiwot Fana Comprehensive Specialized Hospital, and Jugola General Hospital were found. Dilchora Referral Hospital (DRH) and Sabian General Hospital (SGH) were chosen from Dire Dawa City. Jigjiga University Sheik Hassan Yabare Referral Hospital (JU-RH) and Karamara General Hospital (KGH) were chosen from the Somali regional state, which is located 103 km from Harar city. Within a 200-km radius, Bisidimo General Hospital (BGH) and Chiro General Hospital (CGH) were selected among Oromia regional state’s hospitals (namely Gara Muleta GH, Haramaya GH, and Deder GH). Finally, eight public hospitals were selected (Figure 3). From these selected public hospitals daily total ranges of 2376.0–3416 patients flow rate, BGH (150–270), 20 CGH (190–337), 21 DRH (500–693), 22 HU-FCSH (470–538), 23 JGH (190–320), 24 JU-RH (590–838), 25 SGH (190–330), 26 and KGH (246–360), 27 were shared. The mean ranges and standard deviation (Mean ± SD) by bed occupancy in eight public hospitals was (269.5 ± 132.6). Meanwhile, the (Mean ± SD) of the outpatient flow rate inpatient as well as both outpatient and inpatient in these hospitals were ((117.5–191.3) ± (57.3–77.4)), ((198.3–269.5) ± (118.2–132.6)) and (388.3 ± 190.8), respectively. From total staff of 5680 working in selected public hospitals, 1311 from DRH, 28 342 from BGH, 29 376 from CGH, 30 1256 from HU-FCSH, 31 200 from SGH, 32 351 from JGH, 33 1413 from JU-RH, 34 431 from KGH, 35 and respectively.
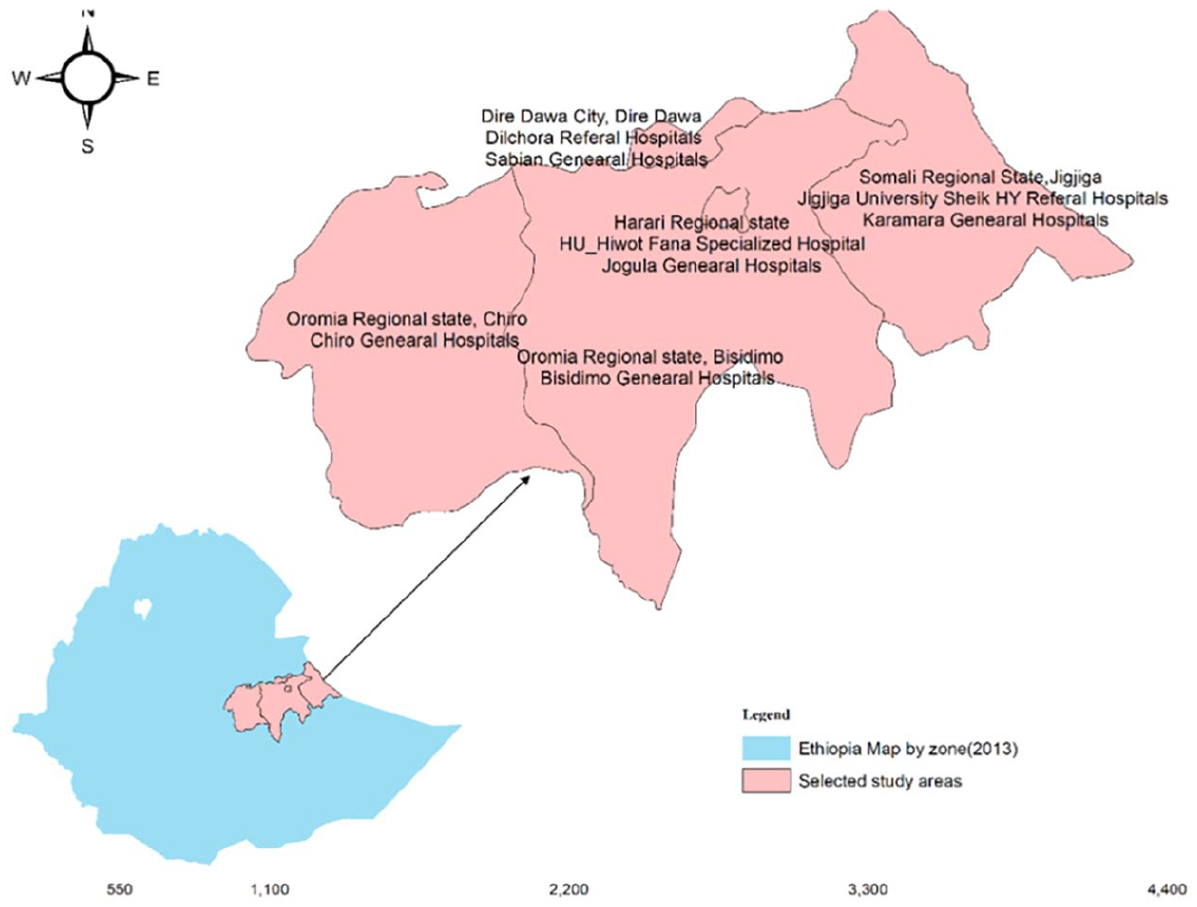
Study map of selected government hospitals to assess Health waste generation rate, 2023.
Study design
A facility-based cross-sectional research design was conducted by mixing both quantitively and qualitatively in selected governmental hospitals in eastern Ethiopia from 1st June to 30th July 2023
Inclusion and exclusion criteria
The public or government hospitals, both general, referral as well as teaching hospitals found within a radius of 200 km, were included. While private hospitals as well as HCW healthcare post, were excluded due to low production of HCWs as compared to general, referral as well as teaching hospitals. Field observation did not include stressors that may be observed within the hospitals. Thus, there may be occupational hazards in hospitals, but this remark was left out.
Data collection methods
Quantitative data collection
In eight hospitals, eight infection prevention and control/IPC experts were recruited for data collections. They were selected because these experts are working on running IPC activities, including sanitation and hygiene in the hospitals. Methodologically, to estimate healthcare waste generation rated “Bed-Patient Model,” which was developed based on the previous studies conducted in Africa, Sub-Africa, and National levels. To do this, in all selected public hospitals, number of beds and number of patients were collected by IPC experts. As the result, the total waste generation rate in the sub-Saharan region was in the range of 0.25–0.80 kg/day (0.53 kg/day), which was set for low-income countries. 36 Thus, it can derive as:

The main common HCW generated from hospital settings and levels are general wastes (GWs), infectious waste (IWs), pharmaceutical waste (PWs), sharps wastes (SWs), and pathological wastes (PtWs). 2 Accordingly, the mean coefficient (Cf) of GWs, IWs, PWs, SWs, and PtWs could generate 0.30–0.39 (0.34), 0.10–0.13 (0.11), 0.02–0.03 (0.02), 0.01–0.01 (0.01), 0.03–0.05 (0.04) respectively from a single patient (Cf = 0.53 patient/day).
Thus, it can be calculated as:


Except GWs, which were estimated from both inpatient and outpatient, four common HCWs were estimated from inpatients, which is adapted from Hayleeyesus and Cherinete. 2 Then, these coefficients were used to compute number of beds and patients. Also, the ratio of non-hazardous waste (80%) to hazardous (20%) was adopted from the WHO set for low-income countries, 36 which is computed as:
Qualitative information
Eight sanitation workers’ representatives were used as key informant interviews, which were conducted in eight hospitals. They were selected on the basis of their extensive work experience in hospitals with regard to sanitation and hygiene, as well as their exposure to cleaners, trash collectors, and garbage emptiers. Data collectors also conducted field observation for medical waste handling within the selected hospitals. About seventeen closed-ended and open-ended questions were prepared. The field observation checklist was focused on medical waste handling systems, including safe sharp according. 37
Data quality
The HCW measurement was adapted from the validated studies.2,36 For Key informant Interviews, the development of the questionnaires was guided by reviewed literature. 37 To ensure the quality of the data, standard and structured questionnaires were prepared. Then, it translated into three local languages according to favor of the speakers and regions. The second, eight data collectors were recruited from the relevant professions. Third, appropriate training was provided for data collectors (how to handle data collection process and participants).
Data analysis
Data was entered into simple Microsoft Excel Office 2019 (Microsoft Corporation, USA). Descriptive statistics was used to present mean, median, and standard deviations (continuous variables) as well as it was used for frequencies, proportions and percentages (categorical) variables. Data was presented by mean and standard deviation (SD) (mean ± SD) and percentage (%) HCWs generation, proportion, rate, and type.
Ethics approval
Ethical approval for this study was obtained from Haramaya University College of Health and Medical Sciences (CHMS), Institutional Health Research Ethics Review Committee (IHRERC) (Ref: IHRERC/064/2023). After the hospital identified whether they were willing to participate in the study and wrote a letter saying they were, the Infection Prevention and Control professionals reached an oral/verbal agreement and collected data.
Result
Bed occupancy and number of patients
The (Mean ± SD) of bed occupancy per day in the selected public hospitals in eastern Ethiopia was (269.5 ± 132.6). In the same manner, the ranges of ((mean) and (SD)) for outpatient flow rate and inpatient occupancy and overall patients were ((117.5–191.3) ± (57.3–77.4)), ((198.3–269.5) ± (118.2–132.6)) and ((388.3) ± (190.8)), respectively (Table 1).
Distribution of beds and patient flow rate in selected public hospitals, Eastern Ethiopia, 2023.

SD: standard deviation; HUFCSH: Haramaya University Hiwot Fana comprehensive specialized hospital; JGH: Jogula General Hospital; DRH: Dilchora Referral Hospital; SGH: Sabian General Hospital; JU-RH: Jigjiga University Sheik Hassan Referral Hospital; KGH: Karamara General Hospital; CGH: Chiro General Hospital; BGH: Bisidimo General Hospital.
Healthcare waste generation by outpatients and inpatients characteristics
From mean range of 315.8–460.8 (Mean ± SD: 388.3 ± 190.8) patients/day, 105.1–142.8 kg/day, and 167.3 244.2 kg/day of HCWs were estimated from outpatients and inpatients of selected public hospitals, respectively. From the mean and standard (Mean ± SD), 388.3 ± 190.8 kg/day of HCWs, 907.3 ± 529.1 kg/day, and 258.3 ± 33.1 kg/day were estimated from three referral and university hospital patients and five general hospital patients, respectively (Table 2).
Distribution of HCWs by outpatients (OPts) and inpatients (IPts) (kg/day) from selected public hospitals, Eastern Ethiopia, 2023.

Healthcare waste generation rate by type
The daily generation of general wastes, infections wastes, pharmaceutical wastes, sharp wastes, and pathological waste by (Mean ± SD)/kg/patient from the public hospitals were (70.0 ± 34.4), (25.7 ± 13.8), (4.7 ± 2.5, 2.3 ± 1.3) and (9.4 ± 5.0), respectively (Table 3).
Distribution of types of HCWs generation rate from selected public hospitals, Eastern Ethiopia, 2023.

Healthcare waste generation rate by weight
The proportionally the generation rate of general, infectious, pharmaceutical, sharps, and pathological waste was 521.9 (62%), 194.8 (23%), 35.4 (4%), 17.7 (2%), and 70.9 (9%) by weight, respectively (Figure 4).
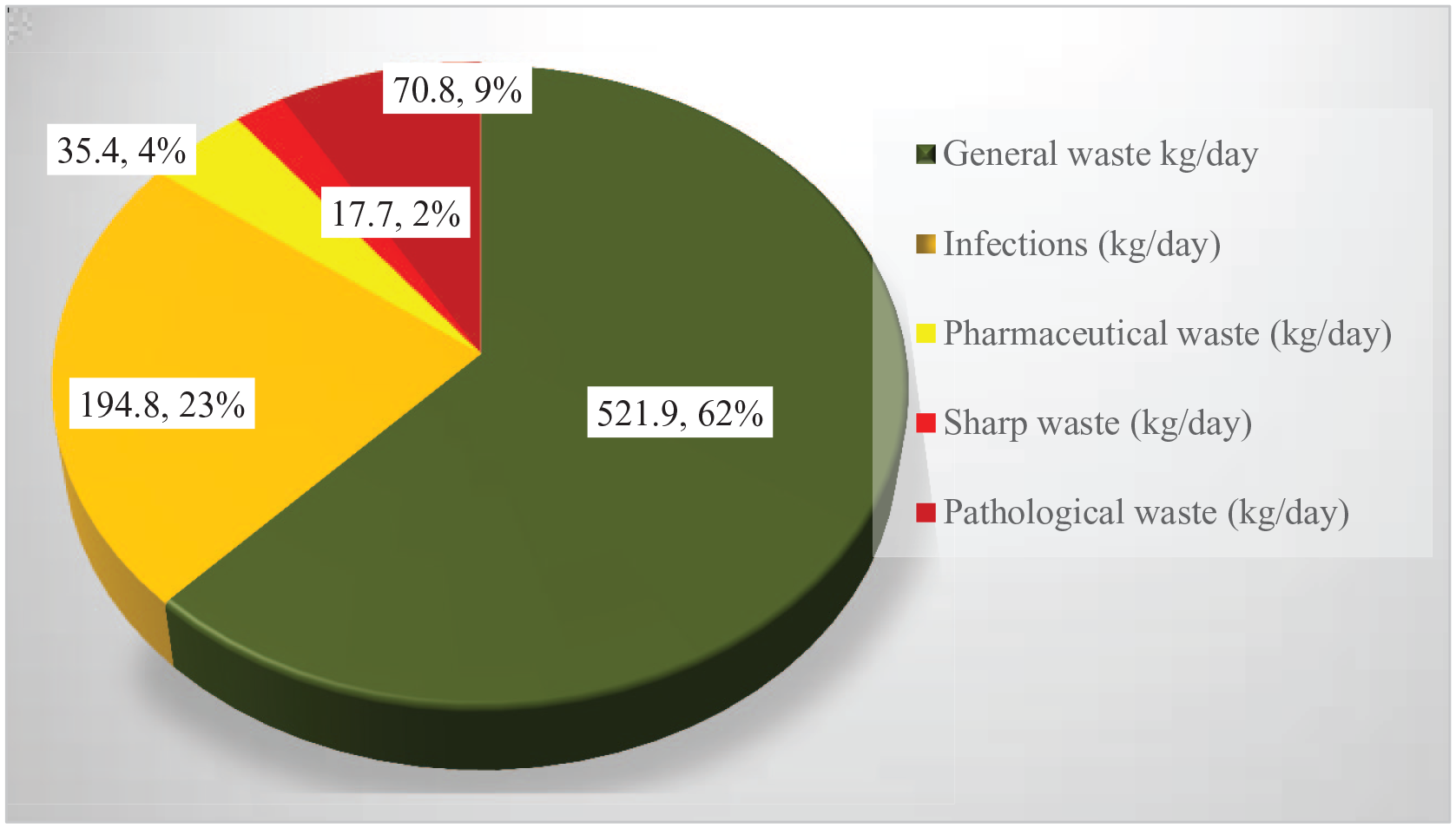
Healthcare generation rate by weight proportion from selected public hospitals, 2023.
HCWs generation by non-hazardous and hazardous
The mean and Standard deviation (Mean ± SD) of daily HCWs generation rate estimated by non-hazardous (NHW) and hazardous (HW) from waste estimated from selected public hospitals were 164.6 ± 80.9 kg/day and 41.2 ± 20.2 kg/day, respectively (Table 4).
Distribution of HCWs by generation rate by non-hazardous (NHW) and hazardous (HW) from public hospitals, Eastern Ethiopia, 2023.

Key informants’ interview sociodemographic
Out of eight sanitary workers’ representatives, all of them responded. All were females, cleaners, job categories, and permanents. Majority of them were earnt grades 9–12th. The mean ± SD for age, work experience, educational status, and monthly income salary were 34.35 ± 7.60, 6.65 ± 6.36, 6.78 ± 2.51, and $36.32 ±6.68 (1982 ± 365 ETB), respectively (Table 5).
Sociodemographic characteristics key informant interview (KII) for qualitative and quantitative information among selected public hospitals, Eastern Ethiopia, 2023.
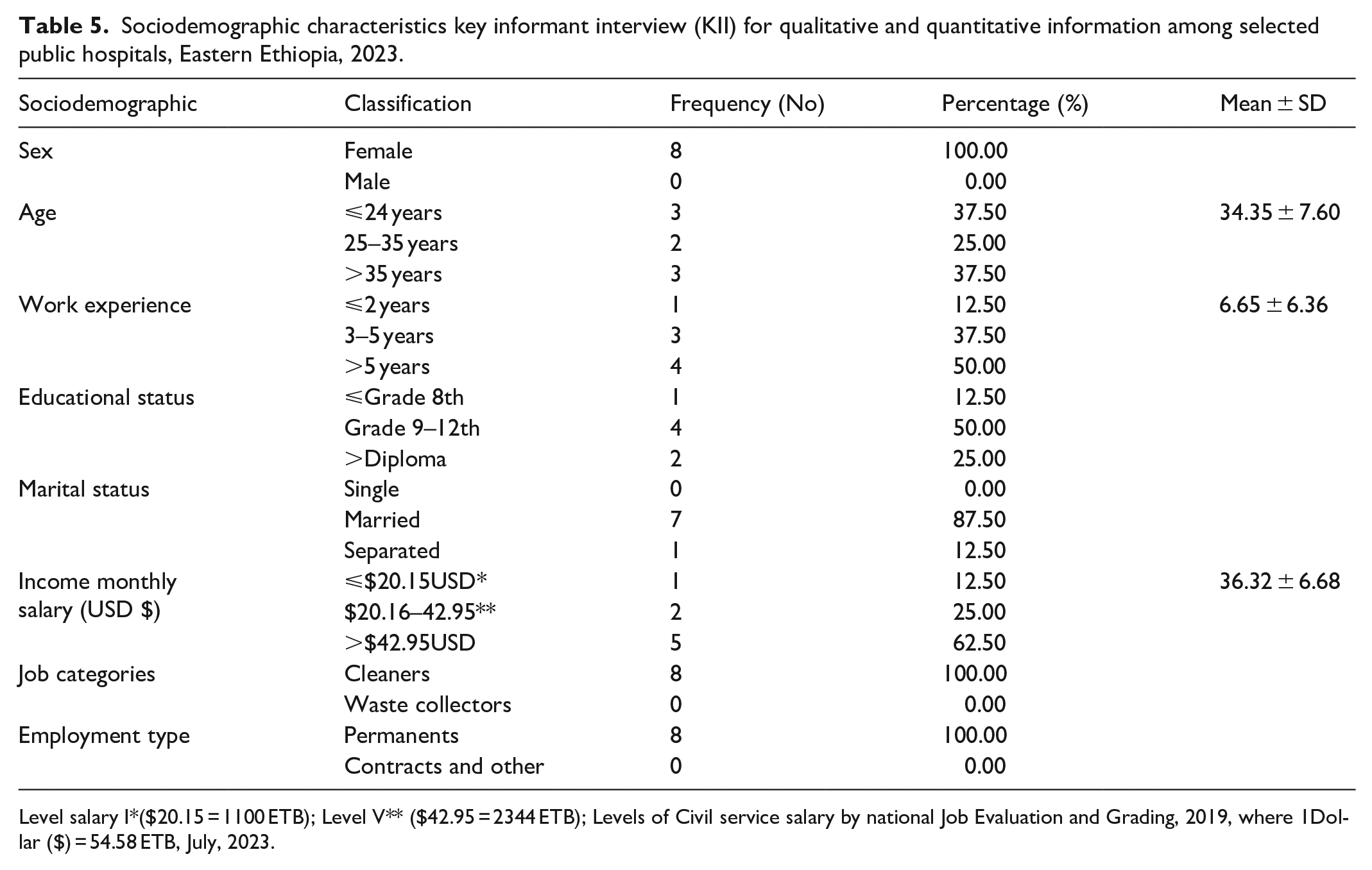
Level salary I*($20.15 = 1100 ETB); Level V** ($42.95 = 2344 ETB); Levels of Civil service salary by national Job Evaluation and Grading, 2019, where 1Dollar ($) = 54.58 ETB, July, 2023.
Key informant interview finding
The overall key informant interview (KII) response from 16 items provided for sanitary workers’ representatives was 44.92%. From this figure, report for the occurrence of injuries due to improper medical waste (MW) handing, providing post-exposure prophylaxis/PEP/those impaired by piercing of sharp materials from the medical waste, hand hygiene practice after their work or duties, government or voluntarily partner monitoring about medical waste management and take necessary measures, and overall medical waste management accounted less than half percent (Table 5).
Field observation
Field observational found that almost eight public hospitals did not segregate trash at the source and did not use a standard incinerator to dispose of medical waste. The observation also found that the hospital's sewage system is not well-designed for the people who use it, and the sewage pipes are not easily identified for maintenance and maybe replacement. Because of urbanization, these areas have a high population density, resulting in a high patient flow rate in each hospital. The patient load and medical waste, on the other hand, are unparalleled. One of the major problems at these hospitals was the lack of operable trash collection containers nearby for non-infected (general) garbage, infectious waste, and sharps waste.
Discussion
The present assessment indicated that the daily mean (bed occupancy), (outpatient flow rate) and (inpatient) were (269.5 bed/day), (117.5–191.3), (315.8–460.8), (388.3), respectively in selected public hospitals (Table 1). In a daily basis, (105.1–142.8 kg) and (167.3–244.2 kg) of HCWs were estimated from outpatients and inpatients, respectively. Combining the in/outpatient HCWs generation rate, the mean and standard (Mean ± SD) of medical waste estimated from the hospitals was 388.3 ± 190.8 kg/patients/day (Table 1). This finding is higher than 228.6 kg/patient/day obtained from Hospitals found in the South-Eastern of Ethiopia. 2 Also, it is higher than 278.85 ± 86.15 kg/patient day reported from Central Ethiopia. 38
According to the field observations, nearly eight of them did not separate the waste at the source and did not employ a typical incinerator for HCW handling. Furthermore, the hospital’s sewage system is not effectively constructed for individuals who use it, and the sewage pipes are not easily recognized for maintenance and perhaps replacement. As is well known, these places have a high population density owing to urbanization, which results in a high patient flow rate in each hospital. However, the patient load and HCWs are unrivaled. One of the significant concerns at these hospitals was the lack of functional trash collection bins in close proximity for non-infected (general) rubbish, infectious waste, and sharps waste. There is no functional burial pit/fenced garbage dump or municipal pick-up for noninfectious (non-hazardous/general waste) disposal. There is no incinerator or alternative treatment technology for infectious and sharp waste (e.g., an autoclave) present (either on or off-site and operated by a licensed waste management service), functional and of sufficient capacity, and no standard wastewater treatment system present (either on or off-site) and operating reliably.
As a result, these issues must be resolved in the future under the banner of HCWS’s sustainable management through collaboration or any initiative involving these hospitals. From the recurrent overall estimation, 907.3 ± 529.1 kg/patients/day and 258.3 ± 33.1 kg/patients/day HCWs were estimated from three referral and university referral and teaching hospitals and five general hospitals (GH), respectively (Table 2). This indicates that even if there were five general hospitals, the load of HCW generated by university referral and teaching hospitals (i.e., 3) was more than three times that of general hospitals (i.e., 5), and this issue will be considered again during the development of HCWs management projects.
The most common types of HCWs were general wastes, infections wastes, pharmaceutical wastes, sharp wastes, and pathological wastes in which the mean and standard deviation (Mean ± SD) were 70.0 ± 34.4 kg/patients/day, 25.7 ± 13.8 kg/patients/day, 4.7 ± 2.5, 2.3 ± 1.3 kg/patients/day and 9.4 ± 5.0 kg/patients/day, respectively (Table 3). However, the study conducted in northern Ethiopia in public hospital found that the mean ± SD for 7 days were general, infectious, sharp, pathological, and pharmaceutical wastes were 184 ± 27.9, 128 ± 27.3, 3 ± 1.7, 18 ± 5.4, and 6 ± 5.2 respectively. 39
Proportionally, general wastes, infectious waste, pharmaceutical, sharps waste, and pathological waste accounted for 62%, 23%, 4%, 2%, and 9% by weight, respectively (Figure 4). This result deviated from the study found in public hospitals South-Eastern Ethiopia, in the proportion of general, infectious, pharmaceutical, sharps, and pathological waste was 25.18%, 22.31%, 22.87%, 9.24%, and 20.40% by weight, respectively. 2 Moreover, the mean and standard deviation (Mean ± SD) of daily HCWs generation rate estimated by non-hazardous (NHW) and hazardous (HW) from waste estimated from selected public hospitals was 164.6 ± 80.9 kg/patients/day (79.69%) and 41.2 ± 20.2 kg/patients/day (20.31%), respectively (Table 4). However, in addition to quantification of medical waste generation, the qualitative information was assessed using key informant interviews and field observational. According to sanitary workers’ representative feedback, the overall mean percentage of the well design path for medical waste transportation until the disposal site and general medical waste management system (liquid waste management and solid waste) in selected public hospitals were 56.25% and 37.50% (Table 5).
Sanitary workers’ representatives Codes 1, 2, 3, 4, 5, 6, and 7 had nearly identical opinions: “As far as I am concerned, the hospitals have poor solid waste management are” they added, we dispose of solid waste at the proximal temporarily disposal site because to a lack of other disposal sites, which exposes the hospitals’ community as well as the surrounding community to illness.” Observation indicated that Pits are found in the some of hospitals but insufficient dimensions; pits/dumps overfilled or not fenced/locked; or irregular municipal waste pick up. In case of liquid waste management, these KII also reported as “there is no standard wastewater treatment system, for example, septic tank followed by drainage pit present either on or off site and functioning reliably.”
This practice could have adverse effects on the hospital community. Because the study found that the majority of medical waste consists of heavy metals, including mercury, which characterize both bioaccumulation and bioconcentration if contact with tissue of human beings and water bodies, respectively, through biomagnification processes. 40 As a result, waste incineration is the main waste management strategy recommended to treat hospital waste in many developing countries, 41 that is applicable to eastern Ethiopian hospitals.
Moreover, according to the field observations carried out in eight selected public hospitals, medical wastes are not properly separated based on their features and kind. Moreover, regulated medical waste is not being managed and disposed of in accordance with municipal, state, and federal standards. The observation also indicated a functional waste collection container for noninfectious (general) waste, infectious waste, and sharps waste in close proximity to all waste generation points. Also, a functional burial pit/fenced waste dump or municipal pick-up is available for disposal of noninfectious (non-hazardous/ general waste not available (Observation, 2023).
Out of eight hospitals, seven of them haven’t an incinerator or alternative treatment technology for the treatment of infectious and sharp waste (e.g., an autoclave) present (either present on or off-site and operated by a licensed waste management service), functional and of a sufficient capacity.
Moreover, field observation of 80 sanitary staff members observed randomly from eight public hospitals (10 in each) revealed that 70% did not perform hand washing following their last responsibilities. Almost seven of the eight public hospitals that were selected for field observations in terms of medical waste management did not properly separate and segregate medical wastes according to their characteristics and sort. Such practice is a problem for healthcare waste handlers because medical trash that contains sharp objects or needlestick materials can cause adverse effects related to working conditions. This finding is similar to the finding obtained from a hospital in the city of Maranhão, Brazi, where inadequate segregation of health service waste (HSW), failure to consider the health hazards of hospital waste, and failure to use personal protective equipment (PPE) reports that leads occupational impairments among frontlines. 42
Sanitary workers’ representatives Codes 2, 3, 4, and 6 reported as the problems of hospitals waste segregation in our hospitals are health care workers ignorantly, they disposed gauze, needle and other sharp materials without proper handling. This type of practice is mostly accounted since we are here in the hospitals. On the other hands, Sanitary workers’ representatives Codes 1, 2, 5, 6, and 7 had nearly identical opinions: As they informed “Our hospital leaders have thought as the responsibility of hospitals waste management only for sanitary workers, namely waste collectors and cleaners”
Moreover, regulated medical wastes are not handled and disposed of according to local, state, and federal regulations. They did not know the exact color code of garbage containers, and also there were no puncture-resistant sharp containers for disposal of sharp and needle stick materials, and even the safety boxes utilized within the hospital were insufficient to conduct safe sharp and needle injections. According to the research, most HCFs, such as hospitals, have inadequate medical waste management practices. This finding was slightly similar to the study found in Brazil hospitals, where 82.23% of them were unaware of what they are or how they are classified, 57.29% were unaware that there is specific legislation governing medical waste management, while 93.97% claimed that waste was segregated, 63.13% were unaware of the final destination and treatment of medical waste. 42
While collecting medical trash, some sanitary employees used surgical gloves. Despite this, sanitary staff did not wear this glove because it is unsuitable, as they claimed. However, for such tasks, a heavy-duty glove is advised. According to KII suggestions, hospitals should provide enough heavy-duty gloves for sanitary personnel to avoid occupationally connected hospital-acquired infections. Moreover, the significant majority of these randomly selected sanitary employees from eight public hospitals did not dilute, store, shelf-life, or contact time of disinfectants for cleaning purposes according to manufacturer standards. This may have exacerbated the repercussions of occupational-related failures that may have resulted in an accident at work.
The key informant interview (KII, 2023) revealed that the overall mean percentage of availabilities of PPE within hospitals, conformability of PPE, and utilization of PPE among sanitation workers those workers engaged with waste collection and cleaning the hospitals hadn’t washed their hands after their work in selected public hospitals was 51.00% (Table 6). This finding is lower than the study found from Brazil hospital cleaners, use of personal protective equipment (PPE), primarily consisting of boots, gloves, and masks); 85.43% claimed to use them routinely. 42 Despite of the fact that sanitary workers’ representatives Code 2, code 4, code 5, and Code 8 reported that,
Key informant interview (KII) inputs on medical waste management and health and safety of sanitation workers among selected public hospitals, Eastern Ethiopia, 2023.

“As you know, our sanitary workers and cleaners are collecting medical wastes and cleaning the hospitals that may we expect high severe to their health. However, the unavailability of PPE and un-comfortability of PPE were commonly observed in our settings.” In addition. They informed as “utilization of PPE as well as distribution time of PPE in our hospital is very worth. As the result our coworkers had exposing with numerous occupational hazards within a work place of the hospital. Disposable items such as injection safety devices, examination gloves existed but only sometimes available”
The KII (2023) report shows that the overall mean percentage of the confined room for workers to change their clothes after medical waste handling, as well as the hygiene practice after collecting waste in selected public hospitals, was 50.00% and 31.25%, respectively (Table 6).
As sanitary workers representative codes 1, 3, 5, and 7, we claimed that we considered ourselves to be slaves in the hospital since we wore our existent PPE as well as other uniform with open space without maintaining our privacy due to a lack of contained place for cloth as well as PPE. Moreover, they reported as “our workers have reliable sterile and disinfected equipment ready for use for average ⩾5 days per week or every day, but not of sufficient quantity.” This demonstrates that the hospital pays little attention to sanitary staff for those working sanitary working including medical waste management.
As indicated above, the pooled percentage of adherence to personal protective equipment practice hand hygiene was less than half percent towards standard precautions of medical waste management among waste handlers. Therefore, they have the possibility to acquire medical waste-related occupational health problems during their working time.
The KII (2023) report shows that the overall mean percentage of training on medical waste handling, management, and way of prevention of waste-based disease in selected public hospitals was 38.00% (Table 6). Of these KII, waste collectors’ representatives Code 1, code 2, code 5, and code 8 reported in the same opinion.
We did not receive any training about medical waste handling, management, or ways to prevent waste-based disease since we began working in the hospital, because the majority of management leaders and clinical leaders did not focus on waste segregation, generation, handling procedures, or management, instead focusing solely on hospital care service.
This study slightly similar to the study found from Brazil hospitals, where 82.92% of the workers’ coordinators claimed to have received some training. The study stated that 23.12% said they had been trained only when they were admitted. Risks associated with handling medical waste were mentioned by 87.94% of the HCW coordinators. 42
Strength and limitation
Strength of the study
This study’s cross-sectional study design and validated techniques made it possible to collect data simultaneously, and it made it simple to assess the evidence about the rate at which certain hospitals generated HCW. Additionally, the study was able to estimate the rate at which HCW is generated as well as the management practices of the chosen hospitals. This offers compelling evidence in support of descriptive analysis and the development of research hypotheses regarding the rate at which HCW is generated, as well as the management practices among the hospitals.
Limitations of the study
Notwithstanding its advantages, the hospital sapling procedures were based on a 200-km radius around the investigators’ homes and the availability of resources, which may have introduced selection bias. The other limitation, the total number of subjects, calculation as well as the sample size selected for this study for quantitative aspects, particularly for medical waste estimation used patient per bed waste generation approaches. This could cause the results to be either over or understated. In this study, the study’s qualitative outcome considered data saturation, even though the primary Informant interview may have more or less information than needed. Because the pilot test was not carried out outside of the research locations, the results may not be of high quality. A further discussion about improper HCW management has been hampered by the lack of evidence regarding the long-term effects of improper HCW on workers, particularly sanitary workers in hospitals who were vulnerable to exposure to highly infectious HCWs during their work activities.
Conclusion
The current assessment concluded that a huge amount of HCWs is produced that is not appropriately segregated and separated at the source, and hospitals do not use a conventional or standard incinerator for HCWs management. On the other hand, the hospital’s sewage system is not well-designed for the people who use it, and the sewage pipes are not easily identified for maintenance and maybe replacement. Moreover, in all hospitals, there was low adherence to HCW management system within the selected public hospitals. As a result, infection prevention and control practices could be poor because the waste management system is one of the components of infection prevention and control practice components practice. This illustrates a lack of HCW management procedures, and poor infection prevention and control practices could as a consequence on staff, patients, and visitors.
Therefore, the study provided the following recommendations in order to satisfy safety and hazards free of HCW. The first one, it is critical to develop a separate regulatory system in charge of regulating healthcare waste and wastewater management based on theoretical framework. Second, it should be crucial to improve healthcare institutions’ capacity to efficiently plan and allocate resources for waste and wastewater management, including infrastructure maintenance and improvements. Third, it is very significant for regional and worldwide collaboration in hospital waste and wastewater management to be promoted to encourage shared learning and improve preparedness for future pandemics and environmental degradation. Also, hospitals need to comprehend how poor HCW management affects patients, staff, visitors, students, and the surrounding community. In order to mitigate the negative effects of inappropriate disposal on public health, the Ministry of Health and Environmental Protection agency should collaborate on the sustainable management of medical waste.
Footnotes
Acknowledgements
Our gratitude will be extended to our host university, Haramaya University College of Health and Medical Sciences, which provided us with financial support for data gathering.
Authors’ contribution
STT, AA, KK, and MM developed the proposal. STT, AA, KK, and MM contributed to data collection process. STT compiled data from the hospitals. STT, AA, KK, and MM wrote the manuscript. All authors contributed to this job.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for data collection was provided by Haramaya University College of Health and Medical Sciences (Research Code: HURG_2023_02_01_64).
Ethics approval
Ethical approval for this study was obtained from Haramaya University College of Health and Medical Sciences (CHMS), Institutional Health Research Ethics Review Committee (IHRERC) (Ref: IHRERC/064/2023). After the hospital identified whether they were willing to participate in the study and wrote a letter saying they were, the infection prevention and control professionals reached an oral/verbal agreement and collected data.
Informed consent
Eight sanitary workers’ representatives participated in the study as Key informant interviews. Eight of them signed consent to participate in the study.
Trial registration
Not applicable.