
Abstract
Background:
There are few studies that have evaluated the provision of compassionate care in Ethiopian contexts. One probable factor could be a lack of validated tools for assessing compassionate care in Ethiopia.
Objective:
To adapt the Compassionate Care Assessment Tool into the Amharic version and to assess its reliability and validity for application in obstetric services of the Ethiopian context.
Method:
Four hundred ten mothers who gave birth at the four referral hospitals in North West Amhara participated in this study. Using SPSS version 23.0 and SPSS Amos 26 and by applying principal axial factoring, the Compassionate Care Assessment Tool was assessed for structural reliability and validity. Cronbach’s alpha was used to evaluate internal consistency and reliability. Factor loadings, composite reliability, average variance extracted and square root of the average variance extracted were used to test convergent and discriminant validity.
Results:
Three factors with thirteen items were identified that explained 69.87% of the variation in the Compassionate Care Assessment Tool. Cronbach’s alpha was 0.917. In the confirmatory factor analysis, all items had factor loadings more than 0.6, and the average variance extracted was greater than 0.5. Composite reliability values were above 0.7, and the square root of the average variance extracted for each element was greater than the correlation of each factor with other factors in the model.
Conclusion:
The three factors and the thirteen items of the tool have shown internal consistency in the exploratory factor analysis. The factor loadings and the average variance extracted confirmed the convergent validity of the tool, while composite reliability and the square root of the average variance extracted values confirmed discriminant validity. Thus, the Amharic version of the Compassionate Care Assessment Tool was found to have excellent internal consistency as well as adequate structural, convergent, and discriminant validity among obstetric service users in Ethiopia.
Introduction
Compassion is a combination up of five components: understanding suffering, recognizing the universality of human suffering, empathy for the person suffering, tolerating unpleasant feelings, and motivation to act/acting to alleviate suffering. 1 Providing compassionate care to patients is essential to current patient care, the practice of professional nursing, and individual center approach.2,3 Compassionate care can be considered as a key element and an indicator of patient-centeredness and successful nursing.4,5
Measurement and reporting of the experiences of patients receiving care are necessary and ongoing efforts to enhance the quality of care. 6 To assess patients’ perspective of compassionate care, various instruments have been developed. These include the 12-item Schwartz Center Compassionate Care Scale (SCCCS), used to assess patient perceptions of care provided by attending physician, 6 the Compassionate Care Assessment Tool (CCAT), used to assess compassionate nursing care in acute hospital environments, 7 Compassionate Care Questionnaire for Nurses 8 and others.
The previous Ethiopian Health Sector Transformation Plan (HSTP) I and the current HSTP II has stated compassionate health work force as one transformational agenda as medical care without compassion and respect cannot be truly patient-centered.9–11 Even though compassionate care has been given emphasis by the Ethiopian HSTP, there are few studies that assessed the provision of compassionate care in Ethiopian settings. One possible reason may be the lack of validated tools to assess compassionate care in the Ethiopian service provision context.
Due to the aforementioned differences between settings, when evaluating compassionate care using instruments created in a different context without validation, a tool may not accurately reflect the level of compassionate health care provided by a given healthcare. These justifications call for refraining from evaluating the state of compassionate care without first undertaking a cross-cultural adaptation study in Ethiopian context setting. 12
An earlier study carried out in Ethiopia revealed that the SCCCS which is reduced into a 10 items has a high internal consistency and an acceptable structural validity value. 12 However, the SCCCS is a one factor-loaded tool, which can make it difficult to make dimension-related analysis, interpretation, and recommendations. Thus, the CCAT which has four dimensions, which are the capacity to create meaningful connections, fulfill expectations, demonstrate caring qualities, and perform as a competent practitioner illustrated compassion from the patients’ point of view and can make it more feasible to conduct dimension-based analysis, interpretation, and recommendation of the findings. These dimensions are Meaningful Connection, Patient Expectations, Caring Attributes, and Capable Practitioner. 7
Therefore, the purpose of this study is to culturally adapt and evaluate the validity and reliability of the CCAT in obstetric care in Ethiopia.
Methods and materials
Study design, period, and area
An institution-based cross-sectional study was conducted from 2 March to 8 May 2020 G.C. The Strengthening the Reporting of Observational Studies in Epidemiology guideline for cross-sectional studies was followed. 13 The study was conducted in the north-west part of the Amhara region, which is one of the 12 Ethiopian regions. The area encompasses 8 out of the 13 zones of the Amhara region. At the time of data collection, the area had four referral hospitals: the University of Gondar comprehensive specialized hospital, Felege Hiwot comprehensive specialized hospital, Tibebe Ghion comprehensive specialized hospital, and Debre Markos comprehensive specialized hospital, all located in Gondar, Bahirdar, and Debre Markos, respectively. According to information from those hospitals, in combination, they serve a population of more than 15.5 million. The four referral hospitals provide a wide range of specialty services, including obstetric services and institutional delivery services, for a large number of pregnant mothers. Data obtained from the previous 6-month report before the data collection (July–December, 2019 G.C.) indicate that, in combination, the four referral hospitals have provided delivery services for more than 13,000 pregnant mothers.14–17
Study population
All mothers who gave birth in selected comprehensive specialized hospitals in North West Amhara were considered as a source population. Whereas all mothers who gave birth during the data collection time in the selected comprehensive specialized hospitals were considered as a study population.
Eligibility criteria
Mothers who gave birth within the data collection time in the selected referral hospital and who can speak Amharic language were included in the study. We excluded mothers who were critically ill or unable to communicate at the time of data collection.
Sample size and sampling procedure: Since this study was conducted as part of another research objective to assess respectful maternity care, the sample size required for the present study was derived using a single population proportions formula, as follows: n = (Z α/2) 2 P(1−P)/d2 where n is the sample size, Z is the standard normal distribution that defines the significance level at α = 0.05, and d is the estimated 5% margin of error, and P is the proportion of women reporting compassionate care while giving birth. Since, there is no research conducted in Ethiopia that assessed compassionate maternal care, by taking a proportion of 50%, the sample size was estimated to be 384. By selecting the sample size from the above results and considering a 10% non-respondent rate, which gives 38, the final sample size required was 422. To confirm the sample size is above the minimum required sample size, a Daniel Soper sample size calculator for structural equation modeling was used with assumptions of an anticipated effect size of 0.3, statistical power of 0.8, a number of latent variables of 4, and a probability level of 0.05. The minimum sample size required was 137. Since the first sample size of 422 was larger than 137, a sample size of 422 was used.
The study participants were chosen using a systematic random sampling method. Since the most recent six-month report before data collection shows that a total of 13,208 mothers gave birth in such facilities, the sampling interval (K) was computed using a monthly average of 2202 mothers. K = N/n = 2202/422 = 5.22 = 6. Women are expected to stay for 24 hours following delivery before being discharged. Immediately after delivery, the birth record will be registered in the delivery registry book. When data collection was started, we considered the first registered mother to be number one. As three was chosen at random as the starting point and six as the sampling interval, every sixth registered mother on the delivery registry was included until the proportionally allocated number for each hospital was attained.
Data collection instrument and procedure
Face-to-face interviews were conducted with the selected mothers who gave birth in the selected institutions, using a structured questionnaire on exit interviews after they had stayed in the postpartum rooms and the decision to discharge the mothers was reached. The questionnaire contains sociodemographic questions and the translated Amharic version of the twenty-item, five-point Likert scale CCAT 7 (Supplemental file 3). The five-point Likert scale has options from strongly disagree to strongly agree. The CCAT is used to evaluate compassionate nursing care in acute hospital environments. 7 The CCAT comprises four categorized components that demonstrate compassion from the patient’s perspective: the ability to make meaningful relationships, satisfy expectations, exhibit caring characteristics, and function as a competent practitioner. These segments are Meaningful Connection, Patient Expectations, Caring Attributes, and Capable Practitioner. 7
Linguistic validation
Translation and cultural adaptation of the CCAT were performed according to the minimal translation criteria of the Medical Outcomes Trust (Medical Outcomes Trust, 1997). 18 Two independent bilingual translators (one an Amharic language lecturer and the other an English-language lecturer) with advanced English and native Amharic language skills translated the CCAT into Amharic. They made no changes to the items’ meanings. An English-language lecturer who is a natural Amharic speaker but has been blinded to the original version produced a back translation. There were no serious issues with reconciling the back-translated version.
Data quality control
Data quality was maintained in four phases: tool development, data collection, data management, and analysis phases. The data collectors were trained for 1 day. Training was given about the questionnaire prior to data collection. The training focused on the contents of questionnaires and interviewing techniques. To assure data quality, a pretest was performed on 5%, or 21 of the questionnaires, at Debre Tabor General Hospital, which was not part of the study. Potential wording issues discovered during the pre-testing phase were addressed and adjusted. Supervision and checking were carried out to ensure that the obtained data were complete and consistent. All collected data were checked for completeness and consistency during data management, storage, and analysis.
Data analysis
Data were entered into Epi-data 3.1, then exported and coded into SPSS version 23 and SPSS Amos 26 and cleaned using data cleaning techniques and all errors were corrected after retrieving and cross-checking with the actual questionnaires.
Descriptive statistics were used to describe the characteristics of the study participants. Mean and standard deviation (SD) were used for the description of continuous data, while median, interquartile range, frequencies, and percentages were used to describe categorical data. The two techniques (exploratory factor analysis (EFA) and confirmatory factor analysis) of factor analysis were employed to determine the number and nature of latent variables or factors. A number of steps have been taken to conduct the two techniques of factor analysis. First, the data’s eligibility for factor analysis was confirmed by running the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy, Bartlett’s test of sphericity, and the determinant of the R matrix. The KMO determines if the variables belong together psychometrically and, as a result, whether the correlation matrix is suitable for factor analysis. 19 The recommended value of KMO should be 0.5 or above to be regarded suitable for factor analysis, where values >0.9 are considered marvelous. 0.8–0.9 meritorious, 0.7–0.89 s middling, 0.6–0.69 mediocre, 0.5–0.59 miserable, and below 0.5 unacceptable. 19 The Bartlett’s test of sphericity, which tests the hypothesis that the correlation matrix is an identity matrix and there is no relationship among the items, was also checked. 20 The Bartlett’s test of sphericity should be significant; a significant value < 0.05. 21 Secondly, factor extraction analysis was undergone using the principal axis factoring (PAF) method of factor extraction. The criterion for determining the number of common factors to be retained included the eigenvalue, scree test, and cumulative percentage of variance. Factors with eigenvalues greater than 1.0 were considered significant and were kept, while the rest were discarded.22,23 Together with the PAF, a varimax rotation method was selected in order to have a more interpretable and simplified solution. Items were removed from the EFA if they were double loaded (i.e., 0.40 or above on more than one factor), unique, and did not load into any factor.24,25 Confirmatory factor analyses were performed using Amos 26 for structural equation modeling to assess the adequacy of the CCAT’s factor structure identified in the EFA model. The maximum likelihood estimator was used to carry out the confirmatory factor analysis. Several fit indices were employed to determine how well the proposed model fitted the sample data. First, the Chi-square statistic was used as a measure of fit between the sample covariance and fitted covariance matrices. In addition to the Chi-square statistic, other fit indices were used to evaluate them, including the Comparative Fit Index (CFI) and the Tucker Lewis Index (TLI). The model with values >0.9 for the CFI and TLI indicates a reasonable fit.26,27 The Root Mean Square Error of the Approximation (RMSEA) and Root Mean Square Residual (RMR) were the other fit indexes that were taken into account to assess the model’s fitness. RMSEA and RMR values of less than 0.8 warrant a good model fit. 28 The construct validity of the tool was assessed using convergent and discriminant validity. Convergent validity assesses the level of agreement between various indicators of the same construct. To establish convergent validity, the indicator’s factor loading, composite reliability (CR), and average variance extracted (AVE) must be taken into account.29,30 The values are between 0 and 1. The AVE value should be greater than 0.50, and the CR value should be greater than 0.7 to ensure convergent validity.30–32
Discriminant validity is considered to be the degree to which each item measures only one construct and nothing else. 33 For acceptable discriminant validity, the square root of a specific latent variable’s AVE should be greater than the correlation between the specific latent variable and other latent variables. 31
Result
Socio-demographic status of study participants
Out of the 422 mothers involved in this study, 410 participated, yielding a response rate of 97.2%. The mothers’ mean age was 28.9 years (SD ± 5.27). The minimum age was 18; the maximum age was 43. More than three-fourths (385, or 85.9%) of the mothers surveyed are married. More than half of all respondents are housewives and farmers (29.3% and 23.9%), respectively, with the majority (60.5%) earning 2000 Ethiopian birr or more each month. 65.5% of respondents reside in urban areas (Table 1).
Socio-demographic status of study participants for cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool.

Validity and reliability analysis result
Exploratory factor analysis
For this study’s sampling adequacy, the KMO measure of adequate sampling was 0.95. Meanwhile, Bartlett’s test of sphericity was also significant for the sample (x² = 7664.4, df = 190, p < 0.001). The overall reliability (Cronbach’s alpha value) was 0.95, and the reliability statistics for the subscales indicate 0.90 for meaningful connection, 0.85 for patient expectation, 0.89 for caring attribute, and 0.96 for capable practitioner (Supplemental file 1).
Out of the 20 items, 13 had high loadings regarding their intended factors, while seven items (i.e., MC1, MC2, MC7, PE4, CA1, CA2, and CA3) had cross loadings on two of the factors. As a result, the items were dropped. Moreover, the analysis was carried out for the remaining 13 items (Table 2).
Factor loadings for exploratory factor analysis with varimax rotation of the 20 items of CCAT for cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool.

The KMO, Bartlett’s test of sphericity, and determinant of the R matrix were evaluated again to determine the data’s suitability for factor analysis on the remaining 13 items. The KMO was determined to be 0.9. Bartlett’s test of sphericity was significant for the sample (x2 = 4473.3, df = 78, p < 0.001), and the determinant of the R matrix value was 0.01. Furthermore, residuals were calculated between observed and reproduced correlations. There were 8 (10%) non-redundant residuals with absolute values greater than 0.05, indicating that the EFA model was fit. The result of the scree plot (Figure 1) yielded a three-factor structure, with factor loadings of items that settled at each subscale of the CCAT with three factors, which accounted for 69.9% of the total variance (eigenvalue = 9.92). The reliability statistics showed that the overall Cronbach’s alpha value for the 13 items was 0.92. The reliability for the subscales was 0.92 for patient expectation, 0.96 for capable practitioner, and 0.80 for meaningful connection (Table 3).
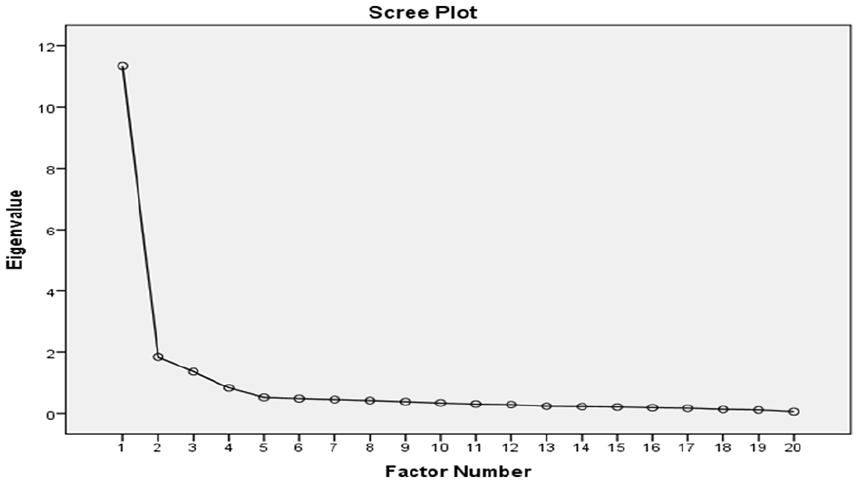
Scree plot of the 20 CCAT items for cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool.
Factor loadings of exploratory factor analysis with varimax rotation for the 13 items of the CCAT for cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool.

Confirmatory factor analysis
Model fit
This model consisted of three components: patient expectation, capable practitioner, and meaningful connection. Table 4 summarizes the measurement model’s goodness-of-fit test findings. Statistics for CFA are shown in Figure 2, Supplemental file 2, and Table 5. Compared to the recommended values for the goodness of fit tests, the values of GFI, CFI, TLI, RMR, RMSEA, and RMR were satisfactory, while the value of the Chi-square’s p-value was not (Table 4). However, since the sample size was large, the p-value could have been affected by the sample size.
Results of fit indices of confirmatory factor analysis model fitness for cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool.


Three factor model of the CCAT with standardized estimates and co-variance between errors for cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool.
Convergent and discriminant validity for Cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool.

The 13 items were all statistically significant at the 0.05 level, with standardized factor loadings ranging from 0.65 to 0.98. Therefore, the fit statistics associated with this model verified the recommended structure of the CCAT (Supplemental file 2).
Convergent and discriminant validity
All three latent variables (factors) had CR values larger than 0.7 and AVE values greater than 0.5. Furthermore, the square root of each specific latent variable’s AVE was greater than the correlation between the specific latent variables and the other latent variables. as indicated in Table 5.
Discussion
The CCAT was evaluated to ensure that it accurately examines compassionate care and that the questions are understandable. The content of the tool was conceptually anchored in the various tool development phases. 7
The lack of validation in many societies and cultures was identified by a comprehensive and critical review as one of the shortcomings of the compassionate evaluation instruments used in health services. 34 Clinical measurements of compassion must undergo measurement validation in order to be used to assess, enhance, and advance clinical practice, healthcare quality, and patient-reported outcomes. 34 Hence, this study was conducted to overcome the above-mentioned shortcoming of the lack of a validated tool for the assessment of compassionate care among obstetric service users in the Amharic language and the Ethiopian context.
Each aspect underwent a thorough tool translation and cultural adaptation procedure in order to adapt it to the target culture while preserving its original meaning and intent. Based on EFA, the PAF with Varimax rotation, this study yielded a three-factor structure with thirteen items. On CFA all 13 items had standardized factor loadings ranging from 0.65 to 0.98. As a result, the fit statistics of this model confirmed the proposed structure of the Compassionate Care Assessment Tool. All three latent variables (factors) have CR values greater than 0.7 and AVE values greater than 0.5, which is appropriate. Thus, the variables’ convergent validity was confirmed. Furthermore, the square root of each specific latent variable’s AVE was greater than the correlation between the specific latent variables and the other latent variables, confirming the study’s discriminant and convergent validity.
The findings of this study propose a 3-factor structured CCAT, which is similar to the Greek version of CCAT, whose analysis suggested a three-factor solution. 35 Based on the EFA, seven items were removed due to low factor loadings and cross loadings consequently, the original 20 item tool proposed was not retained and it was reduced to a 13 item tool. 7 Furthermore, Cronbach’s alpha coefficient of 0.92 indicated that the internal consistency of the 13 CCAT items and their three components was adequate. These findings are consistent with the original developed tool, the validated Greek version, and the validated Persian version of CCAT, which obtained Cronbach’s alpha >0.70, 0.94, and 0.92 respectively, for the whole tool and its proposed factors.7,35,36
Regarding the confirmatory factor analysis, the results of the discriminant validity show that the composite reliability (CR) of the 13 items was greater than 0.7 and the AVE values AVE were greater than 0.5, indicating convergent validity. This finding is similar to the original tool proposed and the Greek version, which assured the convergent validity of the proposed tools.7,35
The discriminant validity result showed that the square root of the AVE of the latent variables (factors) was greater than the correlation between the latent variable and the other latent variables, demonstrating the discriminant validity of the Amharic version of the compassionate care assessment tool. This finding is consistent with the original CCAT and demonstrates the tool’s discriminant validity. 7
The findings of the study showed that the validated Amharic version’s three-factor CCAT structure with the 13 items can adequately measure the provision of compassionate care among obstetric service users in Ethiopia.
Strength of the study
This study is one of the first studies on cross-cultural adaptation and validation of a compassion care assessment tool for applicability among obstetric service users in Ethiopia, with the use of a larger sample size. The tool confirmed a three-factor structure, which can be helpful to assess dimension-related status in compassionate care.
Limitations
This study included mothers who gave birth in public health facilities only; as a result, the validity of the tool to be applied in private health facilities and to other service users may be in question. Face and content validity were also not conducted as data collection began at the heart of the COVID pandemic first case finding in Ethiopia, which made creating an expert panel and conducting discussions more difficult. Virtual means were also challenging, as the cost and access to the internet were challenging. Due to the inaccessibility of study participants for a second interview, a test and retest were also not conducted.
Conclusion and recommendations
The Amharic version of the CCAT was shown to have strong internal consistency and adequate structural, convergent, and discriminant validity among obstetric service users in this study. Given its validity, it is concluded that the-three factor structured CCAT with thirteen items can be used to assess compassionate care practice among obstetric service users in Ethiopia. Therefore, we recommend researchers and service providers use this tool to measure the level of compassionate care provision in the provision of obstetric services.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241254992 – Supplemental material for Cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool for application in obstetric services of the Ethiopian context
Supplemental material, sj-docx-1-smo-10.1177_20503121241254992 for Cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool for application in obstetric services of the Ethiopian context by Amanuel Yosef Gebrekidan, Adane Kebede, Nigusu Worku, Afework Alemu Lombebo, Amelework Gonfa Efa, Gedion Asnake Azeze, Gizachew Ambaw Kassie, Kirubel Eshetu Haile, Yordanos Sisay Asgedom, Beshada Zerfu Woldegeorgis, Solomon Abrha Damtew and Selamawit Gebeyehu in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241254992 – Supplemental material for Cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool for application in obstetric services of the Ethiopian context
Supplemental material, sj-docx-2-smo-10.1177_20503121241254992 for Cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool for application in obstetric services of the Ethiopian context by Amanuel Yosef Gebrekidan, Adane Kebede, Nigusu Worku, Afework Alemu Lombebo, Amelework Gonfa Efa, Gedion Asnake Azeze, Gizachew Ambaw Kassie, Kirubel Eshetu Haile, Yordanos Sisay Asgedom, Beshada Zerfu Woldegeorgis, Solomon Abrha Damtew and Selamawit Gebeyehu in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121241254992 – Supplemental material for Cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool for application in obstetric services of the Ethiopian context
Supplemental material, sj-docx-3-smo-10.1177_20503121241254992 for Cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool for application in obstetric services of the Ethiopian context by Amanuel Yosef Gebrekidan, Adane Kebede, Nigusu Worku, Afework Alemu Lombebo, Amelework Gonfa Efa, Gedion Asnake Azeze, Gizachew Ambaw Kassie, Kirubel Eshetu Haile, Yordanos Sisay Asgedom, Beshada Zerfu Woldegeorgis, Solomon Abrha Damtew and Selamawit Gebeyehu in SAGE Open Medicine
Supplemental Material
sj-docx-4-smo-10.1177_20503121241254992 – Supplemental material for Cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool for application in obstetric services of the Ethiopian context
Supplemental material, sj-docx-4-smo-10.1177_20503121241254992 for Cross-cultural adaptation of the Amharic version of the Compassionate Care Assessment Tool for application in obstetric services of the Ethiopian context by Amanuel Yosef Gebrekidan, Adane Kebede, Nigusu Worku, Afework Alemu Lombebo, Amelework Gonfa Efa, Gedion Asnake Azeze, Gizachew Ambaw Kassie, Kirubel Eshetu Haile, Yordanos Sisay Asgedom, Beshada Zerfu Woldegeorgis, Solomon Abrha Damtew and Selamawit Gebeyehu in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our gratitude to the study participants and data collectors of this study.
Author contributions
AYG: conceived and designed the study, methodology, and data analysis, and participated in interpretation and writing the original draft. AK: participated in supervision, software, data analysis, and writing the original draft. NW: Participated in supervision, software, data analysis, and writing the original draft. GAK: participated in data cleaning, data analysis, and writing the original draft. YSA: participated in software, data analysis, and editing the manuscript. BZW: participated in data cleaning, and writing the original draft. GAA: co-conceived and designed the study, conducted data analysis, and participated in interpretation and writing the original draft. KEH: participated in data cleaning and writing the original draft. AAL: Participated in supervision, software, data analysis, and writing the original draft. AGE: participated in data analysis and editing of the manuscript. SA: conceived and planned the data analysis, participated in the data analysis, and edited the manuscript, and SG: participated in designing the study, data entry, analysis, and writing the original draft. All authors participated in the software, writing review, and editing of the manuscript. All the authors read and approved the manuscript.
Data availability
All relevant data regarding this research work is included in the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The ethical review committee of the Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, provided ethical clearance with reference number Ref. No. IPH/837/6/2012 E.C. The department of health systems and policy, as well as the hospitals’ chief clinical directors, wrote letters of support.
Informed consent
Written informed consent was obtained from all subjects before the study. Illiterate individuals who can sign provided their signature, while those who cannot sign put X as a sign of consent.
Consent to participants
All responders were provided an explanation of the study’s objective and procedures. Each responder gave written informed consent after receiving information about the study’s goal, the benefits of participation, and the right to withdraw at any time. Participants were also informed that the data would be kept confidential and that no information would be shared with a third party. Illiterate individuals who can sign provided their signature, while those who cannot sign put X as a sign of consent. The Helsinki Declaration of Human Research was followed throughout the scientific assessment of this project.
Consent for publication
Not applicable.
Trial registration
Not applicable.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.