
Abstract
Objectives:
To map the evidence on the barriers to and facilitators of diagnosing noncommunicable diseases among people living with HIV in low- and middle-income countries in Africa.
Introduction:
Noncommunicable diseases are increasing among people living with HIV. Thus, strengthened and sustained diagnosis of noncommunicable diseases through integrated noncommunicable diseases and HIV care is needed to improve patient outcomes. However, there is paucity of evidence on the barriers and facilitators diagnosing noncommunicable diseases among people living with HIV in low- and middle-income countries.
Methods:
The Arksey and O’Malley methodological framework was used. A comprehensive systematic search of academic databases (MEDLINE, Academic Search Complete, APA PsycInfo, CAB, and Health Source/Nursing) was performed via EBSCO search and PubMed. The articles were reviewed independently by three reviewers. The results were structured using Capability-Opportunity-Motivation-Behavior model and Theoretical Domains Framework.
Results:
A total of 152 articles were retrieved for full-text review. Forty-one articles met the inclusion criteria. The identified barriers were relevant to all the Capability-Opportunity-Motivation-Behavior constructs and 14 Theoretical Domains Framework domains. A lack of knowledge and awareness of noncommunicable diseases, fear of stigma, financial problems and out-of-pocket payments were the most cited patient-level barriers. Healthcare providers (knowledge and awareness gaps, skill and competence deficiencies, unwillingness, burnout, low motivation, and apathy) were frequently cited. Lack of equipment, noncommunicable disease medications and supply chain challenges, lack of integrated noncommunicable disease and HIV care, and shortage of trained healthcare providers were identified as health-system-level barriers.
Conclusion:
This scoping review is the first to identify barriers and facilitators using a theoretical framework. The most cited barriers include a lack of integrated HIV and noncommunicable disease care, equipment and logistics chain challenges for noncommunicable diseases, patients’ and healthcare providers’ lack of knowledge and awareness of noncommunicable diseases, and healthcare provider’s skill and competency deficiencies. Addressing these issues is crucial for improving patient outcomes and reducing the burden on healthcare providers and health systems.
Introduction
Noncommunicable diseases (NCDs) pose a global public health challenge and account for three-quarters of deaths globally.1,2 NCDs are more prevalent in low- and middle-income countries (LMICs) than in high-income countries, with an earlier age of onset and increased premature mortality. 3 Furthermore, persons living with HIV (PLWH) are exposed to the same NCD risk factors as their HIV-negative counterparts and may be exposed to additional risk factors as a result of contracting HIV and some antiretroviral therapy (ART) medications.1,4 The multimorbidity of HIV and NCDs affects PLWH compared to the general population, contributing to decreased health-related quality of life, increased hospitalization, and increased risk of death.5,6
The availability of ART has improved life expectancy. 7 However, in the ART age, along with increasing life expectancy, there is increased vulnerability to NCDs, and multimorbidity remains.5,6 PLWH have a higher incidence and prevalence of NCDs such as depression, cardiovascular disease (CVD), cervical cancer, diabetes, obesity, and hypercholesterolemia than people without HIV1,8–12; CVD is one of the leading causes of non-AIDS morbidity and death among PLWH.1,9,13
In LMICs, there is a substantial burden of comorbid NCDs among PLWH,14–16 especially NCDs, which are increasing among PLWH in sub-Saharan African (SSA) countries. 8 As the burden of NCDs among PLWH in LMICs increases, the quality of life and health benefits associated with HIV/AIDS are at risk.15,16 As a result, PLWH may require frequent screening for NCD detection, diagnosis, and treatment.17,18 However, LMICs in African countries struggle to manage growing chronic NCDs, as health systems primarily provide episodic care for acute symptomatic conditions. 19
The growing burden of HIV infection and NCD comorbidity implies a focus on healthcare systems that provide chronic multimorbidity care in an integrated manner 20 ; thus, there have been increased calls for the integration of HIV and NCD services to increase efficiency and improve the coverage of NCD care. 21 Furthermore, the needs of PLWH with multimorbidities are critical since they are more prone to care fragmentation due to the involvement of several health providers.22,23 For PLWH, the provision of NCD care and outcomes may be inferior to those of their HIV-negative counterparts. 6 The barriers to CVD screening and management across the patient, provider, and health system levels in LMICs among PLWH require urgent attention. 7 Some barriers include a lack of adequate knowledge and perceptions of NCDs among patients and providers. 7
Strengthening health-system-based approaches to NCD risk factor measurement at appropriate and routine intervals and empowering patients and healthcare providers to respond to NCDs need due attention; in particular, more emphasis is required to address the growing multiple chronic care needs of PLWH. 7 However, there is a paucity of evidence on the barriers to and facilitators of the early detection and diagnosis of NCDs among PLWH in LMICs. Therefore, the current scoping review aimed to systematically map evidence on the barriers to and facilitators of the diagnosis of NCDs, with a focus on depression, hypercholesterolemia, hypertension, obesity, and diabetes for PLWH in LMICs in Africa.
Methods
This scoping review was carried out following the method suggested by Arksey and O’Malley 24 ; The following five steps were used: Step 1: Identifying the research question; Step 2: Searching relevant studies; Step 3: Selecting appropriate studies; Step 4: Charting the data, and Step 5: Collating, summarizing, and reporting the results. The optional step 6, consultation with relevant stakeholders, has been excluded from this review. The incorporation of recommendations made by Levac and colleagues 25 was considered. A scoping study approach enables systematic searching, selecting and examining literature, knowledge synthesis, and mapping of evidence to address research questions. 24
The Preferred Reporting Items for Systematic Reviews extension for Scoping Reviews (PRISMA-ScR) proposed by Tricco et al. 26 was used to present the scoping review report. The PRISMA-ScR provides a reporting guideline containing 20 essential items and two optional items included in scoping reviews. 26 This guideline also facilitates methodological transparency and acceptance of research findings. 26 The protocol for this scoping review has been registered on the Open Science Frameworks (https://osf.io/xvtwd/).
Step 1: Identifying the research question: The present scoping review aims to answer the following questions:
What are the barriers to diagnosing major NCDs (depression, hypercholesterolemia, hypertension, obesity, and diabetes) among PLWH in LMICs in Africa?
What are the facilitators of diagnosing major NCDs (depression, hypercholesterolemia, hypertension, obesity, and diabetes) among PLWH in LMICs in Africa?
The research question was identified using the people concept and context framework approach (Table 1).
People, concept, and context used to identify review questions.

Step 2. Identifying relevant studies
Information sources
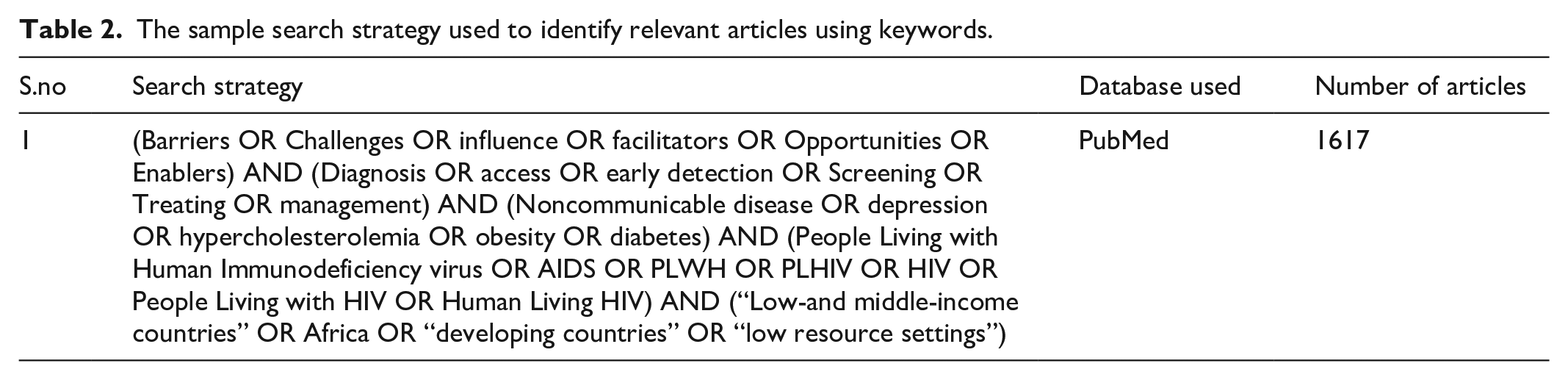
A thorough systematic search was carried out in the MEDLINE, Academic Search Complete, APA PsycInfo, CAB, and Health Source/nursing academic databases retrieved using the EBSCO search engine, as well as PubMed for advanced searches. A comprehensive search strategy based on medical subject headings (MeSH) and keywords was employed. Boolean terms (AND and OR) were used to separate keywords, and MeSH was used in the advanced search of articles. After an advanced search of the included studies from the database, further relevant papers from the reference list were scanned or tracked as a secondary search using the snowball technique.
A sample of the search strategy was used (Table 2).
The sample search strategy used to identify relevant articles using keywords.
Step 3. Study selection
Three authors independently evaluated the titles and abstracts of the included articles. Full-text papers were collected for all eligible titles and abstracts, and three authors independently reviewed the full-text publications to determine which articles should be included in the review based on eligibility criteria.
The eligibility criteria
This scoping review consisted of the following eligibility criteria for including articles in this scoping review:
Studies involving people living with HIV
Studies on the diagnosis of NCDs in PLWH have focused on depression, hypercholesterolemia, hypertension, obesity, and diabetes.
Studies from LMICs in Africa.
All research designs (interventional, observational, mixed, quantitative, and qualitative).
We decided to include studies published between 2013 and 2023 in this scoping analysis to acquire new information on NCDs after the World Health Assembly endorsed the Global NCD Action Plan in 2013. 27
Exclusion criteria
Non-English language articles were excluded due to time constraints, financial limitations, and a lack of language resources and language abilities in the review team to address non-English studies and access to non-English databases.
Selection process
The three review authors conducted a thorough title screening using electronic databases guided by eligibility criteria. All relevant articles were imported into an EndNote library. Then, the articles were uploaded to the online reviewing system Rayyan (Qatar Computing Research Institute) 28 software for deduplication and were shared with the review team for the next stage of the study screening and selection process. Duplicate records were checked and removed. A screening process for the abstract and full-text screening phases was developed using eligibility criteria. Three review authors independently completed the abstract and full-text screening phases and collected data to include categories. Discrepancies in abstract screening were addressed through discussion by the review team until a consensus was reached. The PRISMA flow diagram 29 was used to report the screening results (Figure 1).

PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases, registers and other sources.
Step 4: Charting the data
Microsoft Excel was used for the extraction of data. All relevant data from the included articles including study authors, title, country/setting, aim/purpose of the study, sample size, study design, population, and type of NCDs were extracted after the full texts were read, and the study characteristics, including the study authors, title, country/setting, aim/purpose, and findings relevant to the review question were extracted.
Step 5: Organizing, summarizing, and reporting the findings
Scoping reviews, according to Arksey and O’Malley, 24 require thematic frameworks to present narrative accounts of selected literature. The qualitative software NVivo version 12 was used to organize the data, and thematic analysis was performed. The data were grouped thematically by reading and rereading the data items and grouping similar/related items into iteratively developed themes. The data were analyzed and synthesized using a data-driven bottom-up approach. Thomas and Harden’s 30 thematic synthesis method was used to inductively code, develop, and generate themes from the barriers and facilitators identified across the included studies. Inductive data-driven themes were deductively categorized using the relevant domains of the COM-B model31,32 and the TDF.33,34
Each theme was analyzed and mapped to the COM-B system construct and the 14 TDF domains and categorized as patient-, provider-, and health-system-level barriers and facilitators of diagnosing NCDs. To confirm that the theme was correctly mapped to the TDF domain, we double-checked that the extracted data inside each theme matched the domain content (i.e., the component constructs in each TDF domain). TDF domains were mapped to COM-B components as defined by Cane and colleagues. 33 Disagreements among the reviewers were settled by consensus. The results were tabulated, and a narrative synthesis of the findings was provided, structured around the themes of barriers and facilitators at the patient, provider, and health system levels.
Step 6: Methodological quality appraisal
A methodological quality appraisal step is not mandatory in scoping reviews, and this step was excluded from the current scoping review.
Results
A total of 2326 articles were retrieved, exported to the EndNote library, and imported to Rayyan for deduplication and further review. Three reviewers independently screened 2309 articles’ titles and abstracts; disagreements in 42 articles were resolved through discussion. Finally, 148 articles were included for full-text review, and four additional articles were identified from the references of the selected articles. A total of 152 articles were retrieved for full-text review. The full texts of 152 records were screened, resulting in 41 articles meeting the inclusion criteria and reported in the current scoping review.
Study characteristics
Twenty-eight articles in the review identified barriers to diagnosing NCDs (hypertension and diabetes).14,15,20,35–61 The included studies reported barriers to and facilitators of diagnosing depression among PLWH.42,50,62–73 Two studies reported both NCDs and depression. No studies included in this review reported the barriers to and facilitators of diagnosing hypercholesterolemia and obesity.
Among the included 41 articles met the inclusion criteria (16 cross-sectional, 2 cohort, 1 case-control, and 5 RCTs, as well as 9 qualitative, 4 mixed, 2 commentary, and 2 review studies) (Table 3).
Descriptive characteristics of the final included studies.

The theoretical framework used for the analysis of the findings
The barriers to diagnosing NCDs (hypertension, diabetes, and depression) identified were mapped to the domains of the Capability-Opportunity-Motivation-Behavior system (COM-B)/Theoretical Domains Framework (TDF). According to the COM-B model, behavior change depends on an individual having the capacity, opportunity, and motivation to change their behavior/practice.31,32 The TDF is a 14-domain model that builds on the COM-B model to better understand the underlying barriers to and facilitators of evidence-based behavior change33,34 and is used to analyze and present this scoping review (Figure 2).

Barriers to the diagnosis of NCDs
Barriers to diagnosing NCD among PLWH presented using the COM-B domain and TDF theoretical domain as patient-, provider-, and health-system-level barriers.
Capability construct of COM-B: The COM-B model’s capability domain corresponds to an individual’s psychological (involving a person’s mental function) and physical capability (involving a person’s physique and musculoskeletal function) to participate in an activity.
The psychological component of the capability domain of behavioral change model includes knowledge and the ability to comprehend information and to reason, while the physical component of capability includes skill, dexterity, and strength required for the behavior change practices. Barriers and facilitators were not identified under physical capability domain in this review.
Knowledge
Knowledge (TDF domain) was reported as a barrier at the patient and provider levels.
Patient level barriers
Seven included studies from Zambia, South Africa, Zimbabwe, Tanzania, and Nigeria reported inadequate patient knowledge and low awareness of NCDs,35–40 including poor mental health awareness and poor health-seeking behavior related to depression, 42 as a barrier to the early diagnosis of NCDs.
Provider level barriers
Nine studies from SSA, including Zambia, Uganda, Zimbabwe, Tanzania, Senegal, Ivory coast, Nigeria, and Malawi, reported that HCPs’ had inadequate knowledge and awareness of NCDs, including depression.15,35,36,41,42,50,62–64 Among these studies, five reported a lack of knowledge of HCPs in depression screening and management.42,50,62–64 For example, HCPs perceive depression as a logical outcome of HIV infection and perceive it as difficult to diagnose. 62 In addition, HCPs’ lack of confidence in prescribing depression drugs resulting from inadequate training on depression and mental health.50,63,64 was reported as a barrier to diagnosing NCDs.
Skills
The skill domain of TDF was identified as a provider-level barrier. Four studies from South Africa, Tanzania, and Zimbabwe40,43,44,65 reported HCP deficiency in diagnosing NCDs, mainly due to inadequate training and practice. For example, three studies reported that HIV clinic HCPs had inadequate skills to detect and manage NCD in the context of HIV care.40,43,44 Newly trained nurses come into practice without proper training in diagnosing and managing NCD. 44 In addition, the use of unstandardized screening tools resulted in the inclusion of participants who were not clinically depressed, 65 which was reported a provider-level barrier.
Memory, attention, and decision processes
Two studies identified the memory attention and decision process domains as barriers. Studies from Uganda and Tanzania reported a gap in patient–provider communication and discussion.35,41 For instance, a study conducted in Tanzania reported that PLWH with comorbid hypertension did not inform their HIV status to hypertension care providers and their hypertension status HIV care providers because these two diseases are managed in different clinics and by different providers. 35
Behavioral regulation
Two studies from Zimbabwe and South Africa reported the behavioral regulation of the TDF domain at the patient and provider levels as barriers.45,46 For example, a study from Zimbabwe reported patients’ preference for the use of alternative medication, 46 and a South African study reported disrespectful treatment by staff. 45
Opportunity construct of COM-B
The opportunity domain has two subcomponents. Physical opportunities are created by environments, for example, access to resources that enable factors or hinder toward the practice of intended behavior. Social opportunities are norms and expectations of the social environment, which could be facilitators of or hindrances to intended behavior change practices. The environmental context and resources and the social influence of the TDF domains were identified as patient-, provider- and health-system-level barriers under physical opportunity for behavioral change.
Physical opportunity
Environmental context and resources
The environmental context and resources of the TDF domain were frequently reported as patient-, provider-, and health-system-level barriers.
Patient-level barriers
Transportation and long travel distance
Five studies from South Africa, Eswatini, Zimbabwe, and Tanzania reported patients’ transportation problems and the need to travel long distances.35,40,45,47,48 For example, two studies conducted in South Africa and Zimbabwe reported increased transportation costs to patients,45,48 whereas a lack of funding for patients for transportation was reported in Tanzania, Eswatini, and South Africa.35,47
Financial constraints and out-of-pocket payments
Six studies conducted in Uganda, South Africa, Zimbabwe, and Tanzania reported financial constraints, and higher OOP40,46,48–50,66 was reported. For example, studies conducted in Tanzania and Zimbabwe reported that due to financial constraints caused by poverty, PLWHs failed to visit clinics for depression diagnosis and care.50,66
Provider-level barriers
Six studies conducted in South Africa, Tanzania, Zimbabwe, Malawi, and Kenya reported inadequate training for HCPs on NCD screening and management.40,43,44,50–52 For instance, a South African study reported that an imbalance in HIV and NCD training and practice leads to newly trained nurses who come into practice without proper training on NCD. 44
Health-system-level barriers
Health-system-level barriers were frequently reported in the environmental context and resources domain of the TDF.
Inadequate number of trained HCPs
Sixteen studies conducted in SSA, including Namibia, Uganda, South Africa, Zimbabwe, Tanzania, Malawi, Kenya, Senegal, Cotidivor, and Nigeria, reported inadequate numbers of HCPs trained on NCDs35,40,41,43,48,51–53 including depression screening and diagnosis.42,50,62–64,68–70
Lack of NCD equipment and screening tools
Eight studies from Uganda, Zimbabwe, Tanzania, South Africa, Malawi, and Zambia reported a lack of equipment for NCD prevention, including depression screening and diagnosis.41,43,44,48,50,51,62,67 For example, lack of blood pressure (BP) measurement devices and random blood sugar (RBS) machines and strips41,43,44,48,51 and malfunctions of BP machines, 53 a lack of laboratory testing 48 , and a lack of standard, validated, culturally sensitive screening tools and therapies for depression and mental health problems.50,62,67 have frequently been reported.
NCD drug, medication, and supply chain problems
Eight studies from SSA, including Namibia, Uganda, Zimbabwe, Tanzania, and Malawi, reported NCD drugs, medication shortages, and supply chain difficulties.35,41,43,48,51,53–55 For example, stock out of NCD medications,43,51,53,54 including the nonavailability of HTN and DM medication at ART sites,35,41,48 and challenges of NCD drug supply chains44,47,54,55 were reported.
Lack of integrated NCDs and HIV care
Eleven studies from SSA, including Namibia, South Africa, Mozambique, Zimbabwe, Tanzania, Malawi, and Senegal,14,15,35,51,53,57,62–64 reported a lack of integrated HIV and NCDs, including depression screening among PLWH. For example, lack of active and routine screening of NCD offered as part of HIV care delivery.14,15,53,57 A study from Mozambique reported poor integration of hypertension screening and management with chronic care services. 56
Long waiting times
Six included studies from Uganda, South Africa, Zimbabwe, and Tanzania reported long distances and long waiting times.20,35,40,41,48,49
Lack of health system readiness
Three studies from Zambia, Mozambique, and Zimbabwe reported the limited capacity of ART clinics and lack of health system readiness for NCD services.36,56,58
High out-of-pocket payments
Six studies from SSA, including Zimbabwe, Tanzania, Kenya, and Uganda, reported that high OOP payments and high costs of services35,46,48,52,54,55 were barriers.
Lack of NCD guidelines and guidance
Four studies from South Africa, Kenya, and Nigeria reported a lack of updated guidelines for managing NCDs, including depression screening and diagnosis.40,42,44,52 For instance, the updated guidelines are unavailable for PHC facilities in South Africa.44,52 At the same time, a systematic review conducted in SSA reported that a lack of standard screening tools and culture-sensitive therapies for depression 62 were identified as barriers.
Social opportunity
Four studies from Tanzania, South Africa, Nigeria, and Zimbabwe35,40,42,66 reported the social opportunity of the TDF domain as a barrier to patients, providers, and health systems. At the person level, a lack of clear communication and discussion with HCP providers and patients’ fear of stigma and isolation due to their HIV and mental health issues were reported as barriers. In addition, at the provider level, gaps in communication and clear discussion with patients and HCP-related stigma were reported as barriers. Due to the lack of HIV and chronic disease support programs, poor information provided to patients on chronic disease and medication not delivered on time were identified as health-system-level barriers. For instance, a study from Tanzania reported gaps in patient and HCP communication and discussion. 35 A South African study reported poor information provided and a lack of chronic care support programs, 40 whereas studies from Nigeria and Tanzania reported PLWH fear stigma associated with HIV and mental health problems and cultural ignorance. 42
Motivation construct of COM-B
Motivation is an aggregate of mental processes that energizes and directs behavior. The motivation domain of the COM-B can be either automatic (such as habits) or reflective motivation (such as planning and decision-making). Beliefs about the capabilities, intentions, optimism, goals, and social/professional role domain of TDF were identified as patient-, provider-, and health-system-level barriers.
Beliefs about the capabilities
Five studies from South Africa, Nigeria, Malawi, and Zimbabwe reported low confidence and beliefs about the ability of HCPs to diagnose NCD, including depression and mental health.20,42,44,50,64 For example, a study in South Africa reported that a lack of HCP confidence in managing NCDs in a PHC facility contributes to the underdiagnosis of NCDs, 44 whereas HCPs believe that specialized clinics could offer better care for HIV infection and that NCDs are neglected. 20 A study in Malawi reported that nonspecialized mental healthcare workers feel that they need more time to treat mental health problems, 64 which were identified as provider-level barriers.
Intention
Twelve studies from SSA, including South Africa, Mozambique, Senegal, Uganda, Ethiopia, Tanzania, Nigeria, and Malawi,20,40,41,56,59,60–62,64,71,72 reported a lack of attention given to NCDs, including depression as a patient-, provider-, and health-system-level barrier.
Beliefs about the consequences
One study from Zimbabwe reported concerns about pill burden and possible interactions with ART drugs with NCDs 50 as barriers at the patient level.
Optimism
Two studies from Mozambique and Nigeria42,56 reported barriers in the optimism domain of TDF. For example, a lack of HCP motivation 56 and burnout 42 were identified as provider-level barriers.
Goals
Three studies from Namibia, Uganda, and South Africa41,53,57 reported TDF’s goal domain as a barrier to diagnosing NCDs. For instance, even though the PLWH have frequent follow-ups in HIV clinics, NCDs were underdiagnosed, undertreated, and poorly controlled. 57
Social/professional role
Five studies from Tanzania, South Africa, Uganda, Senegal, and the Ivory Coast35,41,44,63,66 reported barriers. For instance, a lack of open discussion with patients, HCPs and patients was identified as a patient-level barrier, 35 whereas nurses who feel that an NCD diagnosis is the responsibility of medical doctors, 44 provider apathy, 41 and HCP perception of diagnosis and management of depression needed to be performed by a specialist 63 were identified as provider-related barriers (Table 4).
Barriers to diagnosing NCD among PLWH using COM-B and TDF included in studies of a scoping review.

Facilitators for diagnosing depression among PLWH
Four studies from South Africa, Nigeria, and Zimbabwe42,50,68,73 reported facilitators of the diagnosis of depression.
Environmental context and resource domain of TDF
Three studies from South Africa and Nigeria identified TDF’s environmental context and resource construct as a health-system-level facilitator.42,68,73 For instance, a study reported that leveraging existing HIV/AIDS structures could help individuals diagnose depression. 42 The Nigeria and South Africa study reported a task-shifting approach,42,68 and utilizing available human resources from HIV care and engaging community health workers in mental health 42 could facilitate early diagnosis of depression.
Reinforcement
One study reported that reinforcement strategies such as providing incentives for bus fares and refreshments were identified as facilitators of diagnosis 50 (Table 5).
Facilitators for diagnosing depression among PLWH using the COM-B and TDF frameworks included studies in the scoping review.

Discussion
The findings of this scoping review provide an overview of the available literature on the barriers and facilitators of diagnosing NCDs (hypertension, diabetes, and depression) among PLWH in LMICs of Africa. This review identified various barriers linked to the capability, opportunity, and motivation of the COM-B system and TDF domains. A theory-informed method combining the COM-B and TDF theoretical domains to map evidence systematically ensures the exploration of various behavioral determinants. Knowing how identified barriers align with theoretical understandings of behavioral changes is critical for improving intervention design and strengthening the likelihood of successful implementation. A broad range of barriers and potential unknown influences were identified that can be targeted in designing interventions to improve the diagnosis of NCD among PLWH with the increasing chronic care needs. Collectively, these studies provide corroborative evidence of barriers identified at the patient, provider, and health system levels for diagnosing NCD among PLWH.
All of the barriers and facilitators identified in the diagnosis of NCDs were relevant to all of the COM-B constructs and all of the 14 TDF domains (knowledge, skills, environmental context and resources, social influences, beliefs about capabilities, beliefs about consequences, social/professional role and identity, reinforcement, intentions, goals, and emotion). A large number of barriers were reported in the COM-B construct and TDF domains and categorized as patient-, provider-, and health-system-related barriers in the included studies.
At the patient level, the identified barriers to the diagnosis of NCD among PLWH were lack of knowledge and awareness of NCDs, patients longing for alternative medications, fear of the stigma associated with HIV and mental health problems, fear of pill burden, financial problems, and prohibitive OOP payments.
In LMICs, patients, particularly PLWH, face challenges in NCD care due to limited access to accurate information and prevailing social, economic, and cultural conditions 74 and a lack of awareness of their disease due to low health literacy and a lack of knowledge on NCDs and risk factors. 75 When compared to high-income nations, patients living with NCDs in LMICs rely on large OOPs to receive NCD care services. Thus, many people are unable to obtain NCD services because they are unable to pay for OOP. Many OOP expenses (medication, outpatient appointments, diagnostics, hospitalization, and transportation) exacerbate poverty. 76
Low knowledge, awareness, skill, competence deficiencies, lack of confidence due to inadequate training and practice, disrespectful care, unwillingness, burnout, low motivation, and apathy were cited as provider-level barriers for diagnosing NCD among PLWH. Our review report, which was consistent with the WHO report on the African region, indicated that health workers in PHC facilities have insufficient knowledge to diagnose and treat NCDs and provide counseling. 77
The main barriers at the health system level identified were lack of equipment, scarcity of NCD medications and supply chain challenges, lack of integrated NCD and HIV care, lack of health system readiness and guidelines, lack of monitoring and tracking patient referrals and documentation, and inadequately trained human resources and culture-sensitive therapies.
Our review findings were consistent with those of the WHO Africa Regional Report, which found that NCD services are limited, fragmented, and of poor quality. Furthermore, NCDs are not fully integrated into PHC services. Medicine stockouts are common, as are poor implementation and poor supply chain management systems. 77 A shortage of skilled human resources negatively impacts the delivery of NCD services. 77 The availability and affordability of NCD medicines and technologies are much lower in LMICs than in high-income countries (HICs).78,79
Patient-level obstacles could be addressed through activities that improve NCD literacy. Health literacy is critical for preventing and controlling NCDs. It could support people, communities, and organizations in addressing NCDs. 80 Improving health literacy on NCDs and risk factors and awareness creation activities focused on the patient level could be prioritized. Strategies that reduce OOP, such as health stewardship, creating resources, healthcare financing mechanisms, and delivering health services, could help address high OOP. 81
Qualified HCPs responsive to and embedded within communities should be selected with rigorous training and supervisor support. Training related to HCPs is critical for enhancing knowledge and skills on NCDs and could address motivational issues. An appropriately skilled and deployed primary care workforce can optimize the care and management of NCDs, a critical enabler for achieving UHC and realizing global health targets of SDGs. 82 There is a need to prioritize strengthening the health workforce for effective NCD care particularly for PLWH through integrated HIV and NCD services.
The health system can facilitate diagnosis by integrating NCDs, including mental healthcare, with HIV/AIDS services, including leveraging existing structures and implementing a task-shifting approach. Health systems should be strengthened to provide a consistent supply chain of essential drugs, an efficient system for their distribution to patients, and training on appropriate use.
Implication of the findings
The outcome of this study has broad implications for policy makers, decision makers, international and national donors, service providers, researchers, and associations such as people living with HIV and communities at large for NCD response in LMICs in Africa including Ethiopia, particularly for addressing gaps identified through health system strengthening, redesigning service provisions, research and funding to improve early detection and linkage to care to address the multiple chronic care needs of PLWH. Moreover, increase in NCDs among PLWH needs to be addressed by strengthening the PHC system through the design and implementation of evidence based interventions. Thus, this study plays a crucial role in identifying and mapping evidence on the barriers to and facilitators of the diagnosis of NCD among PLWH (at the individual, provider, and health system levels) in LMICs in Africa.
Limitations of the study
This review had the following limitations. We limited our search to English-only papers due to a lack of language experts on the review team. As with most reviews, there is a possibility that some papers could have been missed during the search process. It is also possible that some papers used terminologies different from what we used to search for literature. We did not consider the quality of the studies in the review while synthesizing the findings.
Conclusion
This scoping review is the first to identify barriers to and facilitators of diagnosing NCDs among PLWH using a theoretical domain of COM-B and TDF to map evidence. Various factors, including lack of knowledge and awareness, HCP skill deficiency and shortage of trained HCPs, lack of integrated care, and equipment and logistics chain challenges for NCDs hinder the diagnosis of NCDs among PLWH. Addressing these issues is crucial for improving patient outcomes and reducing the burden on HCPs in LMICs’ health systems struggling with acute care.
The integration of NCDs with HIV care at the PHC level is recommended, with sufficient resources to address supply difficulties and reduce patient OOP expenses for the sustained delivery of services to address the multiple chronic care needs of PLWH.
The contextual factors affecting the integration of NCDs with HIV care at the PHC level need to be explored through primary research.
Footnotes
Acknowledgements
The authors would like to thank the University of KwaZulu-Natal in South Africa, the Health Economics and AIDS Research Division (HEARD), for providing a PhD scholarship to the primary author and the Swedish International Development Cooperation Agency and Wolaita Sodo University in Ethiopia. The current scoping review protocol was published at Plos One journal ![]() .
.
Author contributions
ASB and OHM designed the review. ASB, DDW, and DBD screened articles. ASB analyzed the review article. ASB, DDW and DBD drafted the scoping review paper, while OHM reviewed the manuscript. All the authors have read and approved the manuscript.
Availability of data and materials
All data analyzed for and in this study are included in the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study did not involve human subjects.
Informed consent
Not applicable.
Consent for publication
Not applicable.