
Abstract
The management of intracranial malignancies in pregnancy poses unique challenges to the perioperative team. We describe the successful surgical management of a meningioma in a 28-year-old previously healthy patient, in her third trimester of pregnancy, who first presented with a generalised seizure. Without clear guidelines on the management of intracranial malignancies in pregnancy, a multidisciplinary approach was essential in providing a management plan for the patient’s seizures and on the timing of her surgical intervention. Hormone-mediated tumour growth was a significant factor in opting for urgent surgical intervention and we discuss the current evidence linking hormones to tumour growth in pregnancy.
Keywords
Introduction
Meningiomas are one of the most common primary intracranial malignancies to present in pregnancy, and they have an incidence of 5.6/100,000. 1 They usually occur in the second to third trimester of pregnancy which is thought to be related to hormone-mediated growth of meningioma. 2 Though there are a growing number of case reports on this topic there exists a lack of consensus guidelines. A multidisciplinary approach is therefore essential in managing such cases. Additionally, the anaesthesiologist must be familiar with both neurophysiological and obstetric anaesthetic principles to balance both the need for adequate cerebral perfusion and optimal intracranial operative conditions, with the maintenance of adequate uteroplacental perfusion. In this case report, we describe the management of a pregnant patient who presents with seizures secondary to an intracranial meningioma. We then discuss the current literature on meningioma growth in pregnancy which informed the timing of intervention in this case. The patient has provided her written consent for this case to be published.
Case report
A previously healthy 28-year-old primigravida of 29 weeks gestation presented to the emergency department following a self-terminating 3-min episode of generalised tonic-clonic seizure in the community. Her level of consciousness had returned to normal, and the clinical exam was unremarkable. The patient’s vital signs, including blood pressure, were within normal limits. She had no headache or visual symptoms and therefore eclampsia was not deemed a likely cause for her presentation. Her pregnancy history was uncomplicated. There was no significant prior medical or family history of note. Laboratory investigations were normal. An obstetric ultrasound revealed a single live foetus in the cephalic position of normal size with no abnormality of placental position or amniotic fluid volume.
A magnetic resonance imaging (MRI) brain revealed a 5.3 by 3.2 cm extra-axial dural-based mass consistent with meningioma, overlying the left frontal and temporal lobes with an associated moderate mass effect (Figure 1).
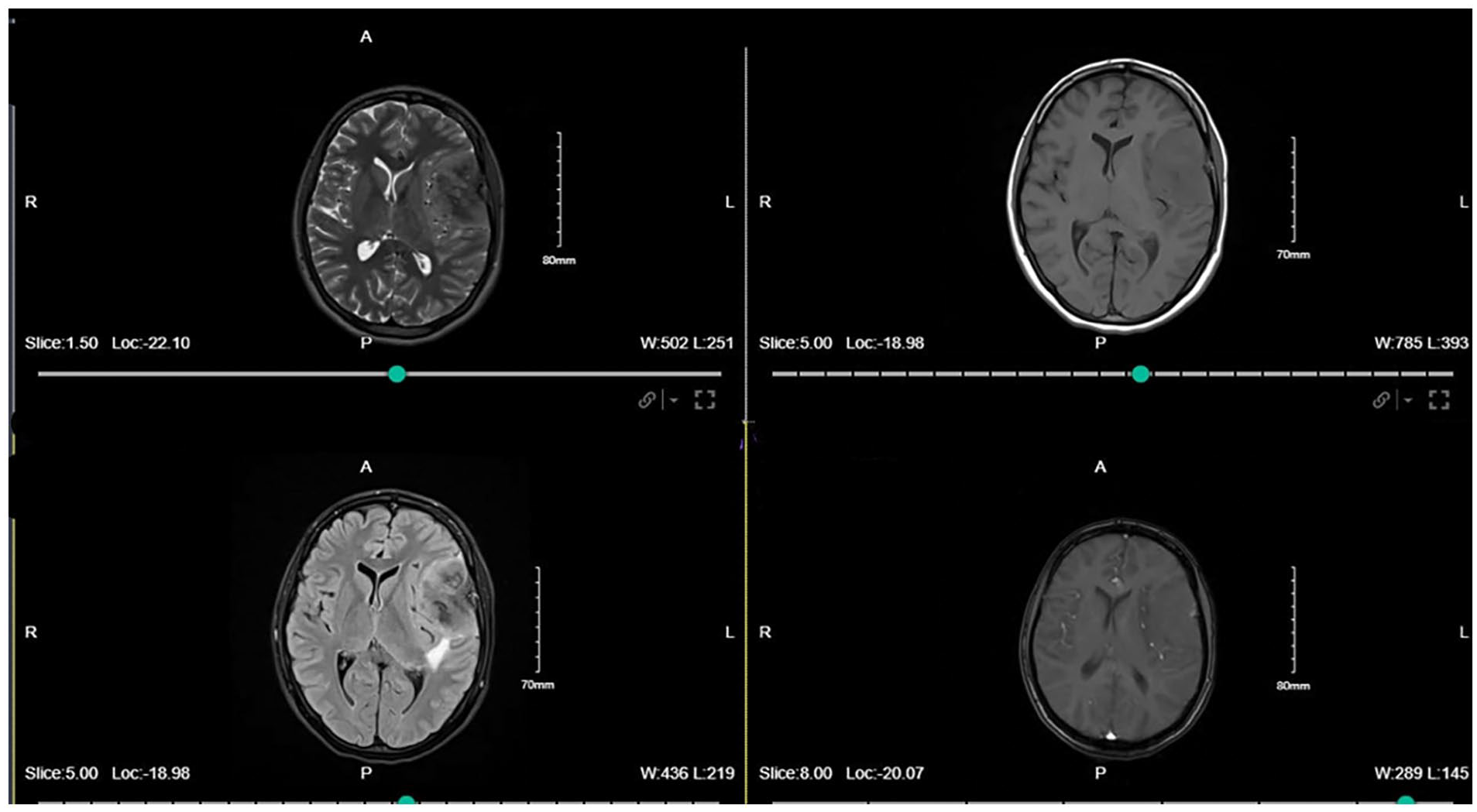
Preoperative magnetic resonance imaging scan showing 5.3 × 3.2 cm extra-axial dural-based mass overlying the left frontal and temporal lobes with moderate associated mass effect.
Immediate management involved commencing the patient on Dexamethasone and Levetiracetam and she was admitted for observation. A multidisciplinary team meeting was arranged. This meeting involved the neurosurgical team, an obstetric anaesthesiologist, an obstetrician and a neonatologist. The risk of developing worsening intracranial hypertension or tumour associated complications was deemed to be high in the context of the size and position of the tumour. Though consideration was given to delaying intervention until after 34 weeks to improve fetal maturity, the additional possibility for hormone mediated accelerated tumour growth informed the decision to proceed with immediate surgical resection.
The patient remained a part of the decision-making process and was counselled on the rationale for intervention, and the associated risks to the patient and her foetus. A preoperative anaesthetic assessment identified no risk of difficult airway, and she was given an American Society of Anaesthesiologists (ASA) classification of III. At 30 + 2 weeks gestation, she underwent left craniotomy and resection of left frontotemporal World Health Organization grade 2 meningioma. Preoperatively, an ultrasound confirmed fetal viability and 30 millilitres (mls) of oral sodium citrate was administered to the patient. Large bore intravenous access was secured in addition to a right internal jugular central venous catheter. Invasive arterial blood pressure monitoring was established. A modified rapid sequence technique using fentanyl 2 micrograms/kilogram (mcg/kg), propofol 2 milligrams/kg (mg/kg) and rocuronium 1 mg/kg was used to rapidly secure the airway with a size 7.0 reinforced endotracheal tube whilst avoiding hypertension associated with laryngoscopy.
The patient was positioned supine with her head secured in Mayfield pins. Left uterine displacement was ensured at all times. Anaesthesia was maintained with Sevoflurane at Minimal Alveolar Concentration of 1 in a 50% oxygen/air mixture combined with an intravenous Remifentanil target-controlled infusion of 1–3 nanograms/ml (ng/ml). Noradrenaline IV infusion was titrated to achieve a target mean arterial pressure (MAP) >75 millimetres of mercury (mmHg). End-tidal carbon dioxide was maintained between 4.6 and 4.8 kilopascals (kPa). Two hours into the resection, 100 ml of sodium chloride 3% was administered to reduce brain swelling, raising the plasma sodium level from 131 to 136 millimole/litre (mmol/L). The surgery lasted 5 h and the estimated blood loss was 400 ml. The patient’s neuromuscular blockade was reversed with neostigmine and glycopyrrolate and not Sugammadex because of concerns relating to progesterone binding of Sugammadex in pregnancy. 3 Postoperatively, the obstetric team reconfirmed the viability of the foetus with ultrasound and her postoperative neurological examination was unremarkable. She was transferred to the intensive care unit for further monitoring. MRI brain on postoperative day three showed complete tumour resection (Figure 2).

Postoperative MRI scan showing a large resection cavity in the left frontal lobe, no definite tumour.
The patient was discharged home 7 days postoperatively on Levetiracetam 750 mg twice daily. She subsequently underwent caesarean section delivery at full term under subarachnoid block with the delivery of a healthy baby girl. At a 3 month follow-up review both the patient and her baby remained well.
Discussion
The timing of surgical intervention may be challenging where there is no immediate threat to life as in this case report where the patient’s neurosurgical status had returned to normal and medical management had been initiated. In the second half of pregnancy, the differential for tonic-clonic seizures is large. Of the neurological causes, important causes to consider are epilepsy, eclampsia, intracranial infection, trauma, cerebral-venous sinus thrombosis, intracranial malignancy, as well as rarer causes such as posterior reversible encephalopathy syndrome associated with HELLP syndrome. 4 The tumour size and its potential for growth, and the fetal gestational age need to be considered. A major factor in the decision to intervene in this patient related to the concern for rapid neurological deterioration due to hormone mediated accelerated meningioma growth.
The rarity of meningiomas in pregnancy makes decision making regarding the timing of surgical intervention difficult. Carbone et al. noted that of 88 reported cases most patients were deemed suitable for elective meningioma resection, and it was the presence of visual symptoms and an early pregnancy diagnosis of meningioma that was associated with urgent surgery during pregnancy. 5 Laviv et al. propose a pathway for determining timing of surgical intervention based on gestational age and visual loss. 6 Additionally, Priddy et al. developed an algorithm based on a patient case series beginning with an evaluation of the urgency of neurological symptoms. If the patient is clinically stable, gestational age and obstetric risks to the patient are to be considered. 7 In our case, we used the risk of hormone mediated growth as a justification for urgent intervention. Our concern with the potential for deterioration secondary to raised intracranial pressure aligns with the trend of urgent surgical intervention in those with visual symptoms. 5 Ultimately, the rarity of such cases means accurately stratifying patients according to risk of surgery during pregnancy versus delaying till the after pregnancy is not feasible and decisions should be made on a case-by-case basis with involvement of multi-disciplinary team. 5
The literature on the incidence of meningioma in pregnancy and the effects of hormone-mediated growth is conflicting. 8 Epidemiological studies clearly point to a female preponderance for tumour development with two-thirds of tumours occurring in women, and many case reports identify pregnancy as a risk factor.8,9 This is supported by evidence that meningiomas contain receptors for progesterone and that progesterone has shown to increase the mitogenic stimulus of the tumour. 10
However, studies attempting to better identify the exact mechanism of tumour growth in the presence of sex hormones are difficult because of the broad effects of oestrogen and progesterone. A recent population-based cohort study detected a lower rate of meningiomas in pregnant patients compared with the normal population and made the argument for the possibility of a protective effect of pregnancy against meningiomas. 8 It is likely however that of those meningiomas that present in pregnancy, they represent a rarer biologically distinguishable subgroup of hormone-dependent meningiomas. A subgroup of meningiomas have been found to have a causal relationship with progestin cyproterone acetate – a synthetic progesterone derivative. 11 Observations overall are now trending towards the presence of a group of meningioma that demonstrate hormone dependent growth and increase in size in pregnancy.
There are also vascular mechanisms described for meningioma growth in pregnancy. The alterations in tissue permeability and fluid distribution in pregnancy may increase peritumoral oedema. Additionally, pathological examinations of meningiomas in pregnancy display increased vascularity compared with non-pregnant women. The possibility of an underlying hormonal link to the vascular alterations in gestational meningioma has yet to be identified. 8
Both uteroplacental circulation to foetus and maternal cerebral perfusion/optimal surgical conditions must be optimally managed intraoperatively. In general, physiological conditions required to optimise both are aligned. Ensuring euvolaemia, normoxia, normal pH and normothermia optimises both systems. The uteroplacental unit is almost totally reliant on MAP for adequate blood flow. The target MAP of 75 mmHg ensures adequate cerebral and uteroplacental perfusion. Mild to moderate hypocapnoea is often indicated to relax the brain in the context of raised intracranial pressure; however, hypocapnoea can lead to uteroplacental vasoconstriction and will cause a leftward shift of the oxyhaemoglobin dissociation curve, both of which will impair fetal oxygen delivery. If hypocapnoea is required to facilitate urgent reduction in intracranial pressures, then it should be limited in duration and combined with fetal monitoring where possible. 12
Conclusion
Intracranial malignancies may present as medical emergencies requiring urgent neurosurgical intervention in pregnancy. There are no guidelines to assist in their management, and timing of surgical intervention remains a significant challenge. A multidisciplinary approach is necessary in such cases. Hormone-mediated tumour growth must be taken into account when deciding in timing of surgical intervention. When surgery is indicated, both maintenance of uteroplacental circulation and optimal intracranial conditions should be targeted to ensure optimal outcome for both mother and foetus.
Footnotes
Acknowledgements
None.
Authors’ note
Dr. Oscar Duffy is listed first as he performed the literature review, edited the case report, wrote the discussion, and is the overall corresponding author. The remaining authors are listed alphabetically by last name after their contribution category.
Author contributions
M.S., O.D. contributed to conceptualization; M.S. contributed to investigation; O.D. contributed to methodology; M.S. contributed to writing – original draft; O.D., T.D., T.O’N. contributed to writing – review & editing; T.D., C.M., T.O’N. contributed to supervision; C.M. contributed to resources; M.S. contributed to patient consent.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for publication of this article recieved from Royal College of Surgeons Ireland.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Guarantor
Oscar Duffy.
Trial registration
Not applicable.