
Abstract
Objectives:
Glucocorticoid steroids are frequently prescribed, and side effects are well-known, such as glucocorticoid-induced osteoporosis. Our aim was to estimate the nationwide trend in the prevalence of glucocorticoid steroid prescriptions over 17 years and to elucidate the proportion of patients on long-term glucocorticoid steroid therapy who receive active bone protective therapy. As well as to examine which medical specialties prescribe glucocorticoid steroids the most.
Methods:
This study was a retrospective observational registry study extended over 17 years (2003–2020). Data were retrieved from the Icelandic Prescription Medicine Register on all delivered glucocorticoid steroids (Anatomic therapeutic chemical code: H02AB) for oral use. Long-term users were defined as those who annually received ⩾90 defined daily doses of glucocorticoid steroids.
Results:
Annually, 3.8% of the population received oral glucocorticoid steroids, from 3.3% in 2006 to 4.3% in 2017. Prednisolone was most frequently prescribed. Females dispatched glucocorticoid steroid prescriptions more often than males (55.8%). Males and females reached their peak prevalence between the ages of 60 and 70. General practitioners most often prescribe glucocorticoid steroids, followed by physicians in training, rheumatologists, internists, and medical students. Of those who received prescriptions for glucocorticoid steroids, 12.2%–18.1% were classified as long-term users. A declining number of patients have been receiving bone-protective therapy in recent years. Only 13.0% of chronic users received bone protective therapy in 2020.
Conclusion:
The use of glucocorticoid steroids has increased during the last 2 decades despite improvements in treatment for inflammatory disorders. The prevalence of long-term users has remained stable. Meanwhile, the use of parallel active bone-protective therapy among long-term users of glucocorticoid steroids is declining. Thus, improvements in prophylaxis for corticosteroid-induced osteoporosis are urgently needed for patients who require long-term treatment with glucocorticoid steroids.
Introduction
Oral glucocorticoid steroids (GCS) are frequently used for their anti-inflammatory and immunosuppressive qualities. They are a cornerstone in treating several acute and chronic inflammatory and autoimmune disorders and are used to reduce clinical symptoms and modify underlying disease activity.1,2 Therefore, GCS are prescribed by a broad spectrum of medical specialists, particularly general practitioners and internists.3–5
The skeletal effects of GCS are well known.6–8 Bone fractures remain the most serious adverse event of chronic GCS use. 7 Continuous oral GCS therapy has been associated with loss of bone mass and an increased risk of fragility bone fractures, especially vertebral fractures.6–8 The fracture risk is dose-dependent and is seen quickly following the initiation of the therapy, already within 3 months, which leads to an imminent risk of fracture.3,6–13 Clinical recommendations in Iceland from 2002 regarding osteoporosis and glucocorticoid use state that all patients that need long-term treatment with glucocorticoids (7.5 mg or more of prednisolone) should receive full prevention for osteoporosis and that those receiving >15 mg prednisolone (or equivalent dose) are at the most risk and should receive bone protective treatment from the initiation of glucocorticoid therapy. 14 Several national medical organizations have more recently, advocated for risk stratification for fragility fractures or the use of antiresorptive or bone-forming agents to prevent glucocorticoid-induced osteoporosis (GIOP) in individuals taking GCS regularly, even if it is only for a few months, for example, 3–6 months.15,16 Prevention of GIOP should start as soon as GCS treatment is initiated since bone loss is most rapid in the first months of therapy. 17 Oral bisphosphonates are considered first-line therapy due to their well-proven effectiveness in preventing osteoporosis-related fractures, safety, and the low cost of this regimen.3,18 Despite this, studies still demonstrate that a minority of patients receiving long-term GCS treatment receive bisphosphonates as a preventative measure for GIOP.2,4,5,19
Studies focusing on the prevalence and duration of GCS treatment illustrate significant differences in GCS use between countries. The variation in the prevalence of glucocorticoid prescriptions ranges from 0.5% to 21.1%.1,2,4,12,20–22 Studies that examine short-term usages of GCS have shown the prevalence to vary from, for example, 3% in Denmark, 21 14.7%–17.1% in France 2 and 14.1% in Western Sweden, 1 meanwhile, in the US the ranges extend from 1.2% to as high as 21.1%.5,12 When specifically examining long-term use of GCS, studies have shown similar numbers of prevalence, or 0.5%–0.75% in the UK,4,20 0.7% in France 2 , and 0.5% in Western Sweden. 1 However, these studies had diverse definitions of chronic/long-term usage of GCS. Therefore, their results are not entirely comparable.1,2,4,20
Few studies have examined nationwide both the prevalence and trends of GCS use and the management of GIOP. A previous study from 2002 in East Iceland found that only 9% of chronic GCS users received primary prevention for GIOP. 19 In another study from the US (2013), it was reported that of the users who used oral GCS for longer than 90 days, only 8.6% received bisphosphonates, 22.7% calcium, and 18.5% vitamin D. 5 A more recent study from 2017 by Bénard-Laribière et al. 2 showed that 55% of patients on GCS therapy in France who were defined as having an increased risk of osteoporotic fracture received calcium and/or D-vitamin supplements. However, only 27.4% received bisphosphonates, and 5.0% received another bone-protective drug.
This study aimed to describe the trend of GCS prescriptions nationwide over 17 years, specifically oral GCS use. Furthermore, we examined the prevalence of parallel prescriptions of bone protective drugs against GIOP among chronic users of GCS (patients receiving ⩾90 defined daily doses (DDD) of GCS over 12-month period). We also aimed to gain a glimpse into the reason for prescribing GCS by investigating which medical specialities had the highest prescription rates of GCS.
Materials and methods
Study design and data
The present study was a retrospective observational study extended over 17 years (2003–2020). Data were retrieved from the Icelandic Prescription Medicines Register (IPMR), operated by the Icelandic Director of Health. 23 The register covers 98% of all dispatched drug prescriptions delivered by pharmacies in Iceland in the end of the study period. The drugs studied in the present study, that is, both GCS and bone protective agents, are delivered only on prescriptions and are highly reimbursed, according to the Icelandic Health insurance system. 24
IPMR represents all prescriptions made and dispatched in Iceland since the year 2002. 23 Iceland has a population of 364.134, as recorded on 31st December 2020. 25 Information on prescriptions; the name of the medication, number of dispatched prescriptions, DDD, gender and prescription date were retrieved from the register using Anatomical Therapeutic Chemical (ATC) codes. All ATCs that represented GCS (H02AB) were included in the data set. For the analysis of oral GCS use, steroids for soft tissue- and joint injections were excluded. ATC codes, including the following bone-protective therapy; bisphosphonates (M05BA) (more specifically M05BA03 Pamidronic acid, M05BA04 Alendronic acid, M05BA06 Ibandronic acid, M05BA08 zolendronic acid), denosumab (M05BX04) and teriparatide (H05AA02), were included in our dataset from the IPMR. Other specific bone protective drugs were not marketed in Iceland during the study period. In addition, we collected data on the age and sex of those who received the medicine and the medical speciality to which the prescribing physician belongs. The dataset was complete, wherefore, no imputation was required.
It is possible to receive selected pre-defined data from the IPMR with prior approval from the National Bioethics Committee and Data Protective Authorities without informed consent from the individual patient as this is an epidemiological study, and no personal identification numbers were delivered to the researchers.
We identified all adult individuals who dispensed a prescription of GCS between 2003 and 2020 in Iceland. All individuals who dispensed a prescription in that period were included in the study and there were no exclusions. We furthermore identified all bisphosphonate prescriptions during the study period and looked especially at prescriptions for those individuals who were defined as chronic users of GCS.
The Strengthening the Reporting of Observational Studies in Epidemiology guidelines were used when preparing the study design. 26
Statistical analysis
Age was defined as the age at first GCS-dispensed prescription. Overall and age- and gender-specific prevalence over the study period were calculated using population data from Statistics Iceland. 25 Population sizes each year were used as a denominator. Data are presented in descriptive statistics.
According to the World Health Organization (WHO) definition, DDD was calculated as 1.5 mg dexamethasone, 30 mg hydrocortisone, 10 mg prednisolone, and 10 mg prednisone corresponding to one DDD. 27 The WHO definition for total DDD delivered for bone protective medicine was also retrieved. International classification criteria for long-term users of GCS are missing. Over the study period, the term “chronic use” has been used for various doses of GCS. At the beginning of the century, the equivalents of ⩾10 mg prednisolone were considered chronic use, but in recent years, 7.5 mg for a 3-month period has been used, and some studies have shown bone mineral density loss and increased fracture risk in doses of 5 mg for 3 months.28,29 To examine those who truly received chronic doses over the study period and should, therefore, qualify for active bone protective therapy, we defined long-term users as those who annually received ⩾90 DDD of GCS in 12-month as that reflects around 10 mg per day for 3 months over 12 months. We furthermore used this definition since pharmacies in Iceland cannot dispatch more than 100 days of a prescribed dose. 30 We also defined active bone protective therapy if the individual receiving a prescription for a bone protective medication within 90 days of filling up their GCS prescription.
Statistical significance was evaluated using Pearson’s chi-squared test. All analysis for statistical significance evaluated the difference between the first and last year of the study period.
All analyses were performed using Microsoft Excel (version 16.43; Microsoft Corporation) and R Studio (version 1.1.419; R Project for Statistical Computing).
Ethics
The study was approved by the Icelandic National Bioethics Committee and The Icelandic Data Protective Authorities (VSNb2021020055/03.0l.) A research grant from Landspitali University Hospital supported HH Bjornsdottir’s work. No other funds were provided for the study. B. Gudbjornsson has received consulting fees from Novartis unrelated to this study. Other authors declare no conflicts of interest.
Results
Prevalence of the prescription of oral glucocorticoids
During the study period, 95,047 individuals (55.8% female) dispatched at least one prescription of oral GCS. Annually, between 9885 and 15,054 individuals received GCS from 3.3% of the population in 2006, with the highest portion in 2017 of 4.3% (Figure 1). The mean annual prevalence of all GCS delivered during the study period was 3.8%. There was a statistically significant increase in filled prescriptions over the study period (p < 0.001). Prednisolone was the most frequently prescribed. In the earlier years of the study period, it was followed by betamethasone, but dexamethasone became the second most prescribed in 2015 (Figure 1). The total annual prevalence of the prescription rates of prednisolone increased by 0.88 percentage points and dexamethasone by 0.16 percentage points. However, prescription rates of betamethasone decreased by 0.96 percentage points over 17 years. The changes in prescriptions of prednisolone, dexamethasone and betamethasone were all statistically significant between the first and last year with a p-value of <0.001.
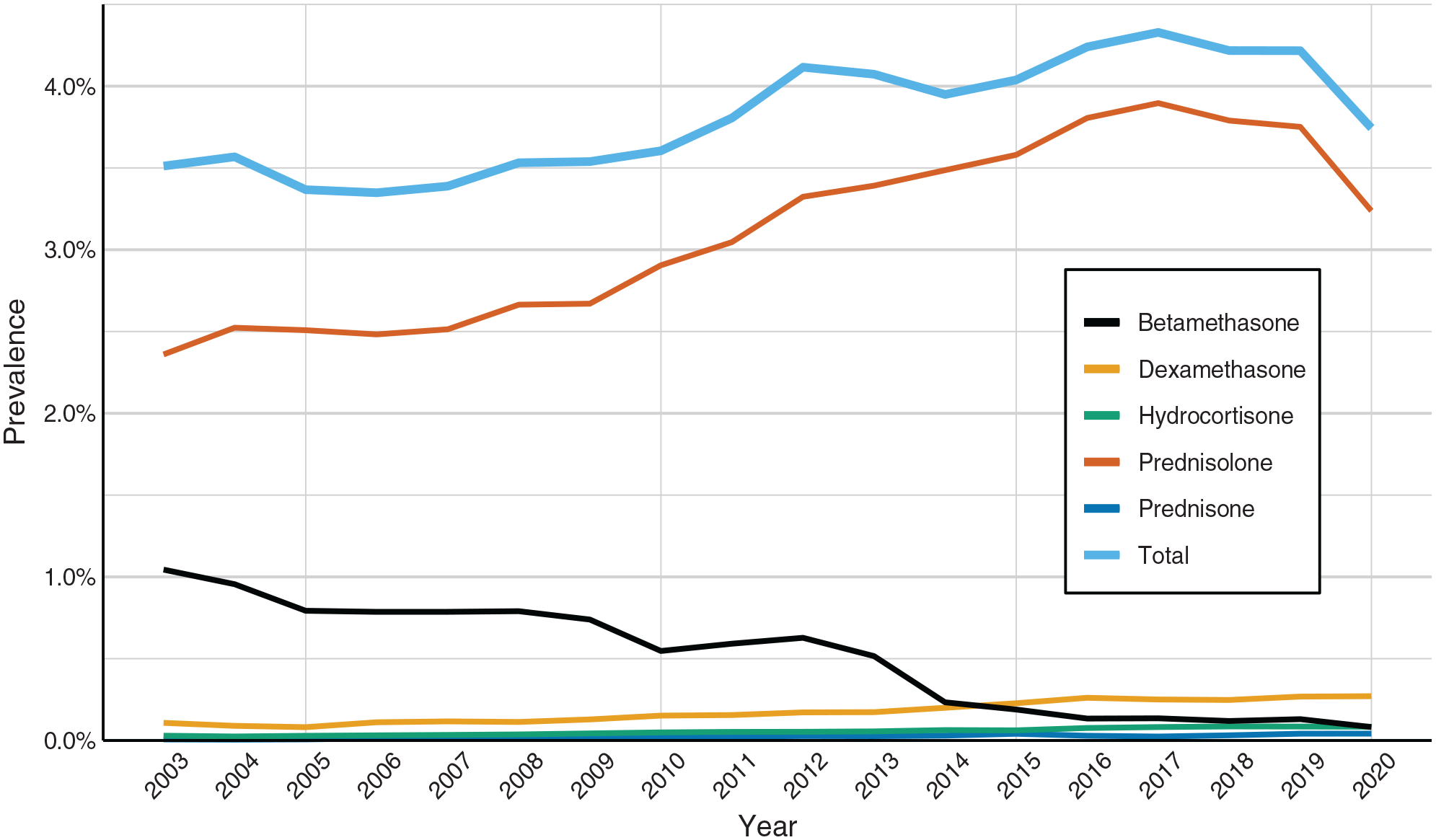
Annual prevalence of prescriptions of different GCS medications per year and the total prescription prevalence of all GCS in Iceland from 2003 to 2020.
The mean DDD prescribed per patient in each prescription was 72 DDD and remained stable during the study period.
Age and sex
Annually, females dispatched a majority of prescriptions of GCS compared to male individuals (58.2%–60.2% of dispatched prescriptions) (Figure 2). Males and females reached their peak prevalence between the ages of 60 and 70.
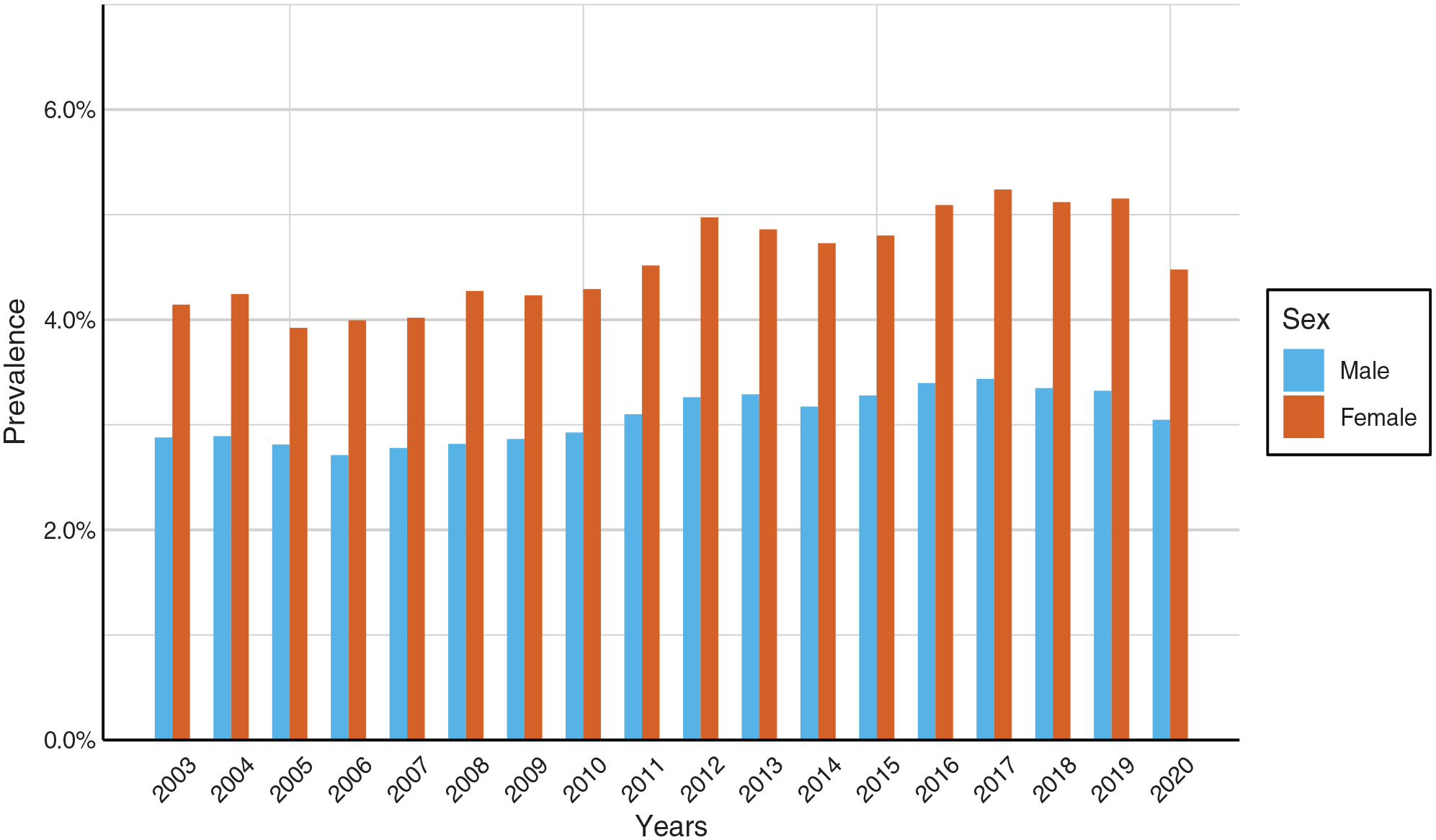
Prevalence of males and females receiving GCS prescriptions for oral use per year (2003–2020).
GCS prescription rates were stable for all age groups except for the two oldest groups. Although prescriptions increased for the 80–89-year-old group, the increase was not significant (p = 0.2943). The increase in the 90+ year-old group was statistically significant (p < 0.001) between the first and last year of the study period (Figure 3).
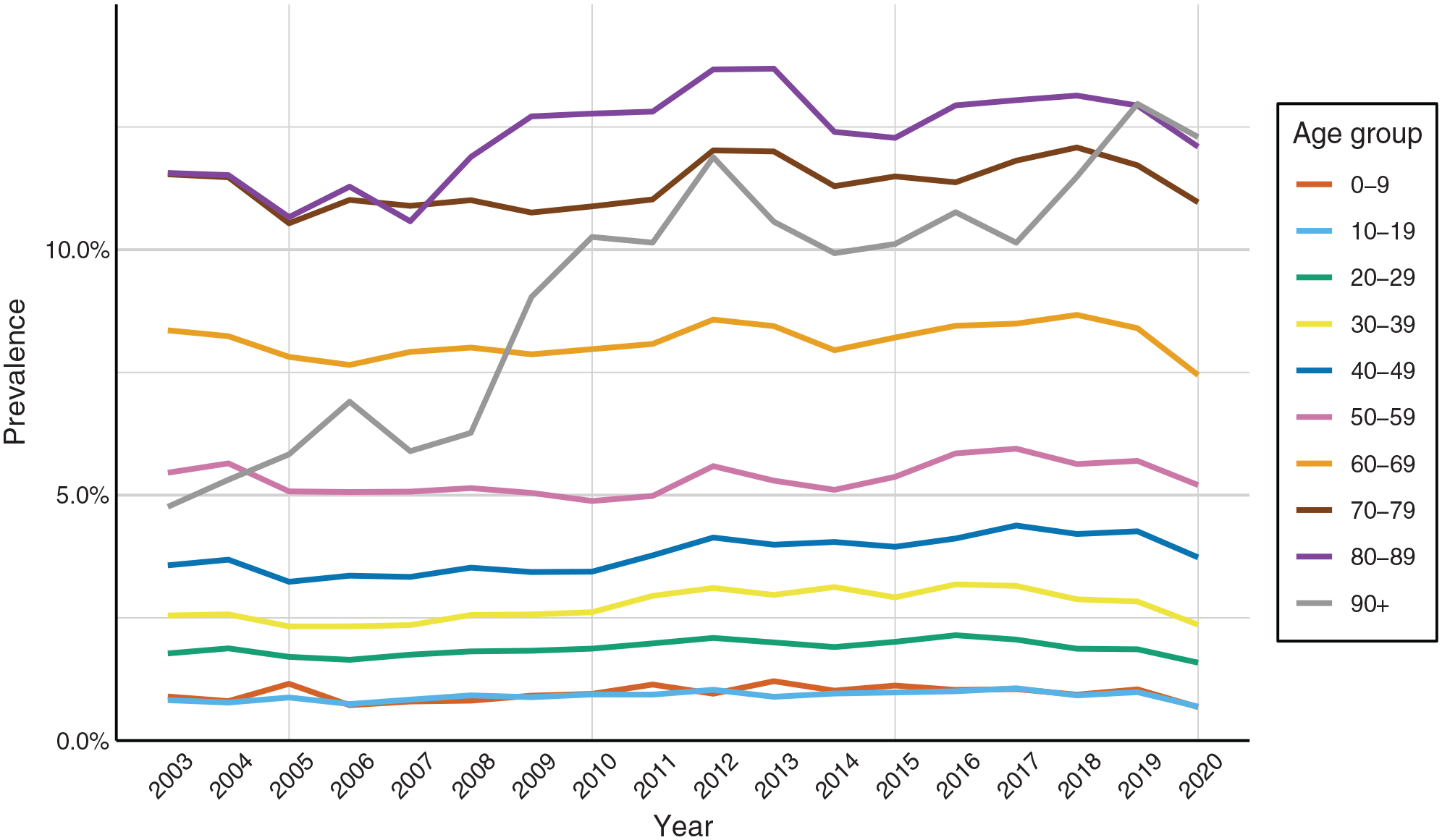
Prevalence of those who received oral GCS by age group from 2003 to 2020.
Long-term users of GCS and prevention
The percentage of GCS users that were defined as chronic users (>90 DDD/year) ranged from 12.2% to 18.1%, representing 0.5%–0.7% of the population at each time (Figure 4).

Prevalence of total users of oral GCS and prevalence of those that receive >90 DDDs of GCS each year.
Of the 1876 patients that received >90 DDD of GCS in 2020, only 244 received treatment with any bisphosphonate within 90 days of the prescription of GCS, representing 13.0% of patients receiving long-term GCS care, the lowest proportion of the study period. Between 2003 and 2020, this ranged from 13.0% in 2020 to 22.8% in 2006, but since 2011, the percentage of patients on long-term GCS therapy receiving active bone-protective therapy has steadily declined (Figure 5).

Percentage of those defined as chronic users that also receive bisphosphonates within 90 days of prescription of GCS, each year from 2003 to 2020.
Alendronic acid was the most commonly prescribed osteoporosis preventive medication during the entire study period, ibandronic acid was the second most prescribed. Teriparatide was the third most prescribed between 2003 and 2009 when it changed to pamidronic acid between the years 2009 and 2015, but after 2015, denosumab became the third most prescribed (Figure 6).

The total prescription prevalence of bone protective medications in Iceland over 17 years (2003–2020) and annual prevalence of different bone protective medications per year.
Medical specialities that prescribe oral glucocorticoids
During the study period, primary care physicians had the highest number of filled prescriptions (158,426), along with the highest DDD count (5,430,678). Physicians without a particular speciality (usually physicians in specialist training) had the second-highest prescription rates (82,057 prescriptions), and rheumatologists were the third (31,785). The following specialities followed in a number of prescriptions respectively: Internal medicine (22,300), medical students (21,641), pulmonology (21,109), immunology (18,495), geriatrics (17,912), oncology (17,398), and endocrinology (11,816). The 10 specialities with the highest prescription rates can be seen in Table 1. The full table is available in the Supplementary Material of this article.
The top 10 specialities that most frequently prescribed oral glucocorticoids.

The following medical specialities had the highest DDD count prescribed following general practitioners: Physicians in training (3,253,469), rheumatology (2,073,993), oncology (1,552,215), internal medicine (1,218,652), pulmonology (1,088,165), medical students (837,953), immunology (794,420), haematology (709,694), and endocrinology (671,149) (Table 1). For the chronic users of GCS, similar patterns were observed in prescriptions by specialty (data not shown).
We furthermore examined which medical specialities prescribed bisphosphonates for the group defined as chronic GCS users. The vast majority of prescriptions filled were prescribed by primary care physicians, physicians in specialist training, oncologists, and internists.
Discussion
In this population-based study, spanning nearly 2 decades, we examined the prevalence of GCS prescriptions and appropriate bone-protective therapy for long-term users of GCSs. We furthermore examined which medical specialities have the highest numbers of prescriptions and highest numbers of DDDs. We found in our nationwide study that the mean prevalence of GCS prescription was 3.8%, with the highest prevalence being 4.3% in 2017. The percentage of GCS users defined as chronic ranged from 12.2% to 18.1%, representing around 0.6% of the population each time. Prednisolone was the most frequently prescribed. GCS prescription rates remained stable in all age groups except for those over 80 years of age. A declining number of patients defined as chronic users received active bone-protective therapy, with only 13.0% of chronic users in 2020 receiving preventative therapy against GIOP within 90 days of filled GCS prescription. General practitioners had the highest number of GCS prescriptions and DDD count, followed by physicians in specialist training and rheumatologists.
The prevalence of overall prescriptions in Iceland aligns with other national studies focusing on this issue. Studies have had a varying prevalence of glucocorticoid prescriptions from 0.5% to 21.1% between countries.1,2,4,5,12,20–22 The prevalence of 3.8% in Iceland is therefore in the lower end of that spectrum. Studies examining the long-term use of GCSs have shown results of 0.5%-0.8%.1,2,4,20 Meanwhile, we found a prevalence of 0.5%–0.7%. However, these studies mentioned above have all had different definitions of chronic/long-term use (either duration of treatment or number of prescriptions while we used well-defined DDD, that is, >90 DDD over a 12-month period), making it difficult to compare these results.1,2,4,20
The overall prescription prevalence of GCS increased during the study period, which is remarkable and somewhat disappointing considering advances in general medical care. However, it was not in the scope of this study to analyse the impact of biologic anti-inflammatory drugs or steroid-sparing drugs such as azathioprine or methotrexate, which would have needed a different study design.
There is a limited number of studies that have examined the prevalence and trends of GCS use on a nationwide basis with regard to the management of GIOP. This is an important aspect of our study. The present study demonstrates that 13.0%–22.8% of long-term GCS users today receive bisphosphonate therapy in Iceland. Which demonstrates improvement compared to 2002. 19 A 2013 study from the US, 5 reported that of users who used oral GCS for longer than 90 days, only 8.6% received bisphosphonates and in 2017, Bénard-Laribière et al. 2 showed that of patients on GCS therapy in France defined as having a significantly increased risk of osteoporotic-related fracture, only 27.4% received bisphosphonates. In Iceland, we have a higher prescription rate of bone protective treatment than in the US but lower than in France.
Interestingly, the number of patients receiving active bone protective therapy and GCS has steadily declined for the last 6 years of the study. This may, in part, be related to the national bone-protective organization shifting from advocacy for bone-protective treatment to minimizing fall risk. During the study period, reimbursements of bisphosphonates changed, with the cheapest (alendronic acid) being the only one to be reimbursed as a first line treatment. Other drugs are available still as second- or third line drugs for treatment and/or prevention of osteoporosis after an application process to the National Health Insurance. This may, in part, have affected the change in prescriptions of these therapies nationwide over the last years of the study. Furthermore, studies on the side effects of bisphosphonates may have played a part in reduced usage. 31 In this study, we were only interested in parallel prescriptions of bone protective agents. It is likely that these patients on chronic treatment receive bone protective therapy later in life, for example, after a fragility fracture or diagnosed osteoporosis, However, in this study, we wanted to demonstrate the proportion that receives active prevention at the initiation of long-term GCS therapy. Therefore, there is quite some room for improvement in the prevention of GIOP.
As we do not have linkage data for underlying disease for GCS users, we aimed to gain a glimpse into the medical indication for prescribing GCS by examining which medical specialities most frequently prescribed GCS and which had the highest DDD count. We found that General practitioners and doctors in specialist training were behind the largest number of prescriptions, not surprisingly, followed by rheumatologists, general internists, immunologists, and pulmonologists. Interestingly, internal medicine doctors had the fourth-highest prescription rate and the fourth-highest DDD count but the ninth-highest number of individuals prescribed. This may reflect that these physicians primarily work in acute hospital settings and, therefore, frequently discharge patients from the hospital on high doses of GCS after a serious illness. The fact that primary care physicians have the greatest number of prescriptions and the highest DDD count reflects that they are both the first stop in the health care system and frequently renew patients’ prescriptions prescribed by other specialists or after specialist consultation. Physicians in training are in the second position, most likely for the same reason as family medicine doctors because of prescription renewals and because they usually write prescriptions on discharge from hospitals. Physicians in training are currently the largest group of doctors in the country, followed by family medicine specialists. Interestingly, the same trends were observed in prescription patterns for long-term GCS treatment patients.
The ability to access a major national database with information on all prescriptions in Icelandic pharmacies is an important strength of our study. However, we acknowledge that the study population does not provide a random sample of the global population. Furthermore, Icelanders have a high medical reimbursement for their medicinal use. Therefore, the reliability of IPMR is further strengthened. Our study extends almost 2 decades. Meanwhile previous studies extended over a maximum of 7 years.1,2,19
In the present study, we could not acquire diagnostic codes related to the GCS prescriptions. Therefore, further investigation into underlying medical conditions for GCS prescription is of interest, especially in long-term GCS users. Furthermore, the burden of adverse effects due to long-term use of GCS is also highly important. In this context, bone fractures and the prevalence of systematic risk evaluation for fragility fracture, for example, with the FRAX-tool30,32 and bone density measurements in this group of long-term users, is of further importance concerning GIOP.
Limitations
We did not provide information on calcium and vitamin D supplements associated with GCS use, as these are frequently sold over the counter in Iceland. Therefore, we believed data regarding these supplements would have been skewed, so we decided not to include information on these supplements in our study. We, therefore, cannot account for how many patients received these first-line osteoporosis preventative measures along with their GCS. Since this was a nationwide study, a power analysis was not performed.
Certain limitations of our study have already been highlighted, such as the fact that we did not have information about the underlying disease and, therefore, indications for GCS treatment. We, therefore, neither have information about comorbidities that might be contraindications for specific bone protective therapies, such as chronic kidney disease, which is a contraindication for bisphosphonates. However, in most cases, those individuals should have been able to receive another type of bone-protective medication, such as denosumab. Since the IPMR is a prescription register, we do not have information about drugs given in inpatient hospital wards. We do, however, have information about prescriptions made at discharge from hospital, and if patients receive their bone protective therapy in outpatient wards, they are prescribed the medication and bring it to the hospital themselves, and those prescriptions are therefore included in the register. Furthermore, we could not indicate which medical speciality the doctor initiating GCS therapy belonged to and which prescriptions were renewals.
Conclusion
The use of GCS has increased during the last 2 decades in Iceland despite advances in general medical care for various inflammatory disorders. The prevalence of long-term GCS users has remained stable while active bone-protective therapy is steadily declining despite national guidelines urging active measurements against GIOP. Glucocorticoid-induced osteoporosis, therefore, seems to be an underrecognized and undertreated medical problem. Thus, for the sake of those patients who require long-term treatment with GCS, there is a need to improve the prophylaxis for corticosteroid-induced osteoporosis. Further research on bone density measurements and fracture incidence in the GCS group compared to matched comparators is of importance.
Supplemental Material
sj-doc-2-smo-10.1177_20503121241235056 – Supplemental material for Nationwide prevalence of glucocorticoid prescriptions over 17 years and osteoporosis prevention among long-term users
Supplemental material, sj-doc-2-smo-10.1177_20503121241235056 for Nationwide prevalence of glucocorticoid prescriptions over 17 years and osteoporosis prevention among long-term users by Hulda Hrund Bjornsdottir, Ólafur Brynjólfur Einarsson, Gerdur Gröndal and Bjorn Gudbjornsson in SAGE Open Medicine
Supplemental Material
sj-docx-1-smo-10.1177_20503121241235056 – Supplemental material for Nationwide prevalence of glucocorticoid prescriptions over 17 years and osteoporosis prevention among long-term users
Supplemental material, sj-docx-1-smo-10.1177_20503121241235056 for Nationwide prevalence of glucocorticoid prescriptions over 17 years and osteoporosis prevention among long-term users by Hulda Hrund Bjornsdottir, Ólafur Brynjólfur Einarsson, Gerdur Gröndal and Bjorn Gudbjornsson in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank applied mathematician Jon Hlodver Fridriksson, MSc, for statistical advice and figure design.
Author’s note
Author contributions
All authors made substantial contributions to the design of the work, analysis, and interpretation of data. All were involved in writing the article and subsequent revisions. All authors have approved the version that is to be published. All authors assume public responsibility for the work.
Availability of data and materials
Due to privacy and ethical concerns, any raw data cannot be shared. Aggregated data from IPMR can be shared upon reasonable request and with appropriate ethics committee approvals.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B. Gudbjornsson has received consulting fees from Novartis unrelated to this study. Other authors declare no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HH Bjornsdottir’s work was supported by a research grant from Landspitali University Hospital.
Informed consent
Informed consent was not sought for the present study because it is possible to receive selected pre-defined data from the IPMR with prior approval from the National Bioethics Committee and Data Protective Authorities without informed consent from the individual patient as this is an epidemiological study, and no personal identification numbers were delivered to the researchers.
Consent for publication
Not applicable.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.