
Abstract
Objectives:
The use of inhaled corticosteroids is the standard maintenance therapy in asthma therapy and as adjunct therapy in moderate to severe chronic obstructive pulmonary disease. A dose-related increase in fracture risk is associated with inhaled corticosteroid use; there is an inverse relationship between bone mineral density and duration and cumulative dose of inhaled corticosteroid. Adequate intake of calcium and vitamin D are cornerstones of osteoporosis prevention. The objectives are to assess whether the proportion of patients receiving inhaled corticosteroids are taking calcium and vitamin D; the association between long-term inhaled corticosteroid use and abnormal bone mineral density or fractures; and how many qualified patients received bone mineral density scans.
Methods:
Patients who filled a prescription for inhaled corticosteroids at selected community pharmacies across Alberta were recruited for a survey of their osteoporosis prevention activities.
Results:
A total of 256 patients from 12 community pharmacies were included. The average age was 60 ± 17.4 years with 65% female. There were 21%, 51%, and 28% of patients on high, medium, and low dose inhaled corticosteroids, respectively. Only 17% of patients >50 years old received recommended calcium and vitamin D supplementation and 87 (73%) of the qualified patients received bone mineral density scan.
Conclusion:
Osteoporosis prevention in inhaled corticosteroid users is currently poorly addressed. More promotion is needed to raise pharmacist awareness of the risks of inhaled corticosteroids.
Keywords
Introduction
Inhaled corticosteroids (ICSs) are widely accepted for their potent anti-inflammatory effects in the lungs and low systemic activity. 1 The use of ICSs is the standard maintenance therapy in the management of asthma. 2 It is also widely used (though only recommended as an adjunct therapy) in patients with moderate to severe chronic obstructive pulmonary disease (COPD). 3 Moderate doses of ICSs are considered highly effective in controlling inflammatory symptoms with minimal serious side effects such as those associated with systemic absorption. 4
It is well recognized that oral corticosteroid therapy is a risk factor for osteoporosis. 5 Although ICS products are designed to deliver the drug particles to the lung, systemic side effects may result from the portion of administered corticosteroid that is systemically absorbed from the upper respiratory tract and through the lung vasculature during administration. Approximately 10% to 60% of ICS dose is delivered directly to the lung and the rest is partially systemically absorbed. The amount of drug delivered to the lung depends on both the choice of corticosteroid and the inhalation device. The remaining 40% to 90% of the drug may be deposited in the pharynx where it can be swallowed and ultimately become systemically available.6,7 Nevertheless, it has been shown that there is a dose-related increase in risk of fracture with high-dose ICS use.1,4,5,8–14 In addition, there is an inverse relationship between bone mineral density (BMD) and the cumulative dose and duration of ICS therapy in patients with asthma.5,14–17 A meta-analysis including observational studies in older patients with COPD and asthma found an increased fracture risk among patients who use high doses of ICS. 10
Corticosteroids-induced osteoporosis results from suppression of bone formation while bone resorption is promoted.11,16 Adrenal androgen suppression may also predispose post-menopausal women to bone loss in the presence of oral corticosteroids. 16 ICS-induced osteoporosis is increasingly important due to the fact that many patients who develop COPD are at an older age, both conditions being independent risk factors for osteoporosis. Also, these individuals may be receiving ICSs as part of their maintenance long-term therapy. Moderate or high doses of ICS are associated with increased risk for effects on the bones. 18 A recent study showed that long-term low-dose ICS use increases the rate of BMD loss in patients with COPD. 19 A meta-analysis of 21 randomized control trials showed that vitamin D plus calcium is more effective than no therapy or calcium alone in preventing decreases in lumbar spine BMD in oral corticosteroid-induced osteoporosis. 20 Wong et al. 5 recommend that patients who require high dose of ICS for long term should consider receiving osteoporosis prophylaxis. Supplements of calcium and vitamin D have been shown to prevent corticosteroid-induced osteoporosis effectively.4,22 The Canadian Osteoporosis guidelines recommends that patients >50 years old should consume calcium 1200 mg and vitamin D 800–2000 IU per day.21,23 Also, patients ⩾65 years old should receive an annual BMD. 21
Recent studies conducted in general practice showed that physicians do not use prophylaxis or treatment in patients receiving ICS with or without risk factors for osteoporosis in the community setting.24,25
Objectives
The primary objective of our study is to investigate whether patients with asthma and /or COPD treated with ICS are taking calcium and vitamin D supplements in the community setting. The secondary objectives are to (1) assess the number of patients receiving long-term ICS treatment that had an abnormal BMD scan or fractures on any ICS dose (long-term treatment defined as ⩾4 years); and (2) determine many patients who were qualified to receive an annual BMD scan actually received one. After an exhaustive literature search, we were unable to find any study that assessed prevention and monitoring of osteoporosis in ICS users.
Setting
The study was conducted in community pharmacies in Alberta, Canada.
Method
The University of Alberta Health Research Ethics Board approved the study.
All patients who filled a prescription for an ICS at 12 selected community pharmacies in Alberta were screened for the study. Since the Health Information Act of Alberta only permits access to patient information by custodians of the clinical records or their delegates, community pharmacies were included in the study if a pharmacy student are employed as a student pharmacist. The student pharmacists approached all patients receiving a prescription for ICS if they met the inclusion criteria. After receiving written or verbal patient consent, the student pharmacist then administered the questionnaire, which included patient demographics, ICS dose, indication for use, duration of use, and any osteoporosis prophylaxis or treatment. Risk factors for osteoporosis such as comorbidities, smoking, alcohol consumption, height, weight, self-reported history of fragility fracture, and lack of exercise were also assessed. Self-reported BMD scan history was also recorded. The questionnaire was conducted either in person or over the phone.
Inclusion criteria. Patients 19 years or older who have been using ICS for a period of 3 consecutive months or longer in the past 12 months were included in the study.
Exclusion criteria. Patients who had difficulty speaking English or who had medications given by a caregiver (proxy for cognitively impaired) were excluded.
Since there is no available study on the topic to determine a sample size, we had to make certain assumptions based on the Nielsen et al. 24 study. Each pharmacy has an estimate of about 100 patients on ICS. Assuming that 75% of patients are not taking vitamin D and calcium supplement, with a significance level set at 0.05, the estimated sample size is 290.
Statistical analysis
Data were analyzed in SPSS version 22. String variables were recoded into binary numerical variables reflecting their original variables. Multivariate analysis was used to determine statistical difference (p < 0.05) between the patients receiving long-term (⩾4 years) and short-term ICS and the association of bone loss or self-reported fragility fracture.
Results
A total of 256 patients were recruited from 12 different community pharmacies across Alberta from April 2012 to May 2013. Over 90% of patients approached by the student pharmacists agreed to participate in the study. The overall average age of patients was 60 ± 17.4 years with 65% females. The demographic distribution of the patients is presented in Table 1. The patient age ranged from 23 to 95 years (Figure 1).
Demographics.
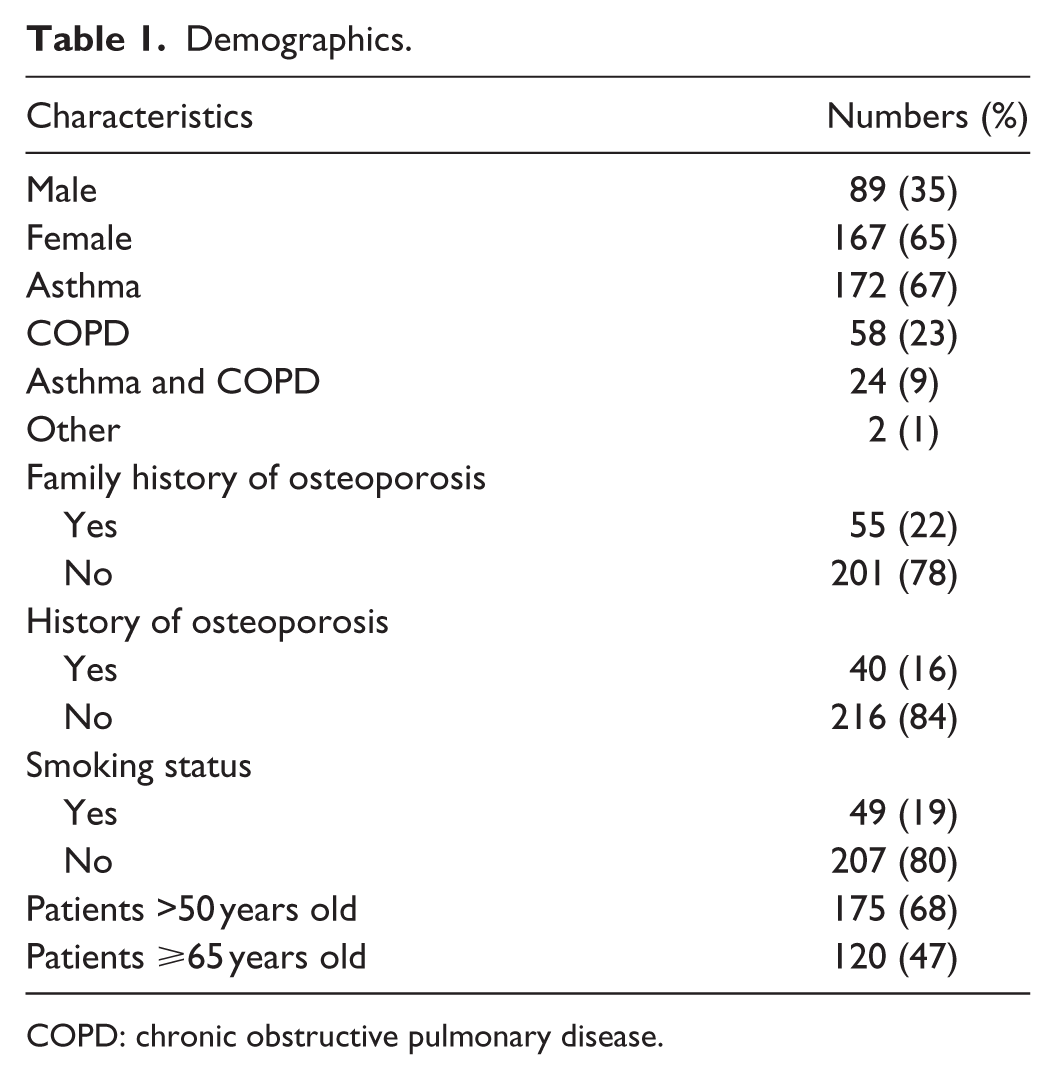
COPD: chronic obstructive pulmonary disease.

Age–sex distribution. This figure shows the distribution of genders of the participation in each age group.
The classifications of high-, medium-, and low-dose ICS are based on the equipotent daily dose for each ICS according to the Global Initiative for Asthma (Table 2). 2 There were 60 (23%), 133 (52%), and 63 (24%) of the patients using high-, medium-, and low-dose ICS, respectively. A total of 173 (68%) and 192 (75%) of ICS users were taking calcium and/or vitamin D supplementation, respectively. Out of 175 patients >50 years old, only 2 (2%), 7 (8%), and 3 (7%) of the patients were taking recommended calcium supplementation of ⩾1200 mg a day; 27 (60%), 56 (64%), and 22 (51%) of the patients were taking recommended vitamin D supplementation between 800 and 2000 IU for high-, medium-, and low-dose ICS, respectively. Only 4 (9%), 19 (22%), and 30 (17%) of patients >50 years old met both the recommended daily intake of calcium (=1200 mg) and vitamin D (800 and 2000 IU) supplementation.
Estimated dose equivalencies for inhaled corticosteroids for adults. 2

pMDI: pressurized metered-dose inhaler; DPI: dry powder inhaler.
There were 165 patients on long-term (⩾4 years) ICS of whom 38 (23%) and 21 (13%) had abnormal BMD and self-reported fragility fractures, respectively (Table 3). There was no statistical significance in the high-dose and medium-dose group with respect to bone loss or fractures.
Duration of ICS and abnormal bone mineral density or fractures.

ICS: inhaled corticosteroid; BMD: bone mineral density.
Patients who had bone loss on BMD scan had a high risk of fracture with the odds ratio of 1.37.
Calcium and vitamin D supplementation
Although the doses vary extensively, overall a total of 173 (68%) and 192 (75%) of ICS users were taking calcium and/or vitamin D supplementation, respectively. Tables 4 and 5 summarize patient calcium and vitamin D daily intake. Out of 175 patients >50 years old, only 2 (2%), 7 (8%), and 3 (7%) of the patients were taking recommended calcium supplementation of 1200 mg a day; 27 (60%), 56 (64%), and 22 (51%) of the patients were taking recommended vitamin D supplementation between 800 and 2000 IU for high-, medium-, and low-dose ICS, respectively (Table 6). Only 4 (9%), 19 (22%), and 30 (17%) of patients >50 years old met both the recommended daily intake of calcium (⩾1200 mg) and vitamin D (800 and 2000 IU) supplementation. Patients were more than twice as likely to meet vitamin D supplementation requirements set by Health Canada and the Canadian osteoporosis guidelines than calcium supplementation requirements regardless of ICS dose.
Self-reported daily calcium intake.

ICS: inhaled corticosteroid.
Self-reported daily vitamin D intake.
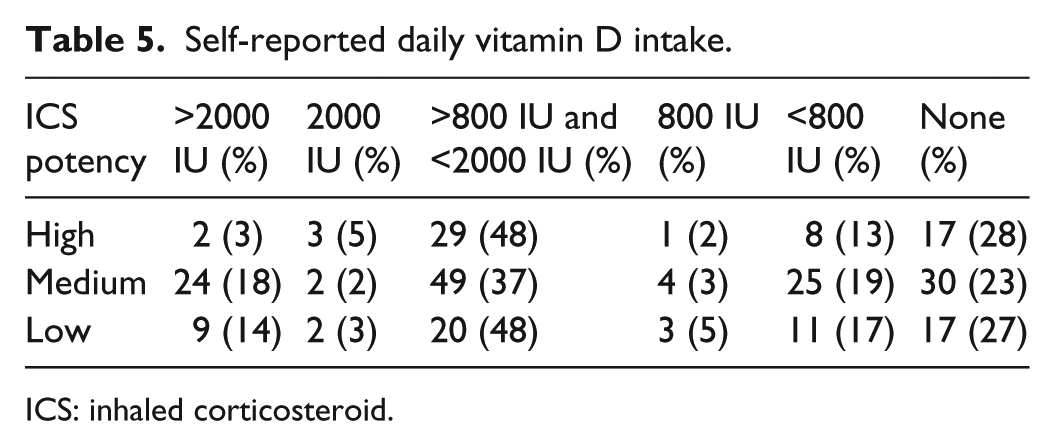
ICS: inhaled corticosteroid.
Self-reported daily calcium or vitamin D intake for patients >50 years old.

ICS: inhaled corticosteroid.
BMD scan
In terms of BMD scan, 87 (73%) of patients ⩾65 years old received an annual scan as recommended (Table 7).
Bone mineral density of ⩾65 years old.

ICS: inhaled corticosteroid; BMD: bone mineral density.
Discussion
ICSs are intended to exert their effects locally in the bronchial airway. However, studies show that ICSs are systemically absorbed and cause cortisol suppression. 26 Similar to Mathioudakis et al., 19 our study suggests that long-term low-dose ICS use could possibly lead to bone loss and fracture. We failed to show statistical significance. We were not able to detect a difference in the high-dose groups possibly because only 29% of the patients received a BMD scan. It is unclear why there is no difference in the medium-dose groups even though more than 50% of the patients received a BMD scan.
This is the first study of its kind to report clinically important research in osteoporosis prevention in ICS users in community pharmacies. In our study, only 30 (17%) of patients >50 years old received recommended intake of both calcium and vitamin D supplementation. Although most patients were able to report the amount of vitamin D and calcium consumed through dietary sources, patient recall may not be reliable. Therefore, it was unclear whether some patients may have adequate dietary calcium and vitamin D consumption and possibly did not require additional supplementation.
More patients were taking adequate doses of vitamin D supplementation than calcium. Tablet size and possible side effects such as constipation may have affected adherence to calcium. In addition, there is concern with cardiovascular adverse events related to high-dose calcium. Meta-analyses evaluated supplemental calcium and vitamin D and their effects on reduction in fractures and bone loss.18,27,28 In addition, recently, there has been a debate among many practitioners whether calcium is associated with cardiovascular disease. A meta-analysis has shown that calcium supplementation of ⩾1000 mg a day has <1% risk of myocardial infarction.29,30
Study limitations
Because of the strict Health Information Act of Alberta, the study encountered challenges. To conduct this study in a pharmacy, the student pharmacists must be an employee of that pharmacy to access patient information as a surrogate custodian of the patient’s health data. As a result, the selection of pharmacies in our study may not represent all pharmacies in Alberta.
A possible limitation of the study is the subjective patient reporting of dietary intake of calcium and vitamin D. Another limitation is that the BMD scans were patient reported and only pharmacy students with access to the electronic health records (Netcare®) were able to verify the information for BMD scans. Subsequently, not all BMD scan reports were consistently confirmed from health records. Although the estimated sample size was 290 patients, we had to terminate the study after 256 patients as we were not able to recruit more patients even though we had pharmacy students recruiting patients from 12 different pharmacies.
Conclusion
Osteoporosis prevention in ICS users is poorly addressed. Most patients over 50 years old treated with ICS are not receiving an appropriate total dose of calcium and vitamin D for osteoporosis prevention. Almost 73% of patients ⩾65 years old received a BMD scan. Future study with a large sample size and including objective measures of bone loss (BMD) and radiographic vertebral or skeletal fracture is needed to identify the risk of osteoporosis and prevent bone loss and fracture from long-term ICS use.
Footnotes
Acknowledgements
We would like to express our gratitude to the following pharmacy students and pharmacies for participating in the study:
Pharmacy students: Basel Alsaadi, Joey Ton, Jonathan Chung, Victoria Lam, Christopher Chen, Roxanne Smith, Zainab Abid, Sing-yue Lam, Sam Wang, and Carmen Ng.
Pharmacies:
Costco #544—Sherwood Park, Alberta. Shoppers Drug Mart #302—Edmonton, Alberta. Shoppers Drug Mart #312—Edmonton, Alberta. Shoppers Drug Mart #346—Edmonton, Alberta. Shoppers Drug Mart #386—Edmonton, Alberta. Shoppers Drug Mart #2301—Edmonton, Alberta. London Drugs #22—Edmonton, Alberta. Safeway Capilano—Edmonton, Alberta. Sprucewood Pharmacy—Lloydminster, Alberta. Walmart #3118—Edmonton, Alberta. Walmart #1570—Camrose, Alberta. Walmart #7236—Edmonton, Alberta.
Ken Cor, University of Alberta, Faculty of Pharmacy and Pharmaceutical Sciences.
Author contribution
V.C. recruited patients and wrote the first draft of the manuscript; A.J.C. contributed to protocol development and wrote the final draft of the manuscript; and H.L.B. conceptualized the research idea; developed the protocol and statistical analysis; and wrote the final draft of the manuscript and supervised Valerie Chan.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.