
Abstract
Background:
Exposure to splash of body fluids is one of the common ways of transmitting blood-borne infections from patients to healthcare practitioners. Globally, there is a paucity of evidence on exposure to splash of body fluids among hospital housekeepers. This study, therefore, investigated splash of body fluid and its predisposing factors among healthcare support staff in the Greater Accra region, Ghana.
Methods:
An analytic cross-sectional survey was conducted among support staff in 10 major hospitals between 30 January and 31 May 2023. A multi-stage sampling procedure was the overarching technique employed, and study participants were recruited through simple random and probability proportional-to-size sampling techniques. The data analyses were conducted using STATA 15 software. The preliminary association between exposure to splash of body fluids and predisposing factors was established through Chi-square, Fisher’s exact, and Mann–Whitney U tests. Log-binomial regression analyses were employed to validate the factors related to splash of body fluids at a significance level of p-value < 0.05.
Results:
The investigation was conducted among 149 healthcare support staff. The exposure to splash of body fluids over the past 1 year was 53.7% (95% CI: 45.3%–61.9%). The types of body fluids that were mostly encountered through these splash exposures were amniotic fluids (36.3%) and urine (23.8%). Several factors were found to be significantly associated with splash of body fluids, namely: employed as a healthcare assistant [APR = 1.61 (1.16, 2.22)], holding a supervisory position [APR = 0.24 (0.11, 0.51)], having a system in place for reporting body fluid splashes [APR = 0.61 (0.44, 0.85)], male healthcare support staff [APR = 0.62 (0.41, 0.93)], and adherence to standard precautions most of the time [APR = 1.66 (1.11, 2.48)].
Conclusion:
Healthcare support staff were highly exposed to splash of body fluids. Gender, supervisory role, category of worker, reporting systems, and adherence to standard precautions were associated with exposure to splash of body fluids. Facility managers are advised to enhance the efficiency of reporting systems.
Introduction
Healthcare workers, together with their support staff, are exposed through splash of blood and other body fluids that come into contact with their eyes, nose, mouth, or nonintact skin. Mucocutaneous exposure, as this type of exposure is referred to, accounts for 25.0% of all exposures at healthcare facilities, 1 and is one of the most effective ways of transmitting blood-borne infections from patients to healthcare practitioners.2–4 Further, it increases the risk of infection to hepatitis B, hepatitis C and human immunodeficiency virus (HIV) infections. As estimated by the World Health Organization, close to 3 million health workers are exposed to blood-borne pathogens every year. Also, due to occupational exposure to blood-borne pathogens, about 170,000, 2 million, and 0.9 million people are disease-ridden with HIV, HBV, and HCV infections, respectively. 5
Globally, many studies have reported on exposure to blood and body fluids among health workers, but few have specifically dealt with splash of blood and other body fluids. 6 Studies on exposure to splash of blood and body fluids have revealed that there is a high degree of splash of body fluids (SBFs) to an unavoidable extent in developing countries.7,8 Moreover, exposure through mucocutaneous injury is very significant in causing infections. 6 According to a recent systematic review and meta-analysis, a 12-month pooled global prevalence of splash exposures among health workers was reported as 56.6%, and 68.4% for Africa. 9 Also, a similar study conducted for Ethiopia, a developing country like Ghana, also revealed a 12-month prevalence of SBFs among health workers as 55.0%. 10
Despite previous efforts concentrating on minimizing healthcare workers and support staff’s exposure to blood and body fluids, there is limited data on mucocutaneous injury and its risk factors, particularly in low and middle-income countries.6,11–13 Additionally, amid this limited data on exposure to SBFs among healthcare professionals, those on healthcare supporting staff such as orderlies and medical waste handlers are almost not available since less attention is given to this group compared to doctors, nurses, midwives, laboratory scientists, and other traditional healthcare providers. Also, those few studies that looked at healthcare supporting staff considered them as part of the general health worker group,14–16 preventing the true picture of mucocutaneous injury among them.
In Ghana, there is limited data on exposure to SBFs among healthcare providers and healthcare support staff. 17 Nevertheless, few studies estimated the prevalence of SBFs without assessing their driving factors. A study estimated the prevalence of body fluid splashes among medical laboratory students at 21.3%, while another among health workers reported 60.5%.18,19 According to a recent scoping review, no study was found among hospital supporting staff regarding their exposure to splash of blood and other body fluids. 17 Recognizing this gap, this study, therefore, investigated the prevalence and risk factors of SBFs among healthcare supporting staff in the Greater Accra region, Ghana.
Study design, participants, and setting
This study utilized a cross-sectional design, employing a quantitative approach across multiple study facilities. The study included orderlies, laundry workers, and healthcare assistants from 10 hospitals located in the Greater Accra region of Ghana. Among these health facilities, four were privately owned while the rest were owned by the state. Specifically, the research was conducted at the following facilities: Weija-Gbawe Municipal Hospital, Ashaiman Community Hospital, Pentecost Hospital, Sakumono Community Hospital, Nyaho Medical Center, Shai-Osudoku Hospital, Tema General Hospital, Achimota Hospital, LEKMA Hospital, and Ga North Municipal Hospital.
The Greater Accra region hosts approximately 30.6% of all medical officers, nurses, midwives, and pharmacists in the country of Ghana. This estimation indicated the largest concentration of healthcare professionals within a specific region during the year 2015. 20 Per the Population and Housing Census, the Greater Accra Region accounts for roughly 17.7% of Ghana’s overall population. 21 This region exhibits a significant level of urbanization and is deemed to possess the highest population density due to substantial in-migration and population growth rates. 21
Sample size determination
The Cochrane formulae,
22
Sampling procedure
The primary sampling technique employed in this investigation was a multi-stage sampling approach. First, a purposeful selection of the Greater Accra region in Ghana was carried out. This was followed by the random selection of districts, hospitals, and study participants. Additionally, the selection of districts from the region, hospitals from districts, and study participants based on their occupation was guided by a probability proportional-to-size sampling technique. The Greater Accra region encompasses 29 districts, which include 2 metropolitan areas, 23 municipalities, and 4 districts. Out of these districts, 10 were chosen, representing more than 30.0% of the total number of districts. A total of 17 major hospitals were included in the sampling frame, and 10 of them were randomly selected for the study. Each district was represented by one major hospital. However, in cases where districts had two or three major hospitals, in which one hospital was chosen at random. The selection of major hospitals for the sampling frame was influenced by the 2021 annual outpatient department attendance data, this was retrieved from the District Health Information Management System. 26 Stratified random sampling was employed to recruit study participants based on their respective professions.
Inclusion and exclusion criteria
The study participants were healthcare support staff: health care assistants, laundry workers, and orderlies. Also, this category of workers should have worked in a hospital for the past year. Apart from the above-mentioned health workers, other healthcare staff were excluded. The 12-month assessment of the exposure to SBFs used did not permit newly recruited healthcare support staff to be part of the study.
Data collection
The data were obtained through a structured questionnaire, which primarily consisted of closed-ended questions in dichotomous, multiple-choice, and ranking scale formats. The questionnaire was developed for this study; however, certain questions were adapted from an already validated Healthcare Workers Safety and Health Survey questionnaire of the National Institute for Occupational Safety and Health and the US Centre for Disease Control and Prevention. 27 The questionnaire was divided into four sections, namely: the socio-demographic characteristics of the respondents; factors related to their occupation, organization, and behavior; factors about interventions; and the prevalence of body fluid splashes, consisting of 8, 7, 3, and 2 questions, respectively.
The study questionnaire underwent a pilot test. It was administered to 20 healthcare support staff members at Ho Teaching Hospital in the Volta Region of Ghana. The questionnaire was reviewed based on suggestions from respondents, occupational health experts, and stakeholders from the Ghana Health Service. Additionally, the final paper questionnaire was converted to the Open Data Kit (ODK), an electronic platform designed for data collection. 28 The self-administered paper questionnaire was distributed to selected participants, who were encouraged to complete it promptly. Nonetheless, some were given until the next day to complete it. Research assistants provided support to participants who needed assistance in completing the survey. Prior to their involvement in the study, all participants provided written consent. The data collection period spanned from January 30 to May 31, 2023.
Statistical analysis
The data collected on the paper questionnaire was inputted into the ODK platform. Following the export of the data from the electronic platform, 28 the STATA SE version 15 (64-bit) statistical analysis software 29 was utilized for data cleaning and analysis. An initial examination of all variables was conducted to ensure the presence or absence of missing values through primary analysis, including frequencies. Additionally, skewness and kurtosis tests 30 were performed on the study variables to determine their suitability for parametric or non-parametric tests.
Descriptive statistics, such as frequencies and percentages, were employed to provide a summary of categorical variables. On the other hand, continuous variables were summarized using the median and interquartile range. In establishing the initial associations between the prevalence of SBF (at least one incidence of SBFs in the past 12 months) and independent variables (socio-demographic, occupational organizational and behavioral factors, and intervention strategies), Chi-square, Fisher’s exact, and Mann–Whitney U tests31,32 were utilized. The analysis employed a statistical significance level of 95% confidence interval and a p-value of less than 0.05. Variables that exhibited significance at a p-value of less than 0.05 in the initial tests were incorporated into a log-binomial regression model. Finally, both crude and adjusted log-binomial regression analyses were employed. This was used to confirm the relationship between independent variables and the prevalence of SBFs.
Ethics approval
This research methodology was sanctioned by the Committee on Human Research Publication and Ethics (CHRPE) of Kwame Nkrumah University of Science and Technology, Kumasi, and given an approval reference number, CHRPE/AP/807/22. Additionally, it was authorized by the Ghana Health Service Ethics Review Committee, under the identity number GHS-ERC:012/03/23. The study was conducted in accordance with the Declaration of Helsinki.
Results and interpretation
Socio-demographic and lifestyle characteristics of healthcare support staff
Table 1 illustrates the socio-demographic and lifestyle characteristics of hospital support staff from 10 major hospitals in the Greater Accra region of Ghana. Out of the 149 participants, majority of them, 128 (85.9%) and 103 (69.1%) were orderlies/laundry staff and females, respectively. Most of the study participants were 30 years and above, and the median age was 33 years with an interquartile range (IQR), 30–40 years. Also, a greater portion of respondents, 117 (78.5%) had attained secondary education, and most (67.1%) were public hospital workers. Further, a little over two-thirds, 100 (67.1%) had 5 years and above working experience. The median working experience was 5 years with an interquartile range of 4–9 years. A huge number of study participants, 116 (78.0%) were permanent staff, and few, 31 (20.8%) were supervisors. Besides, a majority of them, 103 (69.1%) worked for 5 days and below within a typical working week.
Socio-demographic and lifestyle characteristics of healthcare support staff.

Occupational, organizational, behavioral, and intervention-related factors
With respect to occupational factors, almost all healthcare support staff, 140 (94.0%) occasionally experienced pressure from work, and the majority of them, 91 (61.1%) were exposed to a lot of stress. Regarding organizational factors, close to two-thirds, 93 (62.4%) and 98 (65.8%) had access to needed personal protective equipment (working gear, nose mask, headcover, protective shoes and gloves), and perceived understaff in their department, respectively. Also, concerning intervention strategies, about half of the study participants, 74 (49.7%) had training on standard precautions, and most of them, 99 (66.4%) confirmed the availability of systems used for reporting body fluid splashes in their facilities. With behavioural factors, a greater number of participants, 90 (60.4%) most of the time adhered to standard precautions (Table 2).
Occupational, organizational, behavioural, and intervention-related factors.

Prevalence of SBFs among healthcare support staff
As shown in Figure 1, 80 (53.7%) (95% CI: 45.3%–61.9%) healthcare support staff were exposed to SBFs in the past 1 year. The types of body fluids that were mostly encountered through these splash exposures were amniotic fluids (36.3%), urine (23.8%), blood (18.8%), and vomit (11.3%) (Figure 2).

Prior 1-year exposure to SBFs.
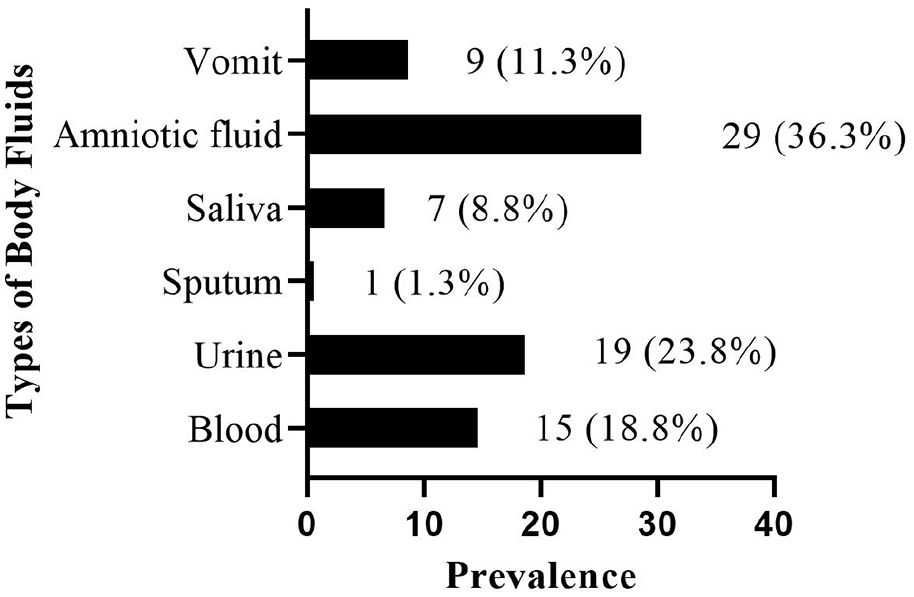
Previous 1-year exposure to types of body fluids.
Socio-demographic characteristics influencing body fluid splashes
Significant associations were found between gender (χ2 = 14.47, p-value < 0.001), category of health worker (χ2 = 7.31, p-value = 0.009), age (t = 3.45, p-value < 0.001), and exposure to SBFs. Also, current position (χ2 = 26.19, p-value = 0.009), and number of working days (χ2 = 14.48, p-value = 0.009) were also significantly related to exposure to SBFs (Table 3).
Socio-demographic and lifestyle characteristics influencing body fluid splashes.

p-values calculated from Fishers’ exact test.
p-values calculated from Mann–Whitney U test.
p-value < 0.05.
Occupational, organizational, behavioral, and intervention factors influencing body fluid splashes
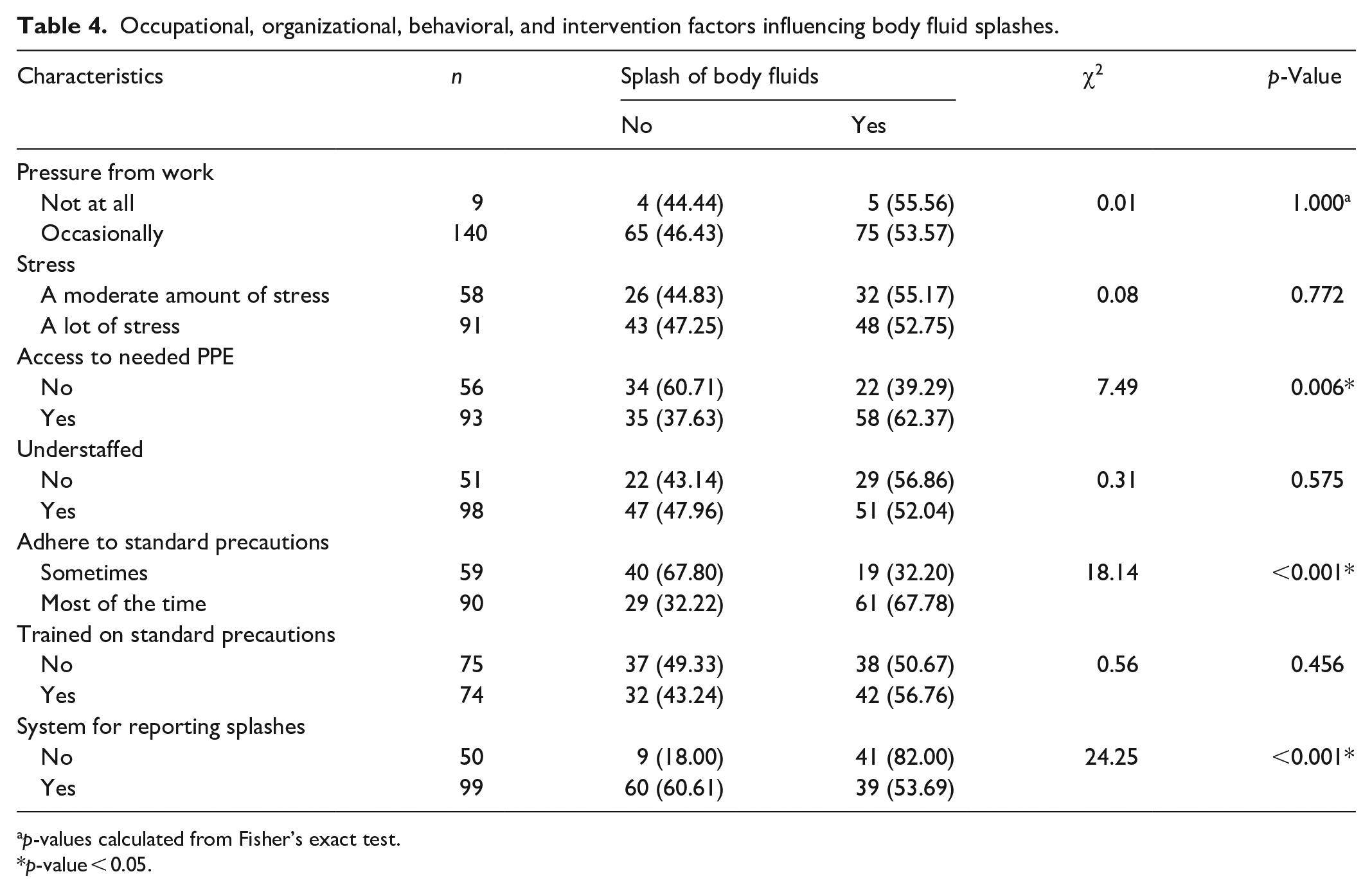
There was a significant relationship between access to needed personal protective equipment (PPE) (χ2 = 7.49, p-value = 0.006), adherence to standard precautions (χ2 = 18.14, p-value < 0.001), system for reporting splashes (χ2 = 24.25, p-value < 0.001), and exposure to SBFs (Table 4).
Occupational, organizational, behavioral, and intervention factors influencing body fluid splashes.
p-values calculated from Fisher’s exact test.
p-value < 0.05.
Factors associated with exposure to SBFs
Table 5 illustrates the results of bivariate and multivariate log-binomial regression analyses of risk factors and exposure to SBFs. All variables were significant on the bivariate log-binomial regression models; however, gender, category of worker, current position, adherence to standard precautions, and system for reporting splashes remained significant on the multivariate log-binomial regression model. The prevalence of SBFs was lower among male healthcare support staff (APR = 0.62, 95% CI: 0.41–0.93; p-value = 0.023), supervisors (APR = 0.24, 95% CI: 0.11–0.51; p-value < 0.001), and those who had a system for reporting splashes (APR = 0.61, 95% CI: 0.44–0.85; p-value = 0.004) compared to their counterparts who were females, held no positions, and had no system for reporting splashes. On the contrary, SBFs prevalence was higher among healthcare assistant staff (APR = 1.61, 95% CI: 1.16–2.22, p-value = 0.004), and workers who adhered to standard precautions most of the time (APR = 1.66, 95% CI: 1.11–2.48, p-value = 0.014) than orderlies/laundry staff, and those who only adhered to standard precautions sometimes, respectively.
Bivariate and multiple log-binomial regression of risk factors and exposure to splash of body fluids.

p-value < 0.05.
Discussion
This current study determined the prevalence and risk factors of SBFs among healthcare support staff. The prevalence of exposure to SBFs in the past 12 months was 53.7% (95% CI: 45.3%–61.9%). Amniotic fluid was the most common form of body fluid that splashed on hospital housekeepers. The prevalence of SBFs was lower among male healthcare support staff, supervisors, and those who had a system for reporting splashes. Nevertheless, SBFs prevalence was higher among healthcare assistant staff, and workers who adhered to standard precautions most of the time.
Our study revealed that 53.7% of healthcare support staff were exposed to SBFs. This study outcome was higher than those reported in studies conducted among health workers in Georgia (46.0%), 33 Ethiopia (39.0%), 34 and Nigeria (38.4%). 35 Also, our estimate was lower than similar studies in Cameroun (60.3%), and Addis Ababa (67.5%). Nonetheless, a recent study conducted by Sahiledengle et al. 10 stated a prevalence of 55.0%. This was consistent with our study result. The health worker category considered for study participation, assessment of splash exposures, and definition of exposure to body fluids are factors that may have contributed to the differences in prevalence of splash exposures. While our study considered only healthcare support staff as study participants, some of the studies aforementioned included all health workers. Some studies considered splash exposures as part of exposure to blood and body fluids, whereas others considered them as separate study outcomes. Also, numerous studies estimated the lifetime and prior 1 year prevalence of SBFs while others measured the previous 3-month exposure.
Although many studies34,36–39 failed to report the form of body fluids that were mostly involved in splash exposure in healthcare settings, our study found amniotic fluid to be the type of body fluid that was mostly experienced by hospital support staff. SBF occurrences involving amniotic fluid may be more prevalent among hospital housekeepers owing to their immediate proximity to pregnant women during labour and delivery procedures, and their involvement in preserving and managing the labour ward. In certain regions, attendants frequently aid healthcare experts during childbirth, which could also position them close to the expectant mother during labour and delivery. 40
Our research revealed that the prevalence of SBFs was lower among male healthcare support staff. Female healthcare support staff are mostly stationed at the delivery and labour wards, where body fluid splashes are frequent, hence, exposing them more to SBFs compared to their male counterparts. However, our outcome was in contrast to a recent study that found a correlation between gender and exposure to blood and body fluids and indicated a greater risk for males. 41 The dissimilarity in study findings might have resulted from the difference in study outcome variables. While our study considered exposure to SBFs, the outcome considered in the previous study may have included exposure to needlestick injuries as a form of exposure to blood and body fluids.
According to the present study, SBFs prevalence was higher among healthcare assistant staff. Although there is a lack of studies to confirm this finding among healthcare support staff, a recent systematic review and meta-analysis publication have shown that doctors, nurses, and midwives are mostly exposed to SBFs. 10 And due to the fact that healthcare assistants usually provide direct support to doctors, nurses, and midwives during their daily routine, it may account for why they are also at a greater risk among healthcare support staff.
Per our study findings, the prevalence of SBFs was lower among supervisors. However, there was a lack of evidence to support this study’s outcome from other studies. The level of exposure to SBFs can vary depending on the specific responsibilities of supervisors, and the policies and procedures in place at a health facility. Supervisors may be responsible for training and ensuring that their staff follow proper infection control protocols, including the safe handling and disposal of biohazardous materials. Therefore, supervisors not involved in basic housekeeping procedures might be the reason for their lower prevalence of exposure to SBFs among them.
Again, our study showed that the occurrence of SBFs was lower among healthcare support staff in facilities that had a system for reporting splashes. This result was comparable to the outcomes of studies carried out in Ethiopia 42 and South Africa. 43 The implementation of a reporting system enables healthcare support staff to quickly notify supervisors and managers. This also leads to the immediate addressing of instances of body fluid splashes, resulting in improved handling and prevention of exposure. The implementation of reporting systems for SBFs is mostly accompanied by regular training and education on splash exposures, which may task health workers to be conscious of their daily routines, and prevent the possible occurrence of body fluid splashes. These reasons may be responsible for the lower prevalence of SBFs in health facilities.
Furthermore, our study revealed a higher prevalence of SBFs among health workers who adhered to standard precautions most of the time. Housekeepers who adhered to standard precautions most of the time may be aware of their vulnerability to frequent exposure to SBFs in their line of duty. However, in similar studies, exposure to blood and body fluids was associated with lower compliance with standard precautions.44,45 Lower compliance has largely been associated with exposure to blood and body fluids in many studies. But the conflicting results may be due to how the level of adherence to standard precautions, and exposure to blood and body fluids were assessed.
The study was vulnerable to some limitations. The final questionnaire was not fully validated but was subjected to a pilot test, and reviewed by occupational health experts before being used for the survey. However, some portions of the data collection tool were adapted from an already validated questionnaire. The use of a cross-sectional study methodology is not capable of ascertaining the order of causality among varying factors. Furthermore, the investigation is susceptible to recall bias, due to the fact that respondents were questioned about events that occurred within the last 12 months. Finally, generalizations of the study results may not be applicable to minor healthcare facilities owing to the use of only major facilities in this current study.
Conclusion
A significant number of healthcare support staff were exposed to SBFs. The types of body fluids that were mostly encountered through these splash exposures were amniotic fluids, urine, blood, and vomit. Male healthcare support staff, supervisors, and workers in facilities that had a system for reporting splashes were associated with a lower prevalence of exposure to SBFs. Also, being a healthcare assistant staff, and a worker who adhered to standard precautions most of the time were related to a higher prevalence of SBFs exposure. Facility managers should enhance reporting systems to curb the exposure to body fluids among healthcare support staff. The study recommends adopting safety policies that serve the needs of hospital support staff.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241234473 – Supplemental material for Splash of body fluids among healthcare support staff in Ghana: a cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121241234473 for Splash of body fluids among healthcare support staff in Ghana: a cross-sectional study by Philip Apraku Tawiah, Emmanuel Appiah-Brempong, Paul Okyere and Mary Eyram Ashinyo in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241234473 – Supplemental material for Splash of body fluids among healthcare support staff in Ghana: a cross-sectional study
Supplemental material, sj-docx-2-smo-10.1177_20503121241234473 for Splash of body fluids among healthcare support staff in Ghana: a cross-sectional study by Philip Apraku Tawiah, Emmanuel Appiah-Brempong, Paul Okyere and Mary Eyram Ashinyo in SAGE Open Medicine
Footnotes
Acknowledgements
The authors express their sincere appreciation to the study participants and management of the chosen study health facilities, who devoted their time and resources to participate in this research endeavour. Your indispensable cooperation and eagerness to impart knowledge have substantially enriched the comprehensiveness and significance of our discoveries.
Author contributions
Conceptualization, PAT and EA-B; methodology, PAT and EA-B; software, PAT; validation, PAT, EA-B, and PO; formal analysis, PAT; investigation, PAT; resources, PAT; data curation, PAT; writing—original draft preparation, PAT; writing—review and editing, EA-B, PO, and MEA; visualization, PAT; supervision, EA-B and PO; project administration, PAT; All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.