
Abstract
Objectives:
Optimal adherence to antiretroviral therapy is required for viral load suppression. This study investigated the sociodemographic (age, sex, marital status, level of education, monthly income, settlement type, distance to the antiretroviral therapy-providing site, ethnicity) and health system (antiretroviral therapy-providing site) determinants of antiretroviral therapy adherence among human immunodeficiency virus-positive patients in the Volta Region, Ghana.
Methods:
A cross-section design was adopted, collecting data from 1729 human immunodeficiency virus patients and analysing them using STATA version 17 at level 0.05.
Results:
Antiretroviral therapy adherence was poor (51.2%). Being divorced (Adjusted odds ratio (AOR) = 0.65), widow (AOR = 0.58), cohabiting (AOR = 0.22), Ewe (AOR = 3.7), Ga/Dangbe (AOR = 2.27), living in a rural area (AOR = 1.54) and an urban area (AOR = 0.64), having a monthly income of GH₵1000 or less (AOR = 3.21), covering a distance of 51 km and above to the antiretroviral therapy centre (AOR = 1.79), receiving antiretroviral therapy from Ketu South Municipal Hospital (AOR = 0.09), Hohoe Municipal Hospital (AOR = 0.03), Ho Municipal Hospital (AOR = 0.02) and Ho Teaching Hospital (AOR = 0.09) were the determinants of antiretroviral therapy adherence.
Conclusion:
Antiretroviral therapy adherence was low. Interventions to improve antiretroviral therapy adherence should target these significant determinants.
Keywords
Background
Adherence to antiretroviral therapy (ART) is defined as taking all prescribed antiretroviral medications following the initiation of Highly Active ART in the correct doses at the prescribed time intervals and in the right manner, observing any dietary restrictions in at least 95% of the time. 1 Adherence is, therefore, a powerful determinant of the quality of life and survival among people living with the Human Immunodeficiency Virus (HIV) (PLHIV). 1
The 95-95-95 target, which aims to achieve 95% of PLHIV receiving ART, is one of the objectives of the Joint United Nations Programme on HIV/Acquired Immune Deficiency Syndrome (AIDS) (UNAIDS) Fast Track strategy to expedite actions to end the AIDS epidemic by 2030. 2 These goals are an update to the 2014 90-90-90 targets, which aimed to ensure that by 2020, 90% of PLHIV were receiving ART. 3
Optimal adherence is required for optimal viral load suppression and reduction in treatment failure. To ensure that there is optimal adherence to ART among HIV patients, the level of ART adherence as well as factors that influence adherence need to be determined. This will provide a scientific basis for the improvement of existing interventions to ensure optimal adherence to ART among HIV patients. Factors influencing ART adherence include demographic and socioeconomic factors such as sex, age, educational level, marital status, income, living place, employment and religion and health delivery factors.4–10
In a study conducted in sub-Saharan Africa (SSA), ART adherence among older adolescents was poorer than in other age groups with psychosocial, socio-economic, individual and treatment-related factors influencing adherence. 11 ART adherence is influenced by individual, health systems and environmental factors, which include treatment outcome, coping skills, disclosure, healthcare provider, family and support, organization of ART clinics, stigma and cost of transportation. Knowledge of one’s HIV status was a factor in ART adherence among adolescents.12,13 A study among eight SSA countries revealed stigma, ART side effects, lack of resistance and forgetfulness as barriers to ART adherence. 14 The findings of a study conducted in Yaounde, Cameroon proved that poor ART adherence is associated with the presence of depressed mood, virologic failure, disease progression and treatment failure. 15 Poor ART adherence can also lead to drug resistance strains of HIV leading to treatment failure and affecting immediate health outcomes. 2
Some studies have been conducted on ART adherence in Ghana: in the Volta Region, 16 in the Upper West Region, 17 in the Cape Coast Metropolis, 7 in the Sunyani Municipality 18 and the Western Region. 19 However, the study in the Volta Region was conducted at a single site (the then Volta Regional Hospital, Ho), which may not be a fair representation of the entire Volta Region. However, due to differences in sociodemographic and health system factors, it is imperative to investigate the determinants of ART adherence among HIV patients in the Volta Region of Ghana to improve adherence.
In the Volta Region, the prevalence of HIV is 3.0% and this is higher than the national prevalence of 1.7%. 20 This higher prevalence of HIV in the Volta Region compared to the entire Ghana necessitated the conduct of this study, which was to investigate the sociodemographic and health system determinants of adherence to ART among HIV patients in the Volta Region. The results of this study would guide interventions aimed at ending AIDS by 2030 in Ghana in general and the Volta Region in particular.
Methods
Description of the study site
The Volta Region is one of Ghana’s 16 administrative Regions, with Ho City designated as its capital. It is located west of the Republic of Togo and to the east of Lake Volta. The Region has a total of 18 administrative districts. It is multi-ethnic and multilingual, including groups such as the Ewe, Guan and the Akan people.
This study was conducted in 5 out of 19 hospitals offering ART services in the Volta Region. These included; Ketu South District Hospital, Ho Municipal Hospital, Battor Catholic Hospital, Ho Teaching Hospital, and Hohoe Municipal Hospital. These Hospitals were selected purposively to participate in the study as the top five Hospitals with new ART clients from 2014 to 2018. 21
In terms of availability of healthcare services, the Volta Region has a total of 749 health facilities: 29 Hospitals, 156 Health Centres, 44 Clinics, 4 Polyclinics, 14 Maternity homes, 452 CHPS Compounds and 50 private health facilities. 21
Study design
For the current study, a cross-sectional design was adopted, whereby data were collected from study participants between March and July 2021. It is an appropriate design because it enables a researcher to collect quantitative data to describe as well as establish associations between sociodemographic and health systems variables and ART adherence.
Eligibility criteria
ART clients from 2014 to 2018 aged 18 years and above who were on ART for at least 6 months and consented to participate, were included in the study. However, clients who were severely sick and needing urgent medical attention were excluded from the study.
Sample size
The sample size for the study was calculated using the formula for cross-sectional studies. 22 A non-response rate of 10% was added to the calculated sample size to obtain the sample size for the study.

Where n = required sample size, z = reliability coefficient (z-score) of 1.96 at 95% confidence level, p = estimated proportion of PLHIV who adhered to ART from a study conducted in the Upper West Regional Hospital, Ghana (62.2%), 17 and d = margin of error of 5% (0.05). The estimated sample size was calculated as follows:


Thus, the minimum sample size required for the study is 398. However, since this was a multi-centre study comprising five ART sites, a sample size of 1729 was used for the study. The number of ART-Naïve patients (patients who have never taken ART before) for the five study sites from 2014 to 2018 was 875 (for Ho Municipal Hospital), 717 (for Ho Teaching Hospital), 1314 (for Ketu South District Hospital), 635 (for Hohoe Municipal Hospital) and 729 (for Battor Catholic Hospital), giving a total of 4270 new HIV clients (Volta Regional Health Directorate [VRHD], 2018).
The sample size for each ART site was determined disproportionately by calculating the number of ART clients at that site out of the total number of ART clients from all selected sites multiplied by the overall sample size for the study. So, the sample size was allocated as follows: Battor Catholic Hospital: 702; Ketu South District Hospital: 312; Hohoe Municipal Hospital: 292; Ho Municipal Hospital: 212; Ho Teaching Hospital: 211.
Sampling
Multistage sampling was used for the study. The first stage involved purposively selecting the ART sites for the study based on the number of naïve ART clients from 2014 to 2018. The second stage involved the selection of the participants at each ART site using systematic sampling. At each ART site, a list of all ART clients who visited the site for ART services was obtained and served as the sampling frame. The sampling interval (Kth) was estimated as N/n, where N is the total number of ART clients at the ART site and n is the required sample size for that ART site. A number was randomly selected between 1 and Kth to serve as the starting point from which every Kth client on the sampling frame was selected until the required sample size for that site was attained. Any ART client selected, who met the eligibility criteria and gave written consent, was included in the study. Any selected client who declined to participate in the study was replaced by the next client to meet the sample size for that site.
Data collection instrument and procedure
Before data collection began, the ART clients were sensitised about the study for 1 month by the heads of the ART centres of the various Hospitals where data were collected for mobilisation purposes. A pretested standardised structured interviewer-administered questionnaire adapted from similar studies, 23 was used for data collection. Before data collection started, the instrument was pretested among a convenience sample of 10% of the planned sample size at a facility in the Volta Region, which did not have implications in the actual study. This was done to ensure the reliability and validity of the questionnaire, and the completion time. Since the ART providers at the various centres assisted with data collection, none of the clients who were approached for the study declined to participate. Also, research assistants interviewed participants using the structured questionnaire on the sociodemographic and health systems determinants of ART adherence. The questionnaire was prepared in English. However, data collection was done in a local language the respondents understood.
Study variables
ART adherence was the dependent variable in the study. It means taking all prescribed antiretroviral medications following the initiation of ART in the correct doses at the prescribed time intervals and in the right manner, observing any dietary restrictions at least 95% of the time. To determine the level of adherence, leftover pills were counted using the pharmacy system and reviewed by research assistants in addition to self-reporting by the participants. This was done by counting the number of pills the patient should have taken from the last visit and the number of extra pills that were returned on the current visit using the following example:
Previous date issued: 06/01/2018; total quantity taken at home: 67; Quantity returned: 15; Date returned: 03/02/2018; Days since last issue: 28; Regimens: 2 bid; Total supposed to take: 56; Total should have returned: 67–56 = 11; Pills missed: 15–11 = 4; Percentage adherence: (56−4)/56*100 = 92%; Adherence level = 92%.
The independent variables consisted of sociodemographic factors (sex, age, marital status, religious affiliation, ethnicity, highest level of education, income, employment status, settlement type, number of children, distance to ART site and duration on ART) and health systems factors (ART-providing site).
Data analysis
Data were entered using Epi-Data and exported to STATA version 17 (StataCorp LLC) (serial number: 401706369918) for cleaning, coding and analysis. Descriptive statistics including mean, percentages, frequencies and cross-tabulations were done. Continuous variables such as age were summarised and presented as means and standard deviations. Categorical variables were summarised into frequencies and percentages. Logistic regression in univariable and multivariable models was used to determine variables associated with ART adherence. Variables with a p-value < 0.05 in the univariable logistic regression model were candidates for multivariate logistic regression. The Hosmer-Lemeshow goodness of fit test was used to indicate the final model goodness of fit. 24 In Multivariable logistic regression, variables with a p-value < 0.05 were considered statistically significant.
Ethical consideration
Ethical approval was obtained from the University of Health and Allied Sciences Research Ethics Committee (UHAS-REC), Ho (UHAS-REC A.2[1]20-21). The clearance letter from the UHAS-REC together with introductory letters from the Principal Investigator (PI) were sent to the various institutions for permission to be granted for data collection to begin. Participant information and consent form describing the study was provided and explained to participants in the language they best understood and they gave informed written consent before being enrolled into the study. The PI ensured that no identifiable information that could be traced to any participant was captured on the questionnaire. Unique codes were assigned to each participant and were used for the analysis. Also, the participants were assured that any information provided would be strictly confidential and that only the PI and the Co-investigators would have access to the information provided.
Results
Sociodemographic and health system characteristics
Table 1 presents the sociodemographic characteristics of the participants. The Mean age of the respondents was 44.6 (SD: 12.6). The majority 1316 (76.1%) were females; most, 1115 (64.4%) were 40 years and above; 849 (49.1%) were married; most, 1597 (92.4%) were Christians; the majority, 1400 (81.0%) were Ewes; the majority, 1062 (61.4%) had less than secondary school level of education; most, 1277 (73.8%) had a monthly income of less than GH₵300; 1291 (74.6%) were self-employed; 1461 (84.5%) had children; 465 (26.9%) were living in the urban area; the ART site was within 50 km for majority 971 (56.2%) of the participants; the majority, 1052 (60.8%) took less than 1 h to get to the ART site; the majority, 1057 (61.1%) had been on ART for between 1 and 5 years and 702 (40.6%) received ART from the Battor Catholic Hospital. There was a significant association between age, marital status, ethnicity, level of education, monthly income, employment status, settlement type, distance to ART site, time taken to get to ART site, duration on ART and ART providing site and ART adherence (p < 0.001 for all).
Sociodemographic and health system characteristics (N = 1729).

HND: Higher National Diploma; OND: Ordinary National Diploma; GH₵: Ghana Cedis; * p<0.001.
Adherence to ART
Figure 1 presents the level of ART adherence, which was 51.2%.
Level of ART adherence.
Sociodemographic and health systems determinants of adherence to ART
Table 2 presents the odds of ART adherence based on the sociodemographic and health systems determinants. Those who were divorced (AOR = 0.65 (95% CI: 0.46–0.93); p = 0.017], widows (AOR = 0.58 (95% CI: 0.39–0.84); p = 0.004), cohabiting (AOR = 0.22 (95% CI: 0.11–0.46); p < 0.001) were less likely to adhere to ART than those who were legally married. The Ewes (AOR = 3.7 (95% CI: 1.76–7.76); p < 0.001) and the Ga/Dangbes (AOR = 2.27 (95% CI: 1.05–4.93); p = 0.037) were more likely to adhere to ART than the Akans.
Odds of ART adherence.
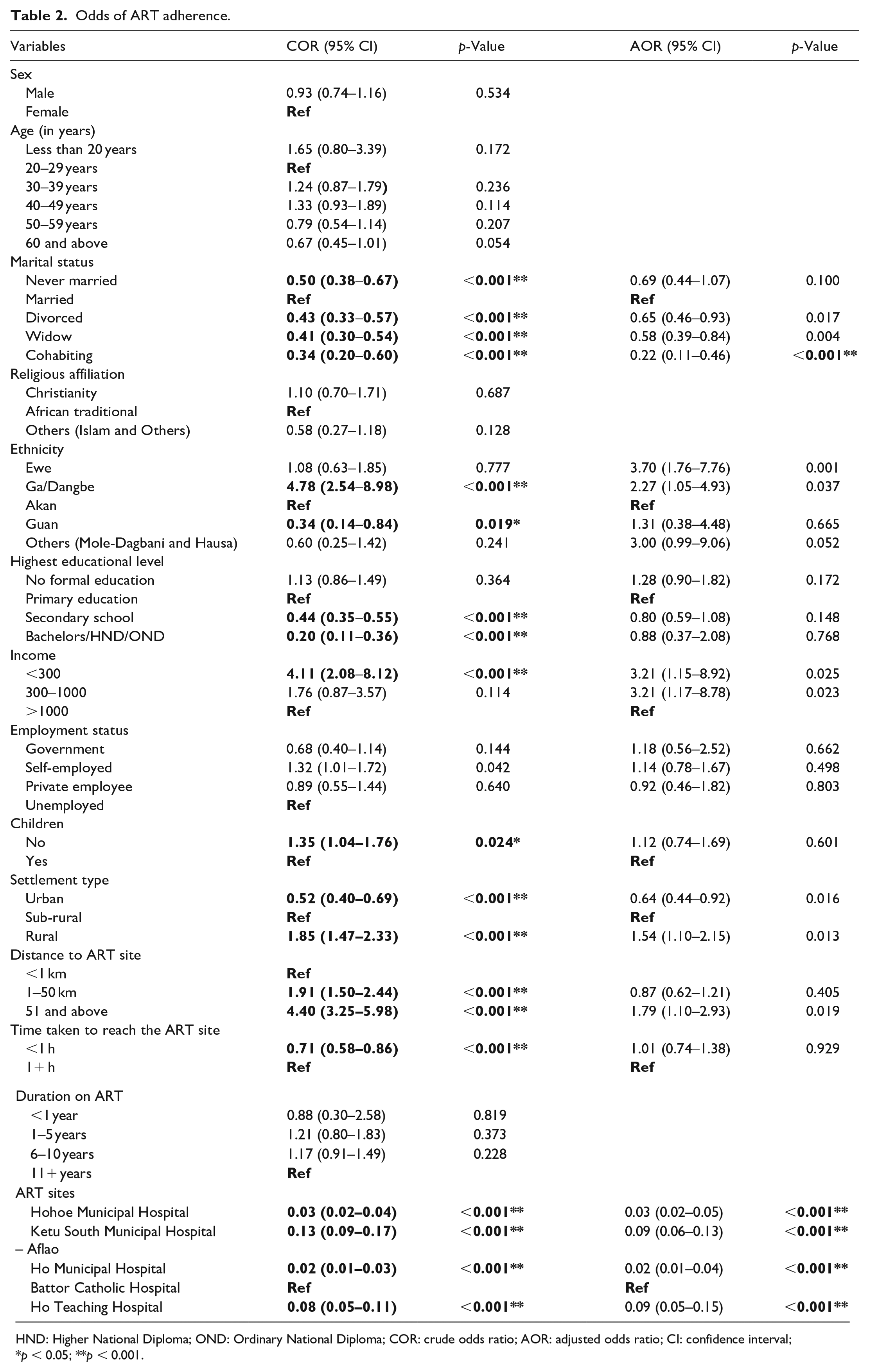
HND: Higher National Diploma; OND: Ordinary National Diploma; COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval; *p < 0.05; **p < 0.001.
Those who had a monthly income of less than GH₵300 (AOR = 3.21 (95% CI: 1.15–8.92); p = 0.025) and GH₵300–1000 (AOR = 3.21 (95% CI: 1.17–8.78); p = 0.023] were more likely to adhere to ART than those with a monthly salary of more than GH₵1000.
Those living in the rural areas were more likely to adhere to ART than those living in the sub-rural areas (AOR = 1.54 (95% CI: 1.10–2.15); p = 0.013], while those living in the urban areas were less likely to adhere to ART than those living in the sub-rural areas (AOR = 0.64 (95% CI: 0.44–0.92); p = 0.016). Those who covered a distance of 51 km and above were more likely to adhere to ART than those who covered a distance of less than 1 km to the ART site (AOR = 1.79 (95% CI: 1.10–2.15); p = 0.019).
Those who received ART from the Hohoe Municipal Hospital, Ketu South Municipal Hospital (Aflao), Ho Municipal Hospital and the Ho Teaching Hospital were less likely to adhere to ART than those who received ART from the Battor Catholic Hospital (AOR = 0.03 (95% CI: 0.02–0.05); p < 0.001), (AOR = 0.09 (95% CI: 0.06–0.13); p < 0.001), (AOR = 0.02 (95% CI: 0.01–0.04); p < 0.001), and (AOR = 0.09 (95% CI: 0.05–0.15); p < 0.001) respectively.
Discussion
The current study investigated the sociodemographic and health systems determinants of adherence to ART among HIV patients in the Volta Region of Ghana. ART adherence was 51.2%, which is similar to that of a previous study conducted in the Volta Region of Ghana at 51.4%, 16 but lower than those of previous studies conducted in the Upper West Region, Ghana at 62.2%, 17 in the Cape Coast Metropolis, Ghana at 79.5%, 7 in the Sunyani Municipality, Ghana at 75.0% 18 and in the Western Region of Ghana at 67.0%. 19 This shows that ART adherence in the Volta Region has been consistently low over the years. The current finding falls short of the recommended 95%. 2 This finding implies that a high proportion of HIV patients in the Volta Region of Ghana stand the risk of progressing to AIDS due to suboptimal adherence to ART. In the 2019 annual report of the Ghana AIDS/STI Control Programme (NACP), a low ART linkage rate and increased loss to follow-up of clients were reported as a challenge. In addition, it was found that ART sites have challenges in the distribution of last-mile ARVs. 25 These challenges could influence the low adherence observed in our study, as they could demotivate PLHIV in maintaining consistency at the ART centres, thus resulting in low ART adherence. It brings to bear the importance of addressing non-adherence using a multi-faceted approach. It is important to note that the NACP has a mandate among others, to provide treatment, care and support services for PLHIV.
Concerning the sociodemographic determinants, the results of the current study showed that marital status, ethnicity, living place, monthly income, and distance to the ART site were the significant sociodemographic determinants of ART adherence.
Regarding monthly income, patients with a monthly income of at most GH₵1000 were more likely to adhere to ART than those with a monthly income of more than GH₵1000. The finding disagrees with the finding of a previous study conducted in China, which reported that PLHIV with a high monthly income adhere to their medication as they may have the financial capacity to afford any cost related to their health. 26 The reason for the current finding could be because PLHIV with a high monthly income are more likely to be employed and as such spend much time at work impacting negatively their adherence to ART. Conversely, PLHIV with a low monthly income may not be actively employed and, therefore, may be extra careful about their health and in so doing, they will do their best to adhere to medication as prescribed by healthcare providers to avoid opportunistic infections and to prolong their lives. Also, people with a high income may lack confidence in ART since it is provided free of charge. They have the financial means to afford other alternatives to ART, which in turn may result in low adherence to ART. It implies that the rate of infection among this category of people will keep increasing since they are not taking measures to manage the disease. The progression of the disease to AIDS will also be faster among these people leading to a surge in the mortality rate of the disease. It is recommended that more campaigns should be done on the effectiveness of ART. This will help PLHIV become aware that ART is the best way to manage HIV and keep it from progressing to AIDS. This will go a long way to increase the confidence that PLHIV have in ART as a whole.
The current study also found that married patients adhere to ART more than those who had never married, divorced or cohabited, which is consistent with findings from previous studies.27,28 This finding could be attributed to married people having much influence from their spouses, and therefore, act in a way that will protect their spouses and children. This finding implies that the rate of infection will increase among people who are single, divorced or cohabiting, which will increase their mortality rate. Subsequently, the progression of the disease to AIDS will increase among these groups of people. It is recommended that education programmes on ART adherence should be organised, targeting PLHIV who are single, divorced or cohabiting.
Concerning participants who are cohabiting, a possible explanation is that there is a lack of security in relationships between partners that are cohabiting, particularly among the females. Most of them are afraid that they may lose their relationships if their partners discover that they are HIV-positive. As a result, they may not adhere to ART. Also, fear of stigmatisation from partners could be a major factor for low adherence to ART among people cohabiting. Subsequently, the rate of infection, as well as the mortality rate, will increase among those cohabiting. On the other hand, Adeniyi and Ajayi 28 found among postpartum mothers in South Africa that, knowing a partner’s HIV status, had a higher odds of adhering to ART. This reflects that transparency in the knowledge of one’s health status among couples promotes support for each other and hence adherence to medication including ART adherence. 28 It is recommended that public health interventions such as health education and health communications on ART adherence should target people cohabiting. Partners should be educated on how to stay and support each other to adhere to ART.
Regarding the place of residence, patients from urban areas were less likely to adhere to ART than those from rural and sub-rural areas. Our findings corroborate with those of a similar study in Ethiopia that urban dwellers are more likely to not adhere to ART compared to rural dwellers. 29 Further, our findings are consistent with a study conducted at Gonder University, Northeast Ethiopia. 30 The reason could be that patients from urban areas are more likely to have a job and as a result are so busy that they can miss taking their drugs, which would lead to non-adherence. Also, most people living in rural areas are more likely to have lower educational backgrounds and as a result, may have little information on the disease and its management. This may necessitate their adherence to the ART because they believe it is the best option for them to stay alive. Patients living in urban areas sometimes do not have the time to attend health programmes and as a result get most of their information online, where they get access to other alternatives to ART. This could deprive them of detailed and important information on ART and could make them prefer other alternatives than going to the HIV centres for ART. This confirms the report that due to active socio-economic adaptations in urban settings, higher levels of non-adherence to ART may occur. 31 The public health implication is that the rate of infection and mortality from AIDS in urban areas may continue to increase. It is recommended that educational programmes geared towards improving ART adherence should use social channels to reach people in urban areas. This is because most people in urban areas prefer getting health information on the Internet. This will ensure that there is more accurate and needed information online on the relevance of ART in HIV management.
Similar to previous findings in Tanzania 32 and in Togo, 33 the current study reported that patients with secondary education and higher were less likely to adhere to ART than those with primary education. The reason could be that highly educated patients are more likely to be employed and their busy schedule could cause them to forget to take their drugs, leading to suboptimal adherence. Also, this category of people is more knowledgeable about HIV and other remedies for reducing the viral load besides ART. Those with a primary level of education may be afraid of dying from the condition and may be convinced that adherence to ART will save their lives. The public health implication is that the rate of infection among patients with secondary education or higher will keep increasing since they are not taking measures to manage the disease. The progression of the disease to AIDS will also be faster among these people leading to a surge in the mortality rate from the disease. It is recommended that other strategies should be adopted in programmes to improve adherence to ART since being highly educated does not always translate into behaviour change.
Regarding ethnicity, the Ewes and the Ga/Dangbe were more likely to adhere to ART than the Akans. This could be because of ethnolinguistic barriers. In the Volta Region, the language of communication of the majority of the inhabitants is Ewe sometimes Ga/Dangbe. Therefore, patients who cannot communicate or understand these dialects may find it difficult to understand instructions on adherence from the ART providers. The public health implication is that there could be an increase in the rate of HIV infection and mortality among the Akans. It is recommended that educational programmes on ART adherence should be in different languages for non-natives to understand and opt for ART.
In contrast to previous findings, 34 the current study revealed that clients who covered a longer distance to the ART site were more likely to adhere to ART than those who covered a shorter distance. The current finding may arise from procrastination on the part of the clients who live closer to the ART site as a result of the proximity to the ART centres. This could result in forgetfulness from going for an ART refill. Forgetfulness is a barrier to ART adherence. 14 Also, clients who cover a distance of less than 1km to reach the ART centre are assumed to be recognisable in the social circle living close to the ART clinic. These people, due to stigmatisation, might avoid going for their medications at the nearby ART centres, leading to a lower likelihood of ART adherence.
Also contrary to previous studies which reported that low income was negatively associated with ART adherence, 35 the current study reported that patients with a lower monthly income were more likely to adhere to ART than those with a higher monthly income. This could be explained by the fact that clients with a low monthly income are aware of their low socio-economic status and, therefore, would not want to jeopardise their health status by not adhering to treatment. Also, those with a higher income are likely to be working in urban areas and are therefore likely not to adhere to ART because of their busy work schedules. As supported by the findings of the current study, patients living in urban areas were less likely to adhere to ART.
Concerning the health systems determinants, it was revealed that patients from Ho Teaching Hospital, Ketu South Municipal Hospital, Ho Municipal Hospital and Hohoe Municipal Hospital were less likely to adhere to ART than patients from the Battor Catholic Hospital. Since all the hospitals implement ART services under the same AIDS control programme in Ghana, a possible explanation could be related to differences in ART service delivery, which may be inherent to each hospital due to variations in human resources and the work environment. Apart from the Battor Catholic Hospital, the other four are public Hospitals, and therefore, there might be a higher degree of laissez-faire attitude among the service providers in these facilities compared to the Battor Catholic Hospital. Furthermore, Battor Catholic Hospital being a denominational facility, may be more organised compared to the public facilities, as projected by Adejumo et al. 11 who mentioned that the organisation of ART clinics influences ART adherence. The public health implication is that there will be low adherence to ART among patients who receive ART at these four public Hospitals, which might lead to a spike in the rate of infection and progression of the disease to AIDS. It is, therefore, recommended that strategies should be put in place in these public Hospitals to improve the healthcare delivery system. This would help improve the rates of adherence among PLHIV receiving services at these Hospitals using an institution-based approach.
Study limitations
The findings of the current study should be interpreted in the light of some limitations. First, being a cross-sectional study, causal relationships between ART adherence and the independent variables could not be ascertained. Due to the sensitive nature of the study, participants might have provided answers to questions, which were not the true reflection of the possible determinants of their ART adherence. Also, because participants knew that they were subjects in a study, they may have answered questions or performed differently. However, assurance of confidentiality might have mitigated these limitations.
Conclusion
ART adherence among HIV patients in the Volta Region of Ghana is far lower than the recommended 95%. Interventions to improve ART adherence should target clients who are divorced, widows, or cohabiting, as also the Akans, those living in the urban areas, those living close to the ART site and those receiving ART from public Hospitals.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241229056 – Supplemental material for Sociodemographic and health systems determinants of antiretroviral therapy adherence among human immunodeficiency virus-positive patients in the Volta Region of Ghana: A multi-centre study
Supplemental material, sj-docx-1-smo-10.1177_20503121241229056 for Sociodemographic and health systems determinants of antiretroviral therapy adherence among human immunodeficiency virus-positive patients in the Volta Region of Ghana: A multi-centre study by Elvis Enowbeyang Tarkang, Emmanuel Manu, Fortress Yayra Aku, Judith Anaman-Torgbor and Nelisiwe Khuzwayo in SAGE Open Medicine
Footnotes
Acknowledgements
Staff and patients of the various ART centres.
Authors’ contributions
EET conceptualised and designed the study and analysed the data; EET and JA-T collected the data; EET and JA-T supervised the data collection; EET, EM and JA-T led the writing of the manuscript; EET, FYA, JA-T, NK and EM critically reviewed the manuscript; All the authors read and approved the final version of the manuscript.
Availability of data
Data will be made available upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.