
Abstract
A gastric ulcer is a tear in the stomach lining that manifests as abdominal pain, nausea, vomiting, and weight loss. Its occurrence is lesser in children as compared to adults and its incidence in children ranges between 2% and 8%. Helicobacter pylori and nonsteroidal anti-inflammatory drugs are the most common causes of gastric ulcers. In our case, we report a 2.5-month-old male who presented with severe pallor, hematemesis, and melena with normal weight gain. The patient’s mother was infected with COVID-19 a month ago and recovered within 5 days but kept using aspirin and nonsteroidal anti-inflammatory drugs for a month during breastfeeding. An upper gastrointestinal endoscopy revealed a gastric ulcer and the Helicobacter pylori antigen was positive in the biopsy. A COVID-19 infection was detected later in the patient. The patient was administered proton pump inhibitor, clarithromycin, and amoxicillin for Helicobacter pylori antigen and symptomatic treatment for COVID-19. This case report shows that a stomach ulcer can appear in infancy, but opportune interventions such as timely diagnosis and treatment can solve the problem. It also marks the pathophysiological connection between Helicobacter pylori and gastric ulcer.
Introduction
A gastric ulcer is a tear in the stomach lining that grows over 5 mm in diameter and breaches the muscularis mucosa. It is curable as well as preventable. 1 The majority of gastric ulcers develop on the lesser curvature of the stomach at or near the antral side of the junction of the oxyntic and antral mucosa. 2 Gastric ulcers affect both men and women equally often, they less frequently appear before the age of 40, and the highest incidence is between the ages of 55 and 65. 2 In addition, the incidence in children ranges from 2% to 8%, which is lower than the incidence in adults, according to several worldwide research. 3 The two most common causes of ulcers are gastric prostaglandin loss caused by nonsteroidal anti-inflammatory drugs (NSAIDs), and Helicobacter pylori (H. pylori) infection. 1 Abdominal pain is the most common symptom, along with nausea, vomiting, gastrointestinal (GI) bleeding, and weight loss. The initial evaluation primarily includes a thorough history taking and a physical examination. Endoscopic or radiologic investigations are then used to confirm the diagnosis. 2 Suppose H. pylori infection is detected through biopsies taken via endoscopy or laboratory tests. In that case, antibiotic therapy becomes a necessary step in the course of treatment, after which H. pylori eradication must be verified. 1 The major complications of gastric ulcers include bleeding, perforation, penetration, and gastric outlet obstruction. 4 The differential diagnoses include gastritis, esophagitis, inflammatory bowel disease, pancreatitis, and many more. 2 We herein report an extremely rare case of gastric ulcer bleeding in a 2.5-month-old male infant suffering from coronavirus disease 2019 (COVID-19) without a known inciting perinatal event.
Case presentation
A 2.5-month-old male presented with severe pallor, hematemesis, and melena for a week. The hematemesis occurred four times a day but only after breastfeeding, while weight gain remained good. The patient was developing normally until this admission when he suffered, besides the symptoms mentioned previously, from severe progressive pallor with hemoglobin of 3 g/dL that required a blood transfusion. The infant’s weight was 5.5 kg, length 58 cm, and head circumference 38 cm. His mother was infected with COVID-19 about a month ago, from which she recovered within 5 days and then continued to take an unknown amount of aspirin and NSAIDs for a month during breastfeeding without consulting a physician. Clinical examination of the baby showed severe pallor, pulse of 140 bpm, and capillary refill time less than 3 s, along with other normal findings. The results of laboratory tests after the blood transfusion are shown in Table 1.
Laboratory tests after the blood transfusion.

Table 1 shows that the patient had a low hemoglobin level due to the gastric bleeding while other laboratory tests were all normal.
Furthermore, WBCs and RBCs were found in a stool test while the stool culture was negative. An upper GI endoscopy was performed, which revealed a bleeding gastric ulcer on the greater curvature (Figure 1). The treatment was symptomatic, consisting of putting the baby on a diet, administering intravenous fluids, intravenous omeprazole, blood transfusion when needed, and vitamin K. Upper GI endoscopy was re-performed 5 days later with ulcer biopsies taken. The pathological examination showed chronic gastritis (Figure 2), and the H. pylori antigen was positive (Figure 3). Subsequently, the patient administered proton pump inhibitor (PPI), clarithromycin, and amoxicillin for 14 days. During the eighth day of treating H. pylori, an infant in the same hospital room was diagnosed with COVID-19, after which a polymerase chain reaction (PCR) screening was administered for all the children in the room, revealing a COVID-19 infection in the patient with the ulcer as well. The patient then received symptomatic COVID-19 treatment in addition to the H. pylori treatment. With hemoglobin values returning to normal, clinical improvement and hemodynamic stability were observed, after which the child was discharged, with a recommendation to repeat the endoscopy and the PCR after a month. In a follow-up after 7 months, the child was completely healthy, weighing 9 kg, and was 72 cm tall. Clinical examination and laboratory tests were normal, and the H. pylori antigen in the stool was also negative.

A gastrointestinal endoscopic examination. Upper gastrointestinal endoscopy showing a bleeding gastric ulcer.

Pathological image of the biopsy specimens. A gastric biopsy showed chronic gastritis and little inflammatory infiltration with lymphocytes (hematoxylin and eosin staining).
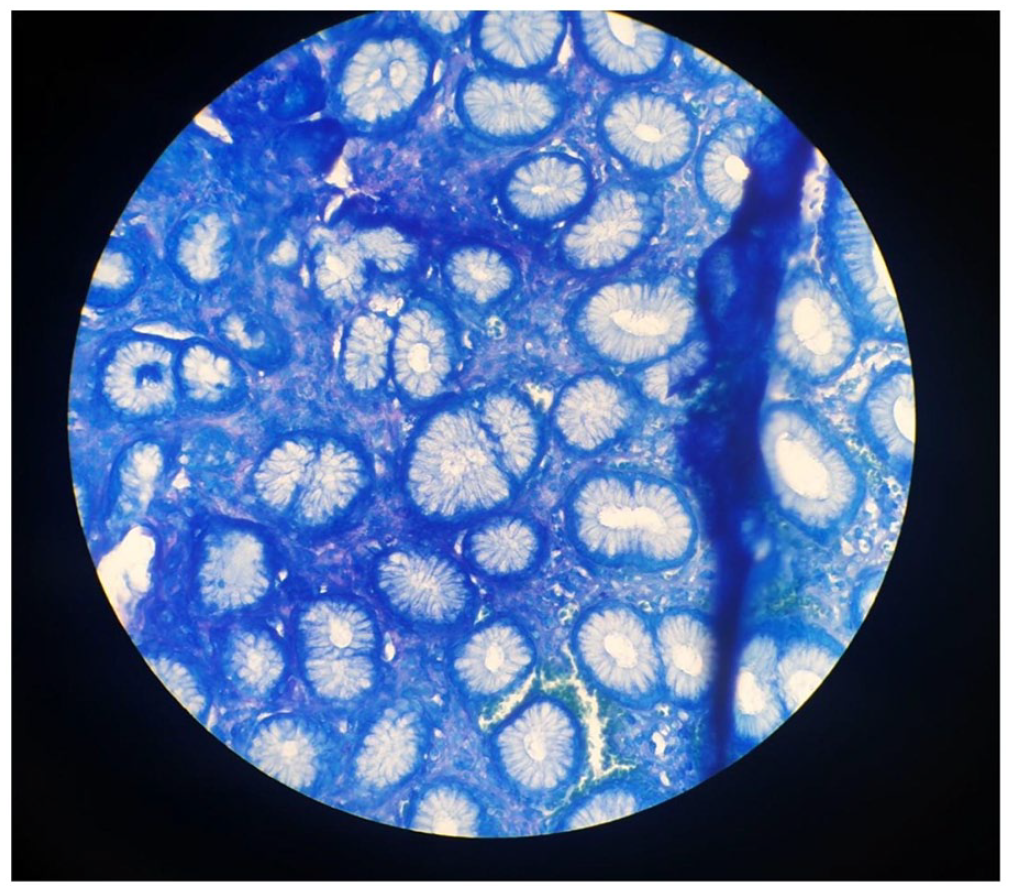
Helicobacter pylori (red arrow) in gastric biopsy (methylene blue staining).
Discussion
A gastric ulcer refers to a lesion in the stomach mucosa that exceeds 5 mm in diameter and penetrates the muscularis mucosa. 1 The global occurrence of peptic ulcer disease (PUD) in the general population has likely decreased over time, particularly in high-income nations, from a previously estimated prevalence of 5%–10% and yearly incidence of 0.1%–0.3%. 5 In addition, the occurrence of PUD in children is less frequent than in adults. According to various international studies, PUD incidence in children ranges from 2% to 8%. 3 Nevertheless, there is a limited number of studies that have investigated the occurrence of PUD in children. Therefore, what makes our case highly distinctive is the occurrence of the ulcer at such a young age, just 2.5 months old. Although previous literature indicates that the majority of ulcers occur on the lesser curvature, 2 our patient’s ulcer developed on the greater curvature and was bleeding during the endoscopy. Adults with gastric ulcers typically experience symptoms such as abdominal pain, nausea, vomiting, GI bleeding, and weight loss. 2 By contrast, younger patients commonly present with symptoms including irritability, poor feeding, regurgitation, vomiting, GI bleeding, or poor weight gain. 3 The patient under consideration presented with severe pallor, melena, and post-breastfeeding hematemesis, yet maintained normal weight gain. Gastric ulcers can be attributed to various factors, with the most prominent being long-term use of NSAIDs and H. pylori infection. 1 To diagnose our patient, an endoscopy was performed, and a biopsy was taken, indicating chronic gastritis and a positive H. pylori antigen.
H. pylori is a slender, curved bacteria measuring 0.5 µm × 3.0 µm in size and belongs to the gram-negative category. These microorganisms are known to generate enzymes such as urease, catalase, and oxidase. 6 In 1983, H. pylori was first identified, and then, in 2005, Robin Warren, a keen-eyed pathologist, and Barry Marshall, an innovative physician from Australia, were jointly honored with the Nobel Prize in Medicine for their groundbreaking discovery of this bacterium and its connection to PUD and gastritis. 7 The colonization of H. pylori is the primary reason for chronic gastritis, and it is also linked to the development of duodenal ulcers, gastric ulcers, gastric adenocarcinoma, and mucosa-associated lymphoid tissue lymphoma. 8 The presence of H. pylori in children under the age of 1 was 28.7%, and this percentage rises as children get older, reaching 40.0% among those aged 9–12 years. 9 Thus, another noteworthy aspect that distinguishes our case is the detection of H. pylori at this remarkably early age (2.5 months).
How H. pylori is acquired and transmitted remains uncertain. 6 Nevertheless, it seems that person-to-person transmission, either through oral contact (such as vomit and possibly saliva) or through contact with fecal matter, is the primary mode of transmission. 10 Therefore, there is a high possibility of catching H. pylori from the mother or other people who live in the same house. In fact, many factors linked to increased H. pylori prevalence were mentioned in more than one study including low socioeconomic status indicators, household crowding, urban residence, having H. pylori-infected parents, number of children in the home, high-ranking birth order, institutional residence, indicators of poor nutritional status, drinking water source, consumption of raw vegetables, and migration from high prevalence region. 8 In addition, several studies have shown that the acquisition of H. pylori in infancy continues to be common in many countries, particularly in low-income and middle-income countries. 10 Moreover, Torres et al. have found that breastfed infants were more likely than non-breastfed infants to become infected patients. 8 Our patient lives in a low-income country “Syria” within a low socioeconomic family; hence, he might have acquired H. pylori from his mother or family through person to person route (oral contact) excluding the fecal-oral route because the stool culture was negative.
The precise mechanism through which H. pylori induces gastric inflammation remains unclear. However, a potential contributor to gastric damage could be the significant presence of urease in H. pylori. Urease can break down urea into ammonia and bicarbonate at the surface of the gastric mucosa. Ammonia can directly harm epithelial cells, and the simultaneous increase in mucosal surface pH might disrupt the functioning of gastric epithelial cells, including mucus production. Apart from urease, substantial research has been dedicated to the H. pylori vacuolating cytotoxin over the years. Strains that produce this cytotoxin tend to exhibit greater virulence compared to those that do not produce it. 6
The preferred treatment options for eliminating H. pylori in both adults and children are amoxicillin combined with clarithromycin and a PPI. In addition, the use of omeprazole, metronidazole, and clarithromycin together has also shown success rates of approximately 90%. Furthermore, efforts to enhance effectiveness involved assessing 7- and 14-day courses of omeprazole, amoxicillin, and clarithromycin. The eradication rates using this treatment were 57% for the 7-day course and 62% for the 14-day course. To sum up, treatment regimens for H. pylori-infected children should include a PPI along with a minimum of two antibiotics, such as clarithromycin and amoxicillin. 8 Our patient was successfully treated with a PPI, clarithromycin, and amoxicillin for 14 days.
Finally, one of the main sources of uncertainty in pediatric H. pylori research stems from the ongoing debate over whether the symptoms in children are genuinely linked to H. pylori infection. This uncertainty primarily arises from the lack of clearly defined criteria for GI symptoms in H. pylori-infected children. 8 Hence, H. pylori can lead to gastric ulcer before it is detected and that is what probably happened with our patient taking into consideration all the risk factors he has.
Although we mentioned before in the presentation that the mother of our patient was taking NSAIDs during the first month of breastfeeding, these medications possibly did not play a role in causing the gastric ulcer. To elucidate, NSAIDs, as acidic medications, possess attributes such as minimal lipid solubility and strong protein binding (exceeding 90%), which reduce the likelihood of significant transmission into breast milk. High protein binding and restricted absorption in the GI tract minimize the extent to which infants are exposed systemically to the drug through ingested breast milk. 11 But what might contribute to the pathogenesis of the ulcer is the use of aspirin; since aspirin remains present in maternal milk for as long as 24 h, and the infant’s metabolism is relatively sluggish. Even with just one dose, once breastfeeding is well established, the infant may encounter approximately 9%–21% of the dose consumed by the mother. In conclusion, when it comes to short-term use, the majority of NSAIDs pose minimal risk to the nursing infant, except aspirin when taken in doses exceeding 150 mg per day. 11
In addition, during the treatment for H. pylori, our patient was found to be infected with COVID-19 through PCR screening. Few reports are still debatable on how COVID-19 infection can exacerbate gastric inflammation, but a study conducted by Mauro et al. examined the endoscopic findings in COVID-19 patients who presented with GI symptoms. According to Mauro et al., active ulcers were observed in nearly half of the patients (44%), making it the most common endoscopic finding. 12 However, there is not enough evidence of this in our case.
This case report shows that a stomach ulcer can appear in infancy, but opportune interventions such as timely diagnosis and treatment can solve the problem. It also marks the pathophysiological connection between H. pylori and gastric ulcers.
Conclusion
Based on the results, it can be concluded that gastric ulcers seldom appear in infancy unless many risk factors, such as H. pylori infection, exposure to aspirin, and living in low socioeconomic status exist.
Footnotes
Acknowledgements
We wish to show our appreciation to
Author contributions
N.M. is the corresponding author. Also, contributed to drafting, editing, reviewing, and bibliography. The author reviewed and accepted this paper. M.A.K. contributed to drafting, editing, reviewing, and bibliography. The author reviewed and accepted the paper. M.B. contributed to drafting, editing, reviewing, and bibliography. The author reviewed and accepted the paper. M.A.K. and M.B. are co-first authors. All contributed equally. M.J. contributed to the conceptualization, editing, reviewing, and bibliography. The author reviewed and accepted the paper. J.M. is the supervisor and contributes to editing and reviewing. The author reviewed and accepted the paper. All authors reviewed and accepted the paper.
Data availability statement
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient’s parents for the anonymized information to be published in this article.
Provenance and peer review
Not commissioned, externally peer reviewed.