
Abstract
Objective:
This study utilized a sample of trangender, nonbinary, and gender-diverse (TGD) patients to build on emerging literature that suggests that hypermobile Ehlers–Danlos syndrome may be overrepresented in TGD populations. The objective of this retrospective chart review was to determine the prevalence of hypermobile Ehlers–Danlos syndrome syndrome at a gender-affirming primary care clinic.
Methods:
A retrospective chart review of medical records was conducted with records between May 2021 and June 2024. Eligible participants were active patients at the gender-affirming primary care clinic, who were over the age of 16, were TGD, and had a diagnosis of hypermobile Ehlers–Danlos syndrome. Of 2180 patients over the age of 16, 59 patients met the criteria. The primary outcome was the prevalence of hypermobile Ehlers–Danlos syndrome in the sample, summarized by frequency and percentage. Secondary outcomes were the prevalence of associated clinical features within the sample of TGD patients with hypermobile Ehlers–Danlos syndrome.
Results:
The prevalence of hypermobile Ehlers–Danlos syndrome syndrome was 2.7%. Within the sample of patients with hypermobile Ehlers–Danlos syndrome, 81.4% were found to have diagnoses of anxiety, depression, or attention deficit hyperactivity disorder, 50.8% had a history of migraines or dysautonomia, 39.0% had a history of gastroesophageal reflux disease, irritable bowel syndrome, nausea, diarrhea, or gastroparesis, 16.9% had history of mast cell activation disorder, 32.2% had postural orthostatic tachycardia syndrome, 30.5% had dysmenorrhea, 83.1% reported chronic pain, and 44.1% reported chronic fatigue.
Conclusions:
We found that 2.7% of the 2180 patients had a diagnosis of hypermobile Ehlers–Danlos syndrome syndrome. The sample had notably high rates of medical comorbidities as well as anxiety, depression, or attention deficit hyperactivity disorder, consistent with emerging research. The results support the intersecting psychological and healthcare vulnerabilities of TGD patients with hypermobile Ehlers–Danlos syndrome. Further research in this intersection could support mitigation of health care disparities that affect TGD patients with hypermobile Ehlers–Danlos syndrome syndrome.
Key points
Background
Ehlers–Danlos syndrome (EDS) describes a group of connective tissue disorders encompassing 14 different subtypes with variable clinical presentations. 1 EDS has an estimated prevalence of 1 in 5000 people (0.02%), although there is limited evidence to support this statistic, suggesting potential underestimation. 2 Hypermobile EDS (hEDS) is the most common type of EDS, and it is the only subtype without a known genetic marker. Diagnosis of hEDS relies on clinical diagnostic criteria due to the absence of specific testing, which likely contributes to underdiagnosis. 2 Those who exhibit symptoms of joint hypermobility but do not meet the criteria for hEDS are classified as having hypermobility spectrum disorder. 2
HEDS presents heterogeneously along a spectrum of severity but is commonly characterized by generalized joint hypermobility, musculoskeletal pain, and cutaneous manifestations. 3 Individuals with hEDS frequently experience several comorbidities, including chronic pain, fatigue, autonomic dysfunction, gastrointestinal issues, cardiovascular, neurological, gynecological, and psychological challenges. 3 With no curative treatments available, care for hEDS focuses on managing symptoms, alleviating pain, and preventing joint injury. 4 Due to the variability in clinical presentation, lack of diagnostic tests, and limited awareness among healthcare providers, patients often face significant delays in obtaining a diagnosis of hEDS. 5
Transgender, nonbinary, and gender-diverse (TGD) individuals experience significant healthcare disparities compared with cisgender individuals due to a complex interplay of institutional systems that reinforce structural oppression and inequities. 6 The disparities may be due in part to discriminatory treatment from providers, such as misgendering or refusal to provide care. 7 Data from the U.S. Transgender Survey indicates that nearly a quarter of TGD respondents avoided seeking medical care due to anticipated discrimination. 8 In addition to interpersonal discrimination, TGD individuals also encounter systemic barriers, including lack of insurance and limited access to gender-affirming services, which further complicate their healthcare experiences and contribute to poor health outcomes. 7
Research on hEDS within TGD populations is limited, but two recent studies suggest a higher prevalence of hEDS in this community compared to the general population.9,10 One study of adolescents at an EDS clinic and found that 17% of patients reported gender dysphoria, which is 13 times the estimated prevalence of gender dysphoria in the general population. 9 Within this group, 82% had hEDS, suggesting that gender-diverse identities may be more common among individuals with hEDS. Another study at a gender-affirming surgery clinic found that 2.6% of 1363 patients had an EDS diagnosis, with 72% of these individuals diagnosed specifically with hEDS. 10 Both studies noted high rates of comorbidities, including chronic pain, fatigue, postural orthostatic tachycardia syndrome (POTS), dysautonomia, anxiety, and depression, underscoring the need for more research into the intersection of hEDS and TGD populations.9,10
Individuals with hEDS often encounter obstacles in accessing healthcare and obtaining an hEDS diagnosis. 3 Considering the healthcare discrimination faced by TGD individuals, 8 it is plausible that this population may experience amplified barriers in seeking care for hEDS. The aim of this review is to contribute to emerging research suggesting that hEDS may be more common than previously thought, with a particular focus on its prevalence within the TGD community. As trans and queer researchers, we are not interested in exploring a biological etiology of gender diversity; rather, we aim to highlight the intersectional vulnerabilities of TGD individuals with hEDS and to promote equity in healthcare access and treatment.
Methods
Study design
A retrospective chart review was performed between May 2021 and July 2024 at a gender-affirming primary care clinic.
Patients were included if they met the following criteria: aged 16 years or older, transgender, nonbinary, and gender-diverse, visited the clinic in the last 3 years, and had a diagnosis of hEDS. The presence of International Classification of Diseases, 10th Revision (ICD-10) code documented in the medical record specific to hypermobile EDS was used to confirm diagnosis.
Patients were excluded if they were under the age of 16, cisgender, or lacked a documented clinic visit within the past 3 years. Additionally, patients with ICD-10 codes indicating hypermobility syndrome, hypermobility spectrum disorders, or unspecified types of Ehlers–Danlos Syndrome were also excluded. Ultimately, 59 patients met the inclusion criteria (Table 1).
Demographic characteristics of participants.
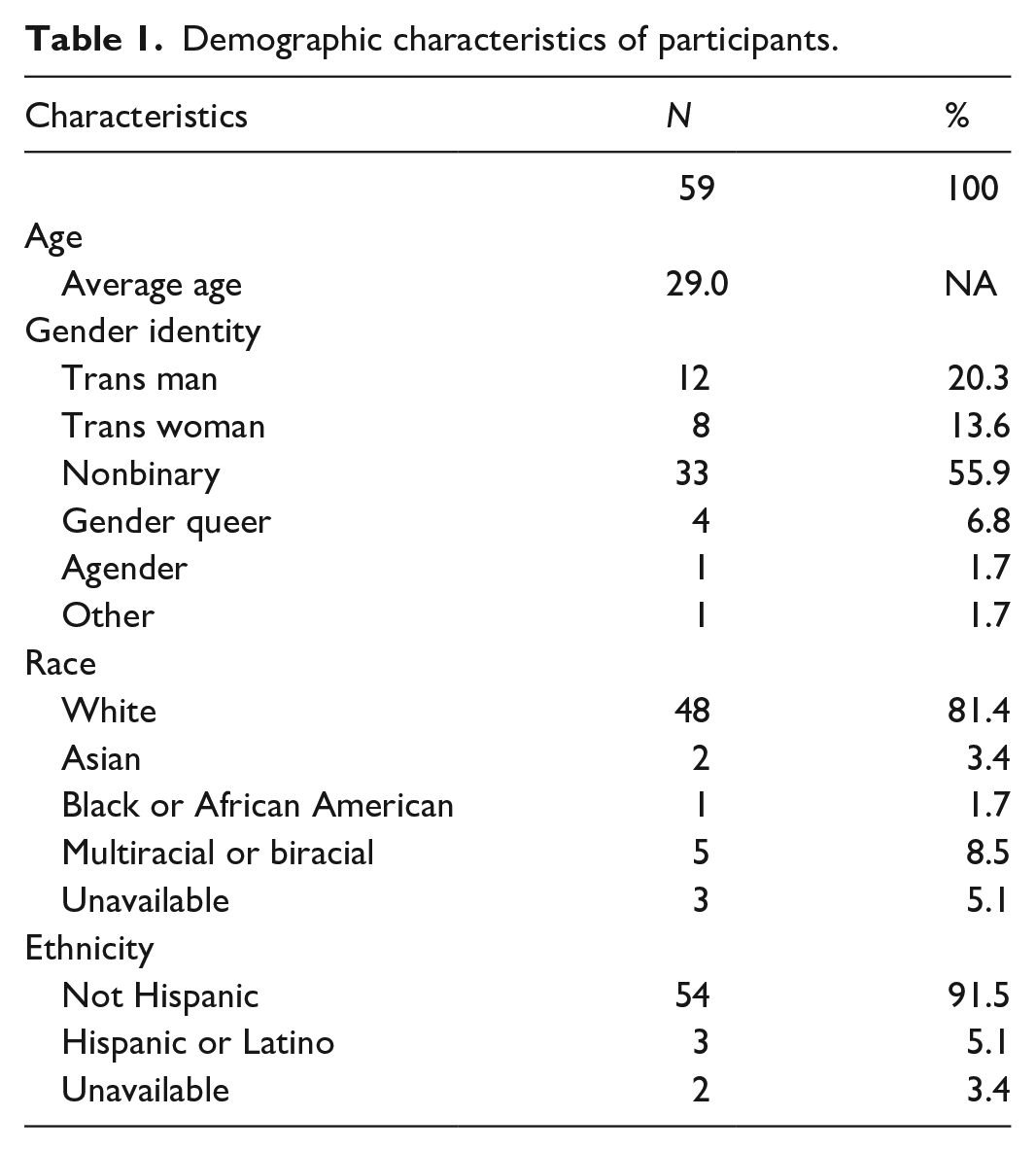
Chart review included analysis of documents in the electronic medical record, including problem lists, diagnoses, and clinical notes. Data collected included the presence of a hEDS diagnosis, demographic information, clinical symptoms related to hEDS, and comorbidities often associated with hEDS. These comorbidities, as outlined in Table 2, were selected based on commonly reported comorbidities associated with hEDS as well as prior research exploring the prevalence of hEDS in transgender populations.9,10 Clinical symptoms such as chronic generalized pain and fatigue were documented based on existing research, which shows that these are commonly recognized symptoms in individuals with hEDS. The patient’s gender identity was identified from the sexual orientation and gender identity designation in Epic which captures assigned sex and birth and gender identity. 11
Medical conditions of participants.

GERD: gastroesophageal reflux disease; IBS: irritable bowel syndrome; POTS: postural orthostatic tachycardia syndrome; ADHD: attention-deficit hyperactivity disorder.
Statistical analysis
The results were analyzed and binary and categorical variables were summarized by frequency and percentage. All statistical analyses were performed using Microsoft Excel.
Ethical approval and informed consent
Institutional review board approval was obtained from Tufts University School of Medicine (IRB STUDY00004950). In accordance with 45 CFR 46.116(f), the IRB granted a waiver of written informed consent. Additionally, the waiver for parent/guardian permission was granted in accordance with 45 CFR §46.408(c) and 45 CFR §46.116(f). The waiver for minor assent was granted in accordance with 45 CFR §46.408(a) and 45 CFR §46.116(f).
Results
Patients were predominantly white and non-Hispanic (81.3%). The entire sample was transgender, nonbinary, or gender diverse; 55.9% were nonbinary, 20.3% were trans men or trans masculine, and 13.6% were trans women or trans feminine. The remainder of patients were either genderqueer (6.8%) or agender (1.7%). One patient reported their gender as “other.” The average age of patients included in the sample was 29 (Table 1).
Of the 2180 patients over the age of 16 at the clinic, 59 (2.7%) had a diagnosis of hEDS (Table 2).
Eighty-three percent of patients reported chronic pain and 44.1% reported chronic fatigue. Eighty-one percent of patients had diagnoses of depression, anxiety, or attention-deficit hyperactivity disorder (ADHD), 50% had diagnosed migraines or dysautonomia, 39.0% had diagnosed gastroenterological issues of gastroesophageal reflux disease, irritable bowel syndrome, nausea, diarrhea, or gastroparesis, 16.9% had diagnosed mast cell activation syndrome, and 32.2% had POTS (Table 2).
Discussion
We found that 2.7% of patients over the age of 16 at a gender-affirming primary care clinic had a diagnosis of hEDS. These findings align with existing research on the prevalence of hEDS among TGD populations; however, our study provides a larger sample within the unique context of a clinic offering both primary and gender-affirming care to transgender and gender-diverse individuals (Table 3).9,10 This study builds on emerging literature suggesting that hEDS may be both underreported in general and overrepresented within the TGD community, warranting additional research into the intersecting vulnerabilities for these patients.
Current research on Ehlers–Danlos syndrome in the transgender community.

EDS: Ehlers–Danlos syndrome; GERD: gastroesophageal reflux disease; POTS: postural orthostatic tachycardia syndrome; ADHD: attention-deficit hyperactivity disorder.
Historically, EDS and hEDS have been characterized as rare disorders, with an estimated general population prevalence of 0.02% for EDS with hEDS being the most common subtype. Clinicians’ perception of hEDS as a rare disease may contribute to delays in diagnosis after a patient’s initial clinical presentation. Patients with hEDS and other hypermobility spectrum disorders often experience a prolonged time between their first clinical symptoms and the actual diagnosis, with an average time elapsed of 14 years; for 25% of patients the delay can last over 28 years. 12 Such diagnostic gaps can exacerbate symptoms, increase complications, and contribute to long-term disability, highlighting the need for clinician education on hEDS in both general and gender-affirming care settings.
Our sample also displayed high rates of comorbid conditions, including POTS (32.2%) and mast cell activation disorder (16.9%), consistent with existing literature suggesting potential associations among POTS, hEDS, and mast cell activation disorder. 13 One study of 91 patients with POTS found that 31% met clinical criteria for hEDS. 14 Yet, a 2020 review reported that these conditions are too poorly defined to establish an association. 15 Research on the prevalence of POTS in transgender populations is limited. Although one study documented symptomatic improvement of POTS in three transmasculine patients after initiating testosterone therapy, it did not aim to quantify the prevalence of POTS in transgender populations. 16 Similarly, there is no specific prevalence data on mast cell activation syndrome in transgender populations, underlining an important research gap.
Previous research has identified links between hEDS and chronic pain and fatigue, patterns also observed in our sample. Individuals with hEDS frequently experience soft tissue injuries leading to joint pain, which can progress to widespread musculoskeletal pain. This pain may be exacerbated by hyperalgesia, likely driven by central sensitization, resulting in heightened pain sensitivity. 2 In addition, the fear of pain and injury may reduce physical activity, contributing to deconditioning and increasing exercise intolerance, and a cycle of chronic pain and disability. 2
There is also growing evidence connecting hEDS with mental health conditions such as anxiety, depression, and ADHD. 17 While the exact mechanism linking hEDS with ADHD is unclear, one hypothesis is that chronic pain disrupts attention. 17 Anxiety in hEDS is likely multifactorial, potentially stemming from chronic pain and co-occurring autonomic nervous system dysfunction, which can mimic anxiety symptoms. 18 Furthermore, patients with EDS frequently experience anxiety and depression not only due to chronic pain but also from the stress of facing limited understanding from others regarding their physical restrictions and social challenges. 17
For individuals with hEDS, encounters with the healthcare system can be fraught with challenges. In a sample of 26 individuals with hEDS, 81% reported negative healthcare outcomes, often attributing these to clinicians’ limited knowledge about EDS. 19 Many participants described clinicians as disrespectful or unprofessional, and 85% indicated they avoided seeking medical care as a result. Such breakdowns in patient–provider communication may worsen the intersection of chronic pain and psychological distress. This issue may be intensified for TGD individuals, who experience higher rates of healthcare discrimination based on gender identity. 8
Mental health disparities are well documented in TGD populations compared to cisgender populations, a finding echoed in our study, where 81.4% of participants presented with anxiety, depression, or ADHD. 20 This rate aligns with previous studies on EDS in TGD populations, reporting psychiatric comorbidity rates of 86% and 89%.9,10 These mental health disparities are consistent with the minority stress model, which attributes psychological distress in transgender and gender-diverse patients not to gender identity itself but to experiences of discrimination and transphobia. 21 In addition, mental health assessments that are required for accessing gender-affirming care may contribute to an overrepresentation of psychiatric diagnoses within TGD populations. 22
Gender-affirming care and strong social support are correlated with improved mental health for TGD individuals. For instance, Olsavsky et al. found that gender-affirming hormonal therapy was associated with reduced anxiety symptoms in transgender adolescents, and family support was associated with fewer depressive symptoms and reduced nonsuicidal self-injury. 23 Similarly, Chelliah et al. found that transgender youth receiving gender-affirming hormone therapy experienced significant improvements in depression, anxiety, and overall psychosocial functioning after 1 year, with family acceptance further enhancing these outcomes. 24 These findings underscore the critical role of gender-affirming care and supportive family environments in promoting positive mental health outcomes for transgender youth, highlighting the need for accessible, affirming healthcare and social support systems.
Limitations
We conducted a retrospective chart review, thus data were limited to what was recorded in the electronic medical record. We could not verify how accurately EDS diagnostic criteria was followed. Furthermore, a retrospective review is unable to imply causality.
The patient population was predominantly white and non-Hispanic, which is not representative of the larger TGD population, but is representative of patients diagnosed with hEDS and our clinic sample broadly. The racial disparity observed in patients diagnosed with hEDS may be attributed to several factors, including differences in healthcare access, variations in clinical presentation, and potential biases within the healthcare system. These factors can lead to delayed or missed diagnoses in non-White populations, further exacerbating health inequities.
Additionally, our sample disproportionately represents nonbinary individuals compared to the general TGD population, with 55.9% of our sample being nonbinary versus 38% reported in the 2022 U.S. Trans Survey. Conversely, transgender women were underrepresented in our sample (13.6%) relative to the survey (35%). 8
This study did not include a formal calculation of sample size prior to data collection, as it was a retrospective chart review relying on available medical records. Consequently, the sample size was determined by the number of eligible patients within the defined study period, which may limit the statistical power and generalizability of the findings. Future studies could benefit from prospectively designed methodologies that incorporate sample size calculations to ensure robust statistical analysis.
Conclusions
This study highlights the prevalence of hEDS in a gender-affirming primary care setting, with 2.7% of patients over the age of 16 diagnosed with the condition. The findings reinforce the emerging recognition that hEDS may be both underreported in the general population and overrepresented within the transgender, nonbinary, and gender-diverse (TGD) community. In our sample of transgender, nonbinary, and gender-diverse patients with hEDS, we see individuals with intersecting vulnerabilities that can complicate healthcare access and strain patient–provider relationships. Future research could inform clinician education initiatives on EDS diagnosis and management and promote cultural humility when caring for TGD patients. Our findings underscore the compounded psychological and healthcare challenges faced by TGD patients with EDS, suggesting a need for holistic, intersectional approaches in both research and clinical practice.
Footnotes
Acknowledgements
None.
Author contributions
TS and SC made substantial contributions to the concept of the article, acquisition, analysis, and interpretation of data and drafted the article and approved the version to be published and agreed to be accountable for all aspects of the work. JL made substantial contributions to the interpretation of data for the article, revised it critically, approved the version to be published, and agreed to be accountable for all aspects of the work.
Consent to participate
The IRB granted a waiver of written informed consent under 45 CFR 46.116(f). Additionally, the waiver for parent/guardian permission was granted in accordance with 45 CFR §46.408(c) and 45 CFR §46.116(f). The waiver for minor assent was granted in accordance with 45 CFR §46.408(a) and 45 CFR §46.116(f).
Consent for publication
Not applicable.
Data availability
The data will not be shared due to concern for patient privacy in the context of a small sample size within a small population of transgender and gender diverse individuals with Ehlers–Danlos syndrome.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Partial funding for open access was provided by Tufts University Hirsh Health Sciences Library’s Open Access Fund.
Ethical considerations
Institutional review board approval was obtained from Tufts University School of Medicine (IRB STUDY00004950).
Informed consent
Informed consent was not sought for this study because it was waived by the relevant Institutional Review board (IRB STUDY00004950). In accordance with 45 CFR 46.116(f), the IRB granted a waiver of written informed consent. Additionally, the waiver for parent/guardian permission was granted in accordance with 45 CFR §46.408(c) and 45 CFR §46.116(f). The waiver for minor assent was granted in accordance with 45 CFR §46.408(a) and 45 CFR §46.116(f). It was waived because the study performed was a retrospective chart review that utilized de-identified data that did not require interactions with patients or participants and it qualified for a waiver of HIPAA Authorization.
Trial registration
Not applicable.