
Abstract
Objectives:
Female genital cutting is a genital operation for a nonmedical reason and involves the cutting away of a part or whole of the female external genitals. Postnatal women with genital cutting could be more vulnerable to circumcision-associated birth complications, and it is still a major health problem during childbirth and the postnatal period in Ethiopia. This study aimed to assess complications associated with female genital cutting among postnatal women in Chuko Primary Hospital, Sidama region, Southern Ethiopia.
Methods:
An institutional-based quantitative cross-sectional study design was conducted from 01 May 2021 to 15 June 2021. A systematic random sampling technique was used to select study participants. Data were collected by using a structured pretested questionnaire and reviewing medical records. The data were analyzed using SPSS version 23.0. Logistic regression analysis was computed to identify birth complications associated with female genital cutting from independent variables, and significance was declared at p < 0.05 with 95% CI.
Results:
The proportion of female genital cutting among the participants was 76.8% (95% confidence interval: 71.1, 81.2). Prolonged labor and birth asphyxia were statistically significant female genital cutting-associated birth complications.
Conclusion:
This study revealed a high proportion of complications associated with female genital cutting. Birth complications such as prolonged labor and birth asphyxia have a statistically significant association with it. Illiteracy and early marriage were the predominant reasons for female genital cutting. Therefore, healthcare providers should educate the rural communities to prevent early marriage and female genital cutting to prevent its complications.
Introduction
Female genital cutting/circumcision (FGC/C) is defined as a surgical procedure that manipulates young girls’ and women’s external genitalia for cultural or nontherapeutic reasons.1,2 According to the World Health Organization (WHO), FGC/C is classified into different types. It involves clitoridectomy, excision, infibulation, pricking, piercing, incising, scraping, and cauterizing the genital area. 3
FGC can be performed during infancy, childhood, adolescence, at the time of marriage, or during the first pregnancy. 4 It is performed for cultural purposes to preserve virginity, marriageability, and religious acceptance.5–7 It is often considered as a harmful traditional practice detrimental to the health of the female gender and a form of discrimination or violence against girls and women. 8
According to the WHO report, more than 200 million women’s genitals are mutilated in Africa, Asia, and the Middle East. 3 The United Nations (UN) report revealed that 80% of reported cases are found in Africa. 9 Studies showed that in Africa one to two babies die per 100 deliveries due to FGC-associated birth complications.10,11 In Ethiopia’s context, a systematic review and meta-analysis studies have shown high prevalence of FGC/C between 77% and 87.5%.12–14
Women with FGC/C were confronted with mechanical obstruction, prolonged labor, fetal distress, perianal tear, wound infection, and fistula during childbirth.11,15–17 Postnatal women with FGM could be more vulnerable to circumcision-associated birth complications, and it is still a major health problem during childbirth and the postnatal period in Ethiopia. Excess vaginal bleeding, wound infection, and neonatal distress have been commonly reported in the course of postnatal period, which may also cause maternal and neonatal morbidity and mortality.10,16 Even though, highly prevalent FGC is in the study area, reliable evidence of the associated birth complications among postnatal women is rare. Therefore, the purposes of this study were to assess complications associated with FGC among postnatal women and establish baseline information for the future implementation of any plan of action.
Methods and materials
Study area and study period
Aleta Chuko is one of the woredas in the Sidama region of Ethiopia. Aleta Chuko is bordered on the south by Dara, on the southwest by Oromia region, on the west by Loka Abaya on the north by Dale, and on the east by Aleta Wendo. The administrative center is Chuko, a town which is located 315 km from Addis Ababa, the capital city of Ethiopia, and 76 km from Hawassa, the capital city of the Sidama region. In a total population of 22,953, 13,788 were female and 5701 were reproductive-age women 18 served by hospitals per year. The pooled prevalence range of FGM in Ethiopia was 74%–85%. 11
Study design
An institutional-based quantitative cross-sectional study design was conducted.
Population
Source of population: All postnatal (15–49 years old) women who registered in the labor and delivery logbook at Chuko Primary Hospital during the study period were the source of population.
Inclusion and exclusion criteria
Inclusion criteria: All sampled postnatal (15–49 years old) women who gave birth in Chuko Primary Hospital were included in the study.
Exclusion criteria: Critically ill and involuntary women during the data collection were excluded from the study.
Sample size determination and sampling technique
The minimum sample size required for the study was determined by using a single population proportion formula
The lists of postnatal women were obtained from the postnatal registration logbook. From 301 eligible women, 250 study participants were selected using a systematic random sampling technique. The skipping interval (K-value) was determined by dividing the number of units in the population (N = 381) by the desired sample size (n = 250), which was 1.524 ˷ 2. Then, the first respondent was selected by lottery method, and subsequent respondents were selected by every other interval.
Data collection procedures (Instrument, Personnel, Data Quality Control)
Data collection instruments: The data collection tool was prepared in English after reviewing related literature and then translated into the Amharic language (16, 17). The questionnaire consisted of sociodemographic variables, obstetrics characteristics, and postnatal complications. Data were collected using a pretested structured interviewer-administered questionnaire from patients and patients’ cards were also reviewed (Annex 1). To assure the quality of data: Two experienced graduate midwives were trained for data collection and two graduate midwives were assigned as supervisors under the supervision of the principal investigator. The training was provided to data collectors and supervisors regarding data collection techniques, data validity, and ethical considerations. The prepared questionnaire was pretested on 5% (n = 5) of the sample size and adjustments were made based on the findings. Each questionnaire was coded with a unique identification number. Filled questionnaires were checked daily for completeness and consistency. The reliability of the questionnaire was checked by Cronbach’s alpha value, which was 0.79. 19
Operational definitions
FGC/C: In this study, a woman who has any surgical modification involving partial or total removal of the external genitalia was considered. Types of FGC/C: No FGM: no evidence of any genital mutilation; FGM I: excision of the prepuce, with or without excision of part or the entire clitoris; FGM II: excision of the clitoris with partial or total removal of the labia minora; and FGM III: excision of part or all of the external genitalia and stitching or narrowing of the vaginal opening (infibulation). 1
Postpartum hemorrhage (PPH): A woman who had blood loss of ⩾500 ml following vaginal childbirth or ⩾1000 ml following cesarean childbirth was considered as postpartum hemorrhage. 20 Episiotomy: An episiotomy is a minor incision made during childbirth to widen the opening of the vagina. 21 Apgar score: The Apgar score is a test to assess newborns soon after birth. A score of 7–10 after 5 min is “normal.” A score below 6 is considered “abnormal.” 22
Statistical analysis
Data entry, cleaning, and screening were done exclusively by the principal investigator and coinvestigators. The edited and cleaned data were entered into EpiData version 3.1 and exported to SPSS version 23 for analysis. Descriptive statistics were performed using frequency tables, measures of central tendency, and cross-tabulation. Logistic regression analysis was computed to identify complications associated with FCG. The fitness of the model was checked by the Hosmer–Lemeshow tests. 23 Variables with a p-value of less than 0.25 in the bivariate logistic regression analysis were selected for multivariable logistic regression analysis. Finally, significance was declared at p < 0.05 with 95% CI.
Results
Sociodemographic characteristics
A total of 250 participants were involved in the study with a response rate of 100%. The mean age of participants was 22.48 ± 5.03 years and 43.6% (n = 109) of participants were aged between 25 and 29 years. Of the study participants, 69.6% (n = 174) were from rural areas. Four-fifth, 82.8% (n = 207) of study participants, were married. More than half, 52.0% (n = 130) of the study participants, were illiterate. One-third, 36.7% (n = 99) of the study participants, were housewives. Nearly half, 47.6% (n = 119) of the study participants, had 500–1000 EB on average. Almost two-thirds, 62.2% (n = 168) of the study participants, had 1–3 family members on average (Table 1).
Sociodemographic characteristics of study participants in Chuko Primary Hospital, Sidama region, Southern Ethiopia (n = 250).

EB: Ethiopian Birr.
Obstetric characteristics of the study participants
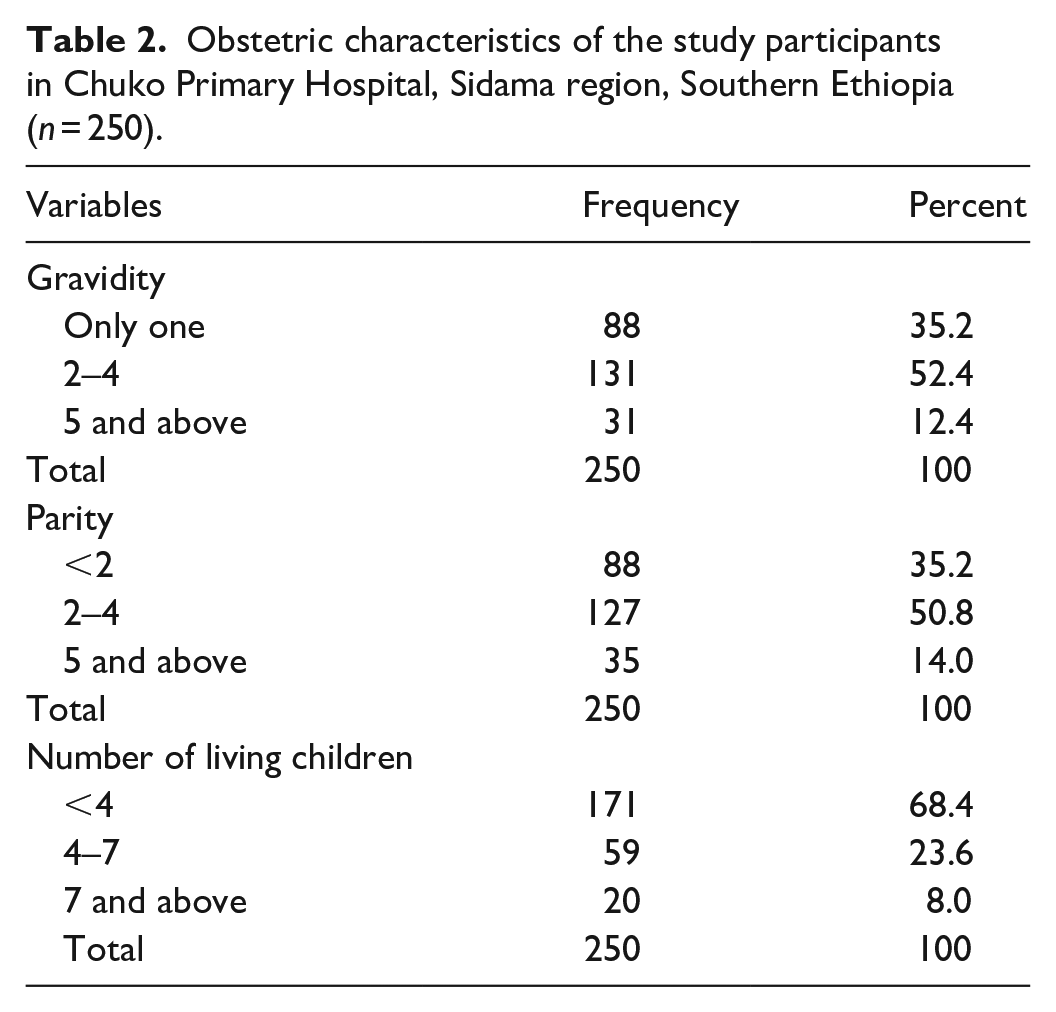
Among the study participants, 50.8% (n = 127) had Gravida two to four on average, followed by Gravida 1 in 35.2% (n = 88) (Table 2).
Obstetric characteristics of the study participants in Chuko Primary Hospital, Sidama region, Southern Ethiopia (n = 250).
Postnatal maternal and newborn complications
Among the study participants, 58.0% (n = 145) had an episiotomy, 34% (n = 85) had prolonged labor, 3.2% (n = 8) had perinea infection, 7.2% (n = 18) had given birth by cesarean section, and 6.8% (n = 16) had PPH during childbirth. More than two-fifths, 42% (n = 105) of the respondents’ babies developed neonatal complications. Asphyxia (37.6%, n = 94) and low birth weight (13.6%, n = 34) were commonly observed neonatal complications (Table 3).
Female genital cutting and maternal and newborn complications of the study participants in Chuko Primary Hospital, Sidama region, Southern Ethiopia (n = 250).

Female genital cutting
Of the study participants, 76.8% (n = 152) had been circumcised (FCG). Among circumcised women, 57.8% (n = 111) had type I, 33.9% (n = 65) type II, and 8.3% (n = 16) type III. All circumcision procedure was carried out with the aid of a traditional birth attendant (TBA). Among women who had FCG, 58.8% (n = 147) were circumcised in less than 10 years (Figure 1).

Magnitudes of female genital cutting of the study participants in Chuko Primary Hospital, Sidama region, Southern Ethiopia (n = 250).
Complications associated with FCG
On bivariate analysis, an episiotomy, prolonged labor, and birth asphyxia were candidates for multivariate analysis. On multivariate analysis, prolonged labor and birth asphyxia were statistically significant in the final model (Table 4).
Bivariate analysis of the female genital cutting and associated complications among postnatal women in Chuko Primary Hospital, Sidama region, Southern Ethiopia (n = 250).

COR: Crude Odd Ratio; AOR: Adjusted Odd Ratio. Significant at *p-value <0.05, and **p-value <0.01.
This study revealed that the odds of having birth asphyxia among mothers who had FCG were two times (AOR = 1.6; 95% CI: 0.03, 0.82) more likely compared with those who had no FGC. On the other hand, odds of having prolonged labor among mothers who had FCG were two times (AOR = 1.52; 95% CI: 0.03, 0.82) more likely compared with those who had no FGC.
Discussions
This study was intended to assess the complications associated with FGC among postnatal women.
In this study, the proportion of FGC among postnatal women was 192 (76.8%) higher than in the study conducted in the Keras district and in Sierra Leone.13,24 However, it was lower than the study conducted in the Hadiya zone, Wolayita zone, Jigjiga district, and systematic review and meta-analysis.12,13,19,25,26 The reason behind this difference may be the area where the study was conducted and the sample size. This study was carried out in a rural primary hospital with a small sample size. Another reason might be the educational status of the respondents. In this study more than half of the respondents were illiterates.
In the current study, women with FGC/C were more likely to have episiotomy when compared with uncircumcised women. The finding of this study was consistent with studies carried out in the Hadiya zone and a short literature review in which women who had circumcision were more likely to have an episiotomy during childbirth when compared with uncircumcised women.19,27 The possible reason behind this difference may be tight perineum due to scar of genital cutting among respondents.
This study also showed that women who had FGC/circumcision were more likely to have prolonged labor when compared with uncircumcised women. This result is comparable with a study conducted in the Hadiya zone, Kersa district, the Bale zone, and a systematic review and meta-analysis. 11,15,19,24 The possible reason behind this difference may be the age of the respondents. In this study, nearly half of the respondents were below 25 years. The other reason may be a tight perineum scar; giving birth at an early age and circumcision scar could decrease the elasticity of the perineum.
This study also revealed that newborn babies from FGC/circumcised mothers were more likely to have birth asphyxia when compared with the newborn baby from uncircumcised mothers. This result is comparable with the study conducted in the Bale zone and a short literature review.15,27 This reflects that circumcision scar decrease the elasticity of the perineum which increases the probability of birth asphyxia for newborn babies. The difference might be due to sampling size and study area; this study was carried out in a rural primary hospital with a small sample size. In rural areas, the acceptance of female genital cutting is high when compared with the urban community due to low awareness and sociocultural effects.
This study revealed that FGC is typically associated with early marriage among respondents which might be related to the educational status of women. Uneducated women were more likely to have FGC/circumcision and early marriage when compared with their educated counterparts. FGC/circumcision has immediate and long-term effects on women and newborn babies. Those effects could be physical like the formation of a keloid scar, infection, and hemorrhage as well as psychosocial. 28
Strengths and limitations of the study
Strengths of the study
The study was carried out in the primary hospital in a rural area.
Data collectors were experts who had been on their activities in the study place which could appreciably minimize errors in data collection.
Bivariate logistic regression analyses were used to see the statistically significant association of an independent variable over the outcome variable.
Limitations of the study
This study employed quantitative study design, so some imperative qualitative data about FGC were not explored deeply.
The nature of the cross-sectional study did not show cause and effect relations among variables.
Conclusion
This study revealed a high proportion of complications associated with FGC. Birth complications such as prolonged labor and asphyxia have a statistically significant association with FGC. Since, the proportion of FGC and early marriage is not prevented, it can be a cause of maternal and newborn complications during the postnatal period. Illiteracy and early marriage had been the predominant reasons for FGC. Therefore, healthcare providers should educate the rural communities to stop early marriage and FCG to prevent its complications.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221144243 – Supplemental material for Assessment of complications associated with female genital cutting among postnatal women in Chuko Primary Hospital, Sidama region, Southern Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221144243 for Assessment of complications associated with female genital cutting among postnatal women in Chuko Primary Hospital, Sidama region, Southern Ethiopia by Yirgalem Yosef, Abebe Borsamo and Seblework Abeje in SAGE Open Medicine
Footnotes
Acknowledgements
We Dilla University, Aleta Chuko woreda health bureau, and Chuko Primary Hospital are the institutions that need to be indispensably recognized for their role in accomplishment of this research. Midwives in Chuko Hospital and colleagues have participated in the overall process. Finally, sincere appreciation and grateful acknowledgement goes to the respondents and data collectors.
Author contributions
All authors have substantial contributions to conception; design; acquisition, analysis, and interpretation of data; drafting and revising of the article critically, for important intellectual content; and the approval of the final version of this article.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available as consent for the sharing of this data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical clearance was obtained from the institutional review board of Dilla University with the reference number M/S/963/2012.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
A permission letter was obtained from Chuko Primary Hospital authorities. Participation in the study was voluntary and written informed consent was obtained from mothers, and for those below 18 years old, was obtained from their parents. All the information taken from the study participants was kept confidential.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.