
Abstract
Objectives:
To identify risk factors for loss to follow-up in periodic intravitreal anti-vascular endothelial growth factor injections for the treatment patients with diabetic macular edema, subretinal neovascularization, age-related macular degeneration, and retinal vein occlusion in a single eye center in São Paulo, Brazil.
Methods:
This was a retrospective longitudinal study that gathered information from 992 patients who required intravitreal anti-vascular endothelial growth factor drugs over 6 months. The authors included age, eye disease, laterality, monthly income, distance, and payment mode as risk factors.
Results:
Two hundred and seventy patients (29.93%) were lost to follow-up. Multivariate analysis showed age, monthly income, eye involvement, and type of medical assistance independently associated with loss to follow-up. The odds of loss to follow-up were greater among older patients than those less than 50 years (reference), p < 0.001. The odds of loss to follow-up were greater among patients who received unilateral treatment than those who received bilateral injections (p = 0.013). Concerning gross monthly income, there were no differences in the odds of the four salary strata; the data also indicate an absence of difference in the three strata of patients’ distance to the clinic. Considering the diagnosis, only age-related macular degeneration showed greater odds of loss to follow-up (p = 0.016). Finally, the data suggest greater odds of loss to follow-up in private patients than in those on a health care plan (p < 0.001).
Conclusion:
Loss to follow-up is paramount because many patients may remain unassisted concerning their eye diseases. Identifying the risk factors is crucial to enforcing measures to increase adherence and the long-term success of the treatment.
Keywords
Introduction
Intravitreal injection (IVI) is the most performed ophthalmologic procedure worldwide. 1 Considering its effectiveness, the use of vascular endothelial growth factor (VEGF) injections for the treatment of retinal vasculopathy, such as age-related macular degeneration (ARMD), central retinal vein occlusion, diabetic retinopathy, has grown substantially.1–3 In the United States, there was an increase from 2.943 procedures in 2000 to 2.619.950 in 2014. Thus, there was an increase in the volume of IVIs in retinal pathologies, 3 replacing expectant management and improving the quality of life.3,4
Intravitreal drug administration allows for better absorption, 5 following protocols described in the literature, such as fixed monthly, “pro re nata,” and “treat-and-extend” protocols.2,5–7 The number of injections depends on the disease and individual patient response, but follow-up visits after treatment are imperative to optimize visual outcomes.6–8 Most papers on this issue come from America and Europe; there is no similar study in Brazil, where 30.8% of the patients present poor adherence to pharmacological treatment. 9
When patients are lost to follow-up, real-world outcomes are of great concern because they cannot always return at recommended intervals.10–12 Patient attrition is not unusual in clinical practice. 10 Therefore, our study aimed to determine loss to follow-up (LTFU) rates among patients who received IVIs and investigate the association of potential risk factors. We analyzed gender, age, distance from the patient’s home to the clinic, patient’s monthly income (BRL), laterality of the treatment (one eye or both), and treatment reimbursement as risk factors for LTFU.
Materials and methods
Study design
This was a retrospective longitudinal study using data from one eye clinic in Brazil. We gathered information on 992 eyes of 992 patients who required intravitreal anti-VEGF drugs from 8 January 2020, to 30 September 2021.
The facility
HCLOE stands for Hospital de Clinicas Oftalmológicas Especializadas or Hospital of Ophthalmological Specialized Clinics and includes four units in urban places in São Paulo. There are 27 clinical offices and a monthly mean of 8.800 appointments. The surgical procedure only occurs in one of the four units located in a central suburb of the city. The satisfaction grade of the patients is high (NPS, or Net Promoter Score average > 8), which minimizes the possibility of losing patients to competitors nearby. 13
Eligibility
The authors included patients with diabetic macular edema (DME), subretinal neovascularization (SRNV), age-related macular degeneration (ARMD) and retinal vein occlusion (RVO) as the primary diagnoses, which required vitreous injections. We included patients aged 18 years or older who had undergone at least one IVI at our facility. We excluded patients diagnosed with polypoidal choroidal vasculopathy, macular telangiectasia, uveitis, central serous chorioretinopathy, coats, and best syndromes because of the low frequency of such cases among our sample. Finally, we excluded patients for whom information was incomplete and those who submitted to glaucoma or retina surgery or were deceased during the study (confirmed through regular telephone contact by the staff).
The first eye that entered the study, the second eye would go automatically to the bilateral group.
Main outcomes
After anti-VEGF injections, the primary outcome was LTFU rates. The authors defined the LTFU as no succeeding follow-up visit within 12 months after one or more injections.
Risk factors
The staff aimed to detect the consequence of gender, age (in years), distance from the patients’ home to the clinic, patient’s monthly income (BRL), laterality of the treatment (one eye or both), and the treatment reimbursement in the rate of LTFU.
Brazil has three reimbursement categories: government provision (also called public health system), health care plan (sometimes referred to as health insurance, with the same meaning), or payment from patients’ pockets (referred to here as private). In our study, the patients come from the two last categories; the clinic does not provide public health system. Therefore, concerning the reimbursement categories, we compare only those patients from health insurance to those who pay for the procedure from their pocket.
The authors arranged to not include race owing to the difficulty of unequivocally classifying all the races in our country.
Monthly income groups
The authors leaned on the site https://www.salario.com.br to correlate the patients’ professions with their monthly incomes. The site is a free Brazilian portal from the General Office of Social Welfare in the Ministry of Welfare. The study protocol assigned a monthly welfare of BRL 2280.16 to retired patients, which corresponds to the mean in the 2020 statistical report of social security benefits for urban workers (http://sa.previdencia.gov.br/site/2020/04/Beps022020_trab_Final_portal.pdf). Students and nondefined professions received an arbitrary monthly value of BRL 1000.00. BRL is the Brazilian currency, called the “Brazilian Real”; 1 US Dollar approximately equals 4.77 BRL by June 2023.
Distance from the patient’s house to the clinic
A computer programmer depended on the Google Distance Matrix API (application programming interface) geotagging to determine the distance from the patient’s house to the clinic, located on a unique site in the Bela Vista Suburb in São Paulo. The programmer had the addresses and converted them into latitude and longitude in geotagging position coordinates. Those positions fed the app, which returned the distance, from the patient’s house to the clinic, in kilometers.
Ethics
The mainboard of Opty Group—HCLOE—Oftalmologia especializada endorsed the study, which was the condition of complete anonymity of all patients. For this reason, the patients remained anonymous during the study’s collection, analysis, and writing. The data were gathered and remained in an encrypted file in one unique computer (Marcos Balbino). The research methods fulfilled the Helsinki Declaration. The study did not demand informed consent owing to its retrospective design and noninterventional review of medical records.
Statistical analysis
The null hypothesis assumes the same rate of LTFU concerning all the risk variables; the alternative hypothesis sets to detect a difference in the rates, assuming the variable groups, under the threshold of p < 0.05. The authors expressed the number and percentage of LTFU patients. Continuous variables were scrutinized for skewness and kurtosis to define their distribution.
We estimated the number of charts we needed to gather as a retrospective study. Based on the previous reports Gao et al., 1 we expected a similar dropout rate (0.25). The staff ran a McNemar test of proportions inequality, setting an odds ratio threshold of 1.35, with an alpha of 0.05 and a power of 0.95. We decided to set a proportion of 0.75 (0.25 LTFU, as described by others). The calculated total sample size was 786; we included 15% more to cover those with incomplete data archives.
The study design assumes the report of the odds ratio and the respective 95% confidence interval. The first part of the comparison includes the Chi-squared test for 2 × 2 tables, involving the LTFU as a dependent variable and the risk factors as a covariable. Then, the potential risk factors for LTFU are evaluated using a univariate logistic regression, using the two-tailed p values. Predictive margins and marginal effects are plotted with 95% confidence intervals to show prediction tables. Multivariate analysis of variance (MANOVA) is used to measure the effect of multiple independent variables on LTFU. The multivariate model includes variables with statistical significance at univariate tests. The authors relied on Stata 13.0 (StataCorp. 2013 Stata Statistical Software: Release 13; StataCorp LP, College Station, TX, USA).
Results
Nine hundred and two patients met the initial criteria for inclusion. The described criteria excluded 54 patients. Figure 1 describes the selection criterion diagram. Among the 902 patients, 270 (29.93%) were LTFU. Table 1 shows the demographics of the patients and the respective comparison of the categorical variables.

The flowchart for inclusion of the patients.
Patient demographics of the study.

BRL: Brazilian Real (1 US Dollar equals 4,77 BRL, on 22 June 2023).
Indicates the p-value in the rejection region of the null hypothesis.
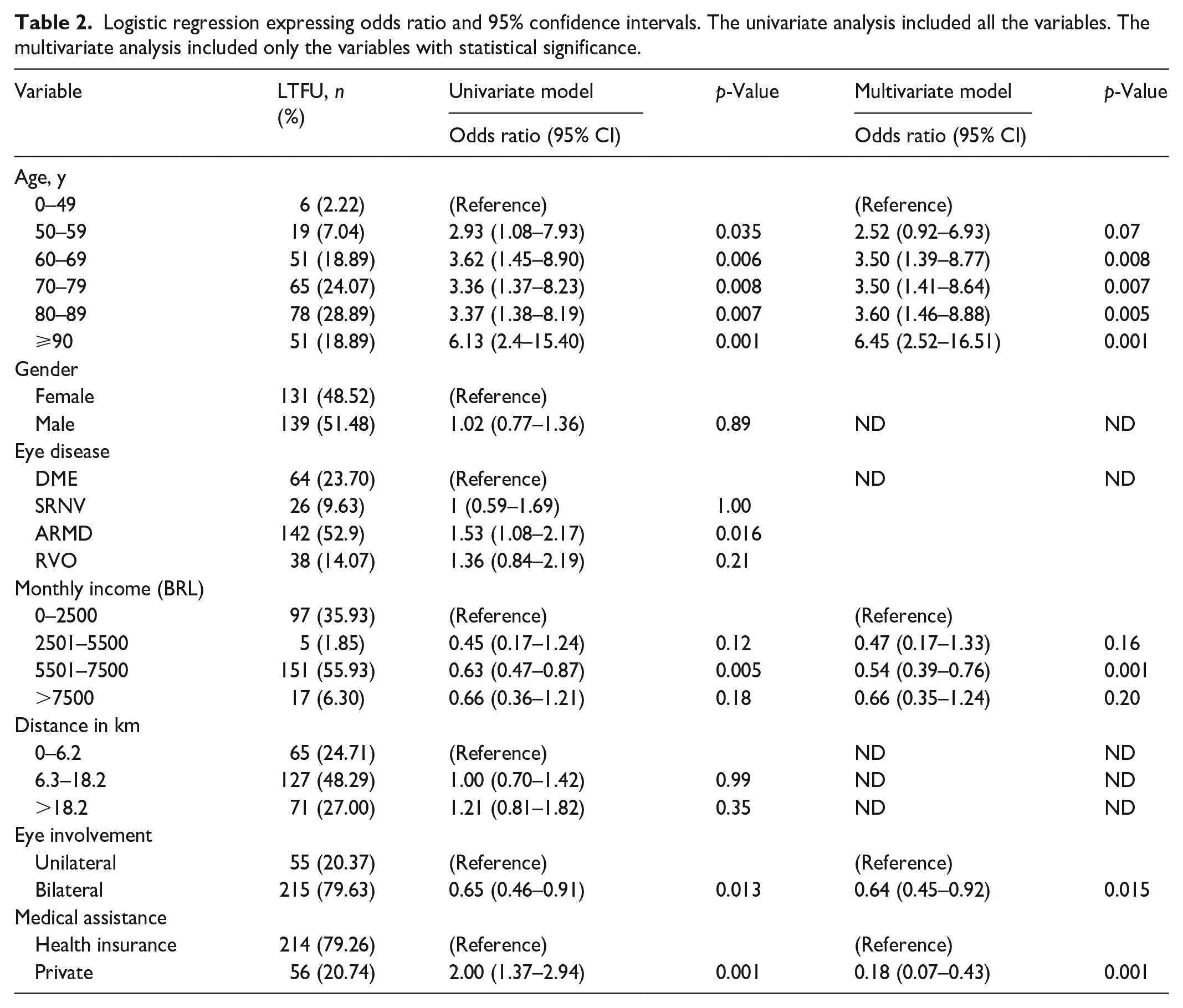
The odds of LTFU were greater among patients 50–59 years of age (OR 2.93, 95% CI: 1.08–7.93), p = 0.04, among those 60–69 years of age (OR 3.62, 95% CI: 1.45–8.90), p = 0.006, among those 70–79 (OR 3.36, 95% CI: 1.37–8.23), p = 0.008, among those 80–89 (OR 3.37, 95% CI: 1.38–8.19), p = 0.007 and more than 90 years of age (OR 6.13, 95% CI: 2.40–15.40), p = 0.001, compared with patients younger than 50 years old.
The odds of LTFU were greater among patients who received unilateral treatment (OR 1.54, 95% CI: 1.09–2.18), p = 0.013, than among those who received bilateral injections. Concerning monthly gross income, odds of LTFU were (OR 1.52, 95% CI: 0.82–2.81), p = 0.18 for the range BRL $ 0–2500.00, (OR 0.68, 95% CI: 0.22–2.11), p = 0.51 for the range BRL $ 2501.00–5500.00 and (OR 0.97, 95% CI: 0.54–1.75), and p = 0.91 for the range BRL $ 5501.00–7500.00, compared to the range of BRL $ >7500.00. The odds for LTFU, concerning the distance from their home to the clinic, were (OR 0.99, 95% CI: 0.70–1.42), p = 0.99, for those living from 6.3 to 18.2 km and (OR 1.21, 95% CI: 0.81–1.82), p = 0.35 and for those living more than 18.2 km, compared to those living from 0 to 6.2 km. The odds for LTFU were greater among private patients (OR 2.00, 95% CI: 1.36–2.95), p = 0.0003, than those on a health insurance. There was no difference concerning sex in the odds ratio for LTFU (OR 1.02, 95% CI: 0.77–1.36), p = 0.89, for men compared to women.
Considering the four primary diagnoses, DME, SRNV, ARMD, and RVO, only ARMD showed a higher OR for LTFU (OR 1.53, 95% CI: 1.08–2.17), p = 0.016, compared to patients with DME, the reference disease group.
Multivariate analysis showed age, monthly income, eye involvement, and type of medical assistance independently associated with LTFU (Table 2).
Logistic regression expressing odds ratio and 95% confidence intervals. The univariate analysis included all the variables. The multivariate analysis included only the variables with statistical significance.
Probability for LTFU
The authors stratified the impact of the type of assistance (health insurance versus private procedure) on the variables such as age, eye disease, monthly income, distance to the clinic, and eye involvement (unilateral versus bilateral). The probability of LTFU, related to several variables, is illustrated in Table 3. Private assistance shows a higher probability of LTFU, mainly in those older than 90 years old (0.56), those with the lower monthly income strata (0.53), those living farthest from the clinic (0.47), and those in unilateral treatment (0.47).
Logistic regression resulted in predictive margins and means. The table shows the predictive probability of LTFU for the variables in all the patients (global, first column). The two other columns show the probability stratified in two categories, according to the medical assistance (health insurance and private) for the variables.

Discussion
Among the 902 remaining patients, 270 (29.93%) were lost to follow-up after 12 months, corroborating numerous other studies’ findings.1,6,10 We uncovered differences in all age levels, laterality of the treatment (one eye), payment mode (private), and monthly income (second salary strata). Anthony Obeid et al. 8 showed that 22.2% of patients with ARMD receiving IVIs did not adhere to the advised follow-up schedule. In a cross-sectional study by Xinxiao Gao et al., 1 one in four patients (25%) with nonproliferative diabetic retinopathy who had DME was LTFU, which was much higher than expected. The frequency of LTFU is highly concerning owing to the importance of ongoing treatment in these patients to optimize outcomes. 14 Abdelmotaal et al. 7 proliferative demonstrated an overall LTFU rate of 16.3% over approximately 5 years in patients who received panretinal photocoagulation and/or IVIs anti-VEGF to treat proliferative diabetic retinopathy.
The present study identified several patient characteristics associated with LTFU. A notable discovery was the disparity in LTFU rates considering the laterality of the treatment, with the highest rate of LTFU in unilateral procedures. In addition, we evaluated laterality combined with age strata, and unilateral eye treatment resulted in a higher risk to LTFU in all age strata. Moreover, the LTFU has grown from 36.36% (bilateral) to 47.62% (unilateral) among patients above 90 years of age. Concerning laterality and the type of medical assistance reimbursement (private vs health insurance), again, those patients who received bilateral injections had lower LTFU rates in both groups of medical assistance. Obeid et al. 8 found that unilateral eye disease was a risk factor associated with LTFU among patients with neovascular age-related macular degeneration. They suggest that patients who receive bilateral injections have lower LTFU rates, which may be related to an association between more severe disease and stricter follow-up. Droege et al. 15 showed from the patients’ point of view that anxiety of a negative examination result was more pronounced than fear of intraocular injections, which would be an argument for continuous follow-up.2,5,6
The age variable, singly, showed variation among its strata. The odds of LTFU from patients between 80 and 85 were not more significant than those of patients younger than 80. However, the odds of LTFU were more significant in patients 85–90 and older than 90 compared to patients 80 or younger. A possible explanation for this occurrence is that patients older than 85 years have at least two chronic diseases,15–18 and comorbid conditions can severely limit an individual’s ability to perform daily activities unassisted.19–24 Younger age has lower follow-up rates. 25 This may reflect more restrictive employment schedules or a lower prioritization of seeking health care among patients in this demographic.25,26 In addition, the contrast between different age groups might be confounded by insurance coverage and deductible plans, as Mohammadi et al. 21 explained. According to some studies, younger patients are less likely to have insurance than older patients.27–30 In our sample, we compared the age and monthly payment groups, and we see that private patients demonstrate a more significant disparity in LTFU rates by age.
Our results also suggest an association between higher rates of LTFU and private payment mode. Patients’ high lifetime treatment cost is also a concern, 16 as evidenced by the significant positive correlation between treatment unaffordability and the number of IVIs.15–18 Although insured patients are sometimes responsible for only a fraction of this cost, 30 the associated payers can be difficult for low-income patients.13,30 Self-pay patients and those with high-deductible plans often bear an even more significant cost duty, 2 especially when requiring frequent return visits and injections.10,11 Low socioeconomic status may influence patient behavior and health26–28,31 and increase the risk of not receiving preventative vision care, possibly due to the difficulty of affording out-of-pocket costs. 31 Our study considered four monthly salary groups (BRL) inversely associated with LTFU. The group with a monthly salary 0–2500.00 is associated with high LTFU. When we plotted against the type of medical care, the private payment mode seems to be associated with a higher probability of LTFU in all salary groups than the insurance modality. Additionally, the lower salary level defines the highest LTFU rates in both payment categories. A possible explanation is that unemployed patients with little or no access to costs.13,30 The price of the drugs is so high that there is no difference in LTFU comparing salaries strata (only the lowest grade did); however, private patients (which means those who will pay from their pocket) will feel the skyrocketing prices regarding the salary strata.
The distance did not seem to influence the loss of follow-up and is not associated with high LTFU. This is an exciting finding in our analysis because another study showed an increase in LTFU as the distance to the clinic increased.1,2,5,6 In the study by Boulanger-Scemama et al., 19 distance also appeared to play a significant role in determining LTFU, with 51.7% of the patients who were LTFU identifying distance as the primary cause of their noncompliance. Obeid et al. 8 showed that medicare beneficiaries who lived more than 20 miles from their ophthalmologist were 33% less likely to receive regular eye examinations within four consecutive 15-month periods than were patients who lived less than 20 miles from the ophthalmologist. 6 When we compared the three home-to-clinic distance ranges against the type of medical care in our study, there was a higher LTFU in the private group. A possible explanation for this occurrence is that patients with health insurance have lower treatment costs with injections27–31 even with more distance. The insured patients are sometimes responsible for only a fraction of this cost27–30; therefore, the LTFU is lower in all distance classes than in private groups.
Considering the possibility of LTFU among the four primary diseases, there was a high LTFU in the ARMD group. It is the leading cause of irreversible vision loss in the developed world among people over 50 years of age, 24 and its prevalence is steadily rising owing to our aging society.24–26,31 Nevertheless, increasing age with ARMD could increase LTFU rates because older patients have multimorbidity and poor independence,19–24 as we described earlier. During their treatment, patients’ major problem was traveling to and from the hospital,29,30 and most usually required an escort, 21 involving family members or friends. 29 In addition, ARMD can evolve into severe forms with poor visual outcomes.2,6–8 Droege et al. 15 showed that 7 out of 95 patients did not attend further visits because of a loss of motivation; this group had a lower visual acuity outcome than patients who persisted with treatment. Boulanger-Scemama et al. 19 reported similar results of subjective dissatisfaction, with the benefits of anti-VEGF therapy being one of the reasons cited for discontinuation during follow-up, with poor visual outcomes observed during the first year.25,27
Brazil is the 12th largest economy globally; however, it still suffers from fundamental health issues. Some indicators rival the ones from developed countries, such as the increase in cancer, diabetes, and cardiovascular diseases. The Brazilian Ministry of Health, in 2019, has described an expansion in diabetes (7.4% of the population), arterial hypertension (24.5%), and obesity (20.3%). It is estimated that 24%–39% of all Brazilian people with diabetes have retinopathy, with 2 million cases in 2021 (Brazilian Government Portal, www.gov.br). Gao et al. 1 remarked a worldwide prevalence of diabetic retinopathy as far as 127 million, in 2010. The adherence to the anti-VGEF therapy in Gao’s paper is similar to the adherence we described in the present paper.
The high cost of anti-VGF drugs and the crowded hospitals from the public health system (government-funded) may explain our findings concerning LTFU. The majority of the patients of our clinic rely on health insurance. Therefore, the distance from the clinic to their homes becomes less important; what matters is to take advantage of the treatment. The salary ranges did not impact LTFU; however, private patients are at risk of LTFU in all salary strata. Finally, age risk to LTFU follows the standard of developed countries, where the economics and infrastructure influence less on this variable.
It is reasonable to address the present study’s pitfalls. The salary groups obtained from a national database repository may not reflect our actual reality. There is the possibility of overestimating the salaries in professional strata or those on welfare benefits. As we mentioned before, our group of retired patients may not represent the high welfare strata. Therefore, we could have highlighted differences where we did not, as we noticed no significant discrepancy in odds regarding salary groups. Economic reasons may represent an undercover variable regarding the distance from the patients to the clinic. Even patients at more significant distances feel compelled to continue their treatment. Again, it could explain the absence of difference in the odds related to the distance.
Our study revealed that 270 patients failed to complete their 1-year follow-up at our clinic out of 902 individuals. Identifying factors correlated with LTFU can encourage the development of targeted interventions to reduce this detrimental event.6,21–24 It is paramount to improve adherence by supplying patients with comprehensive details about the benefits of intravitreous injection and the importance of recurring long-term follow-up visits for preserving visual improvement.23–31
Conclusion
The high cost of anti-VGF drugs and the crowded hospitals from the public health system (government-funded) may explain our findings concerning LTFU. The majority of the patients of our clinic rely on health insurance, and private patients are at risk of LTFU in all salary strata. The distance to the clinic and the salary strata did not interfere with the dropout rates. Finally, the age risk of LTFU follows the standard of developed countries.
The present paper tries to show risk factors for LTFU, for relevant retina diseases, in a large and peculiar country. Healthcare professionals must seek treatment adherence at all costs; therefore, spreading such knowledge and keeping the research on track is vital.
Footnotes
Appendix 1.
Appendix 2
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.