
Abstract
Objectives:
Malaria in pregnancy is associated with adverse pregnancy outcomes including maternal anaemia and low birthweight. Uptake of preventive interventions is sub-optimal in sub-Saharan Africa including Ghana. Understanding local-level factors that influence uptake of these interventions can enhance control. The study assessed uptake of intermittent preventive treatment of malaria during pregnancy using sulphadoxine-pyrimethamine (IPTp-SP) and insecticide-treated net (ITN) use, their determinants and effects on pregnancy outcomes.
Methods:
A cross-sectional study involving 349 post-partum women was conducted from 25 August 2022 to 9 October 2022 at the Ho Teaching Hospital. A structured questionnaire was used to collect data on participant socio-demographics, ITN use, number of doses of sulphadoxine-pyrimethamine received, knowledge of malaria in pregnancy, haemoglobin levels and birth weight among others. Summary statistics were reported as frequencies, percentages and means. Associations between exposure and outcome variables were assessed using logistic regression methods and odds ratios reported with 95% confidence intervals. Statistical significance was concluded at p < 0.05.
Results:
More than 80% (291) of respondents received ⩾3 doses of intermittent preventive treatment using sulphadoxine-pyrimethamine and 64.8% (226) slept under ITNs the night before the survey. Age >25 years, employment, good knowledge of malaria in pregnancy, parity ⩾2 and initiating antenatal care visits in the first trimester facilitated the uptake of these interventions. Receiving ⩾3 doses of sulphadoxine-pyrimethamine was associated with having normal-weight babies (adjusted odds ratio 2.80, 95% CI: 1.07, 7.34; p = 0.036) while ITN use was associated with having term babies (adjusted odds ratio 2.72, 95% CI: 1.24, 5.90; p = 0.013) and normal maternal haemoglobin concentration at term (adjusted odds ratio 1.57, 95% CI: 1.01, 2.47; p = 0.044).
Conclusions:
The interventions were beneficial against low birthweight and preterm births which predispose to neonatal deaths and poor cognitive function in children. Malaria in pregnancy health campaigns should be intensified, especially among younger-aged primigravidae, to increase their knowledge of the condition as a way to further improve uptake of these preventive interventions.
Keywords
Introduction
Malaria in pregnancy (MiP) remains a public health concern largely in endemic areas and is associated with adverse pregnancy outcomes including maternal anaemia, low birthweight, prematurity, intrauterine growth restriction, stillbirth, abortion and maternal and newborn deaths.1,2 Placental and peripheral malaria infection at delivery doubled the odds of stillbirths in a systematic review. 2 Plasmodium falciparum MiP accounts for about 12.0%–20.0% of stillbirths and 11.0% of newborn deaths.2,3
The World Health Organization (WHO) recommends two key effective interventions for prevention of MiP in areas with stable malaria transmission; intermittent preventive treatment using sulphadoxine-pyremithamine (IPTp-SP) and sleeping under insecticide-treated bed nets (ITNs). IPTp-SP is the monthly administration of a full dose of SP under direct observation to pregnant women from 16 weeks until delivery. 4 Three or more doses of IPTp-SP was associated with a 20% reduced risk of low birthweight and about 50% less risk of placental malaria. 5 Varying effects of IPTp-SP on maternal anaemia have been reported.5,6 Consistent and proper use of ITNs has been shown to reduce low birthweight and miscarriage/stillbirth by 23.0% and 33.0% respectively in paucigravidae and also reduce placental parasitaemia by 23.0% in all gravidae. 7 Use of ITNs was found to be protective against maternal anaemia. 8
Despite available evidence of their effectiveness, uptake of these interventions has not been optimal. The 2021 world malaria report and an analysis of pooled data from malaria indicator surveys conducted over 2015–2019 in 12 sub-Saharan African countries showed only about 31.0%–34.0% of African pregnant women currently receive ⩾3 doses of IPTp-SP.9,10 The latter reported a 59.6% prevalence for Ghana. 10 Older age, employed status, higher education and wealth index and trust in the health care system have motivated IPTp-SP uptake11–13 while challenges like SP stock-outs, poor provider knowledge of IPTp-SP protocols, negative health staff attitudes, fear of adverse effects, late commencement of prenatal care and inadequate education of pregnant women on IPTp-SP have mitigated uptake.13–16
Regarding ITN use, a pooled analysis of data from 21 sub-Saharan African countries collected over 2010–2018 showed 74.2% of pregnant women used ITNs with age, wealth status and living in a male-headed household being facilitators for sleeping under ITNs. 17 This pooled analysis included data from the 2014 Ghana demographic and health survey which reported 49.2% ITN use among pregnant women. The WHO reported 52% ITN utilization among pregnant women in the 33 African countries with moderate to high malaria transmission in 2020. 9 Barriers to ITN use among pregnant women include heat, discomfort, urban residence and low level of education.18–20
The reported uptake of these interventions in Ghana falls below the targets of 80% set for both ⩾3 doses of IPTp-SP and ITN utilization among pregnant women in Ghana in the 2021–2025 national malaria strategic plan. This is in spite of the fact that MiP remains a burden in the country with an average malaria test positivity rate of 37.3% among pregnant women over 2014–2021. 21 Understanding individual-level dynamics that facilitate uptake of these interventions in particular geographic areas are crucial for designing measures to improve uptake in that locality. 22
Several studies have reported 32%–80.7% uptake of ⩾3 doses of IPTp-SP.23–27 and ITN utilization of 40%–95% in pregnant women25,28–31 in Ghana over the last decade. However, there is a paucity of data on the uptake of these interventions and a limited understanding of local factors influencing them in the Ho Municipality of the Volta Region. Literature review showed two studies that reported on uptake of either ITNs or IPTp-SP but not both in the Ho Municipality.28,32 A 42.5% ITN utilization was reported among antenatal care (ANC) attendants in the municipality in 2016 with higher educational level being a significant facilitator 28 while the second study found that 95% of post-partum women received 3–5 doses of IPTp-SP in 2021. 32 The present study was conducted among post-natal care (PNC) attendants at the Ho Teaching Hospital (HTH) to primarily assess current uptake of the two MiP interventions and the factors influencing them. The study further explored the effects of these interventions on pregnancy outcomes such as birthweight, preterm delivery and maternal anaemia at 36–40 weeks gestation. PNC attendants were used because they were more accessible than women at delivery. Additionally, these women recently completed their ANC and it was better to measure uptake of the malaria preventive interventions among them. ITN utilization in this population was used as a proxy for use during pregnancy on the assumption that it was unlikely they only started sleeping under ITNs in the post-partum period.
Methods
Study design, area population
This was a cross-sectional survey among post-partum women accessing PNC at the post-natal clinic of the HTH in the Ho Municipality, Volta Region, Ghana from 25 August 2022 to 9 October 2022. The HTH is a referral facility for the entire Volta Region and some parts of the Eastern Region. It also provides services to clients from neighbouring Togo. Clinic attendance for ANC numbered up to 6000 while 1964 deliveries were recorded in the maternity ward in 2021 (Biostatistics Unit, HTH, 2022). Malaria transmission in the study area is perennial with peaks in the two rainy seasons; March to July and September to November. Prevalence of malaria parasitaemia in pregnancy has generally declined in Ghana over the past 2 decades and this includes Ho which lies in the middle transitional/forest malaria epidemiological zone of the country. 33 Malaria parasitaemia in pregnancy prevalence of 2.4%–28.8%, over 2016–2019, have been reported in the near-by South Tongu, Central Tongu and Akatsi districts.34–36
Sample size estimation
The Cochran formula N = Z2pq/d2 was used to estimate the minimum sample size for the study. N is the sample size estimate, Z is the reliability coefficient of 1.96 for a 95% confidence interval, p is the proportion of ANC attendants receiving ⩾3 doses of IPTp-SP, q is 1-p and d is the allowable margin of error. Using ‘p’ of 66% from a study in the near-by Central Tongu district 35 and a 5% margin of error, a minimum sample size of 345 was estimated for the study.
Study procedures and data collection
Participants were included if they were ⩾18 years old, 2 weeks post-partum and had a singleton during the last pregnancy. Women who neither spoke Ewe nor English and who looked ill at the time of recruitment were excluded from the study. With an average daily attendance of 10–12 for PNC observed over the preceding 2 months, all attendants were approached every weekday for recruitment into the study. Thus, there was no sampling of the study participants.
At the post-natal clinic, potential participants had the study and its objectives explained to them for their consent. Where a woman refused participation in the study, the next woman in the queue was approached. Based on the exclusion criteria and refusal to participate, 32 (18 were 6-weeks post-partum, 5 had twin pregnancies, 3 were below 18 years of age and 6 refused participation) of the 381 women approached were excluded and the rest recruited. Data collection was done using a structured questionnaire developed by the investigators (see S1 Questionnaire under Supplemental Files) and administered in English or the local Ewe language where necessary by the second author. Data were collected on socio-demographic characteristics such as age and employment status, ownership of ITNs, whether participants slept under an ITN the night before the survey and a composite variable ‘knowledge of MiP’. The latter entailed assessing participants’ knowledge on the cause of malaria, its signs and symptoms, effects on the pregnant woman and the foetus and prevention.
The number of ANC visits during the last pregnancy, doses of IPTp-SP taken, haemoglobin concentration and gestational age at booking ANC visit, gestational age at delivery, birthweight and haemoglobin concentration at term (36–40 weeks) were obtained from a review of participants’ maternal and child health record books. Birthweight and gestational age at delivery were validated using the delivery register at the labour ward. The questionnaire was pretested among eight post-partum women at HTH and relevant changes were made for clarity before using it in the actual study. These women were outside the final sample size used and were not included in data analysis.
Statistical analysis
The questionnaires were checked for completeness and accuracy and data double-entered into an Excel template. The data was cleaned and analysed using Stata version 13 (College Station, TX, USA). Summary statistics were reported as frequencies, percentages, mean and standard deviation and median and range.
Knowledge of MiP was assessed based on 10 questions (see C2–C11 in the questionnaire). For questions C2 and C8–C11, a score of 1 was assigned to the correct answer and all other options assigned 0. Question C3 allowed for multiple answers though there was only one correct answer. The correct answer for C3 was ‘I don’t know’ and it was assigned a score of 1 provided the study participant selected that option alone. All other options attracted a score of 0. Selecting multiple answers that included the option ‘I don’t know’ still attracted a score of 0. This was to emphasise the importance attached to knowing the correct answer.
Questions C4–C6 also allowed for multiple answers and a score of 3 was assigned if participants provided at least 2 correct answers. Providing only one correct answer attracted a score of 1 while wrong answers and the ‘I don’t know’ option were assigned a score of 0. Question C7 centered on what a pregnant woman can do to protect herself from malaria and it also allowed for multiple answers. The options for ITN use and IPTp-SP were each assigned a score of 2 and the other correct but less important options assigned 1 for at least one correct choice. The option ‘I don’t know’ was assigned 0. The total score was 20 and a score of ⩾14 was deemed to represent good knowledge of MiP while <14 was described as poor knowledge of MiP. The choice of 14 as a cut-off was arbitrary and based on a desire for pregnant women to have sufficient knowledge of MiP. Though subjective and limits comparison to other studies, such arbitrary categorisation schemes have been used in previous studies.37,38
The two primary outcome variables were (i) IPTp-SP uptake (<3 and ⩾3 doses) and (ii) ITN use defined as ‘whether participant slept under an ITN the night before the survey’ (‘No’ and ‘Yes’). Bivariate logistic regression was used to assess for association between selected independent variables including age, education and gestation at booking and each of the two study primary outcomes. Participant characteristics such as religion, ownership of ITN, source of ITN and number of ANC visits were essentially homogeneous and were not included in the bivariate analysis. In the multivariate analysis, all independent variables earlier explored in the bivariate analysis were included in a backward stepwise elimination process using a threshold p-value of 0.1.
In a second level of analysis, the two primary outcome variables were used as independent variables and their association with the dependent variables ‘birthweight’ (low birthweight and normal birthweight), ‘gestational age at delivery’ (preterm and term babies) and ‘participant’s haemoglobin concentration at 36–40 weeks (term)’ (maternal anaemia or normal haemoglobin concentration at term) investigated using logistic regression methods. Regardless of an association (defined as p < 0.05) in the bivariate analyses, IPTp-SP uptake and ITN use were included in multivariate analyses for each dependent variable on account of a plausible association and because IPTp-SP uptake was associated with a decreased risk of anaemia at term/delivery in paucigravidae in a systematic review. 5 Crude and adjusted odds ratios with 95% confidence intervals were reported. A p-value of <0.05 was considered statistically significant in the final multivariate models.
Definition of some variables/terms used
Optimal dose of IPTp-SP is receiving ⩾3 doses of IPTp-SP.
Normal birthweight is birthweight 2500 g and above.
Low birthweight is birthweight <2500 g.
Maternal anaemia is haemoglobin concentration less than 11 g/dl. Moderate anaemia is haemoglobin concentration of 7 g/dl–9.9 g/dl. Mild anaemia is 10.0–10.9 g/dl.
A preterm baby is one delivered at less than 37 weeks gestation.
Ethical considerations
Permission was also obtained from the management of the HTH. Written informed consent was obtained prior to study initiation after explaining the objectives, risks and benefits of the study in English or the local Ewe language. Literate participants signed the informed consent form to indicate participation. The few illiterate participants thumb printed the informed consent form in the presence of the PNC clinic midwives as these women either came to the clinic alone or were accompanied by under-age helpers who could not be deemed as legally authorized representatives. Participants were informed that participation was voluntary and refusal to participate would not result in denial of care. Participants’ details were anonymized using study codes to ensure confidentiality.
Results
Study participants’ background and clinical characteristics
Three hundred and forty-nine women contributed data for analysis. Table 1 summarises the participants’ background and clinical characteristics. The mean age (SD) was 29.4 years (5.4) and 67.6% (236) were in the age group 25–35 years. At least three-quarters (77.6%) were married and 72.2% (252) were of parity ⩽2. About 70% (243) had either been educated up to the senior high school or tertiary level while nearly 80% (279) were employed. Four out of five women started their ANC visits within the first trimester and 36.5% (128) were anaemic (Hb < 11 g/dl) at booking. About 6% (22) of the participants had low birthweight babies while 8% (28) had preterm deliveries. Of the study women, 263 (75.4%) had good knowledge of MiP.
Participants’ background and clinical characteristics.

These were muslims and traditionalists.
Includes 6 years of primary school and 3 years of junior high school.
Insecticide-treated net use and uptake of IPTp-SP
Over 90% (327) of the participants reported owning ITNs and these were mostly given at ANC. About two-thirds, 64.8% (226), of participants slept under ITN the night before the survey. Of those who did not sleep under ITNs the night before the survey, 91 (74%) reported they were either not comfortable with the ITNs or simply did not feel like sleeping under them. Four (3.3%) women had the nets but had not been able to hang them yet while the others did not have it or felt there were no mosquitoes in their rooms.
Majority, 83.7% (291), of the women had optimal doses of IPTp-SP while 44 (12.6%) received one or two doses. Thirteen women (3.7%) had no evidence in their ANC books that they had taken any dose of IPTp-SP (see Table 1). It was thus documented that they had taken none at all.
Determinants of IPTp-SP uptake
In the bivariate analysis, older women had higher odds of receiving optimal doses of IPTp-SP. Women in the age group 25–35 years had five times the odds compared to those 18–24 years (OR 5.09, 95% CI: 2.67, 9.70; p < 0.001). Participants above 35 years also had about six times the odds of receiving ⩾3 doses of IPTp-SP compared to the reference group (OR 5.79, 95% CI: 2.02, 16.60; p =0.001). Women of parity 2 also had almost three times the odds of taking ⩾3 doses (OR 2.91, 95% CI: 1.39, 6.08; p = 0.005) compared to women of parity 1 (see Table 2). Employed participants had higher odds of receiving ⩾3 doses compared to unemployed ones (OR 4.27, 95% CI: 2.32, 7.88; p < 0.001). Women with tertiary education had six times the odds of receiving ⩾3 doses of IPTp-SP compared to those with none at all (OR 6.00, 95% CI: 1.56, 23.11; p = 0.009).
Logistic regression output for factors influencing uptake of IPTp-SP and ITN use.

Being in the age group 25–35 years and >35 years, having a good knowledge of MiP, being employed and commencing ANC later than 13 weeks remained statistically significant in the final multivariate model (see Table 2).
Factors influencing ITN use
Women aged 25–35 years (OR 2.46, 95% CI: 1.39, 4.33; p = 0.002) and >35 years (OR 3.14, 95% CI: 0.99, 4.59; p = 0.052) had higher odds of sleeping under an ITN the night before the survey compared to those 18–24 years in the bivariate analysis (see Table 2). Similarly, women of parity 2 (OR 2.44, 95% CI: 1.43, 4.15; p = 0.001) and ⩾3 (OR 2.19, 95% CI: 1.26, 3.81; p = 0.005) also had twice the odds of sleeping under an ITN the night before the survey compared to women of parity 1. Participants who were employed had twice the odds of sleeping under an ITN the night before the survey (OR 2.17, 95% CI: 1.27, 3.70; p = 0.004) while those who commenced ANC later than 13 weeks had a 49% reduced odds of sleeping under an ITN the night before the survey (OR 0.51, 95% CI: 0.29, 0.88; p = 0.016).
In the multivariate analysis, being employed (AOR 1.78, 95% CI: 1.02, 3.09; p = 0.043), parity 2 (AOR 2.18, 95% CI: 1.27, 3.74; p = 0.005) and parity ⩾3 (AOR 2.13, 95% CI: 1.21, 3.75; p = 0.009) doubled the odds of sleeping under an ITN the night before the survey (see Table 2).
Comparison of haemoglobin concentrations at booking ANC visit and at 36–40 weeks
About 63% of the study women had normal haemoglobin concentration at their booking visit but this reduced to 49.3% by gestational age 36–40 weeks (see Table 1). The proportions of participants with moderate anaemia at booking and at term appeared to be comparable (12.3% versus 13.0%) while the proportion with mild anaemia increased at term compared to booking (37.7% versus 23.9%) (see Table 1).
Association between IPTp-SP uptake and ITN use as exposure variables and birthweight, maternal anaemia at 36–40 weeks (term) and gestational age at delivery
In the bivariate analysis, optimal doses of IPTp-SP had almost three times the odds of having normal-weight babies (⩾2500 g) (OR 2.77, 95% CI: 1.06, 7.21; p = 0.037) but neither influenced gestational age at delivery nor maternal anaemia at term. Women who slept under an ITN the night before the survey had approximately three times the odds of having term babies (OR 2.66, 95% CI: 1.22, 5.84; p = 0.014) compared to those who did not. There was no association between ITN use and birthweight or maternal anaemia at term (see Table 3).
Logistic regression output for association between IPTp-SP uptake and ITN use as exposure variables and birthweight, gestational age at delivery and maternal anaemia at 36–40 weeks/term.
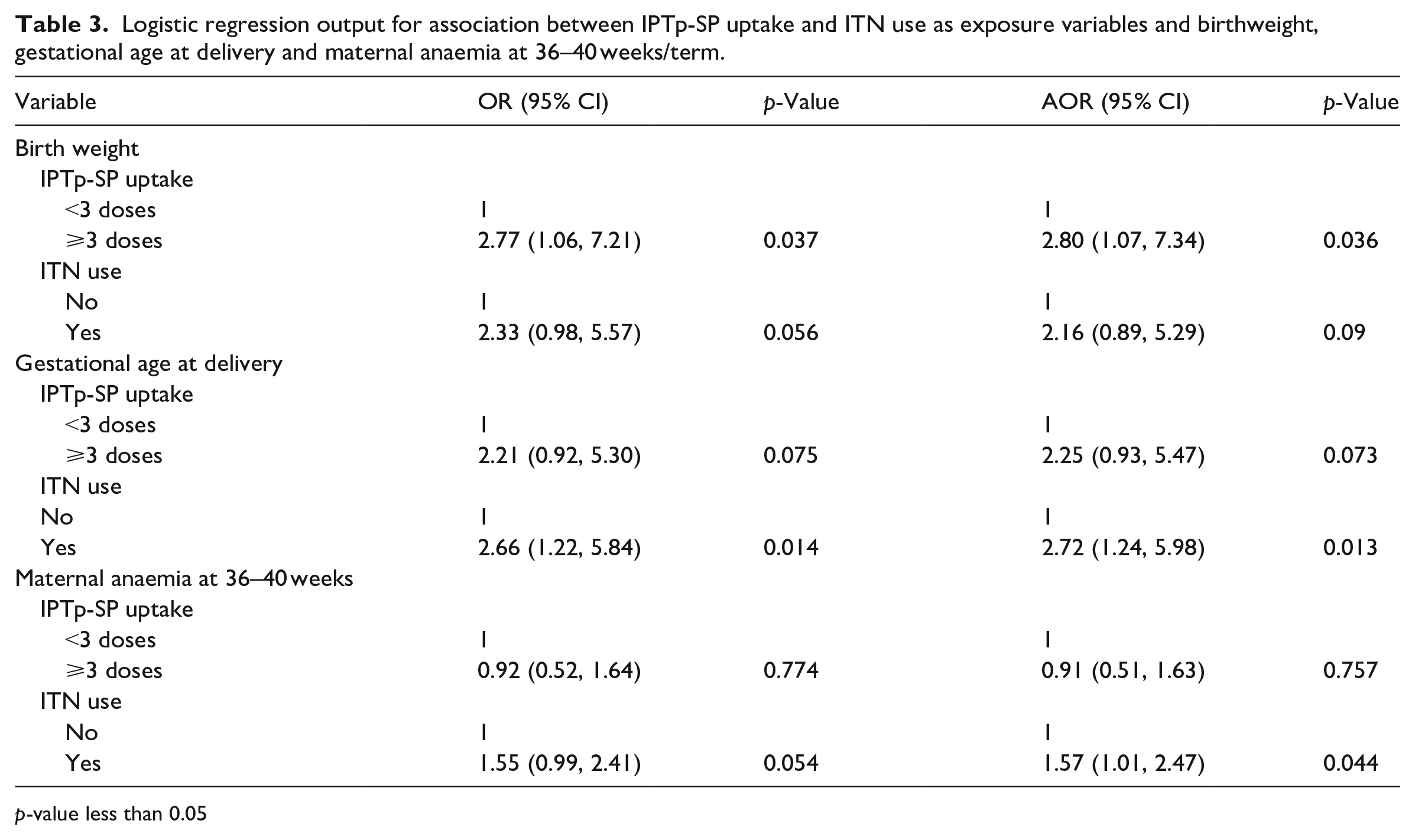
p-value less than 0.05
Adjusting for ITN use, receiving ⩾3 doses of IPTp-SP maintained the higher odds of having normal-weight babies as observed in the bivariate analysis (AOR 2.80, 95% CI: 1.07, 7.34; p = 0.036) (see Table 3). Similarly, adjusting for IPTp-SP uptake, ITN use maintained its association with having term babies (AOR 2.72, 95% CI: 1.24, 5.98; p = 0.013) and was associated with about twice the odds of having normal haemoglobin concentration at term (AOR 1.57, 95% CI: 1.01, 2.47; p = 0.044) (see Table 3).
Discussion
The study reports on the uptake of ⩾3 IPTp-SP doses, ITN use and their determinants among women accessing PNC at HTH in the Ho Municipality to help appreciate local factors at play and subsequently inform context-specific measures to improve uptake of these ANC interventions. More than 80% of respondents received ⩾3 doses of IPTp-SP while 64.8% slept under ITNs the night before the survey. Age >25 years, employment, good knowledge of MiP, parity ⩾2 and initiating ANC visits in the first trimester facilitated the uptake of these interventions. Optimal doses of IPTp-SP and ITN use were observed to protect against low birthweight, preterm delivery and maternal anaemia at term. To the best of the authors’ knowledge, this is the first report of both IPTp-SP uptake and ITN use in the municipality and their effect on birthweight, premature birth and maternal anaemia at term.
Approximately 84% of the study women received optimal IPTp-SP doses in their last pregnancy. This is higher than national level reports of 55.0% in 2021 from Ghana’s district health information management systems database (DHIMS 2) 21 and the 61% reported in the 2019 malaria indicator survey. 27 This may be due to differences in the denominator for computing these measures. For DHIMS 2, the denominator is the total number of ANC registrants over the year 39 which includes women who have not yet completed their ANC while that used in surveys such as the present study is the total number of respondents surveyed and these correspond to those who have completed their ANC. Thus, the denominator for the DHIMS 2 is invariably larger and could account for the lower uptake seen. Another explanation is the larger population size used in the DHIMS 2. The wide difference between the 61.0% in the 2019 malaria indicator survey (MIS) and the 84% in the present study could be because the MIS covers a much larger geographical area, population size and wider variability in the IPTp-SP uptake. The uptake of optimal doses in the current study far exceeds the 64.5% and 71.0% reported in some Ghanaian studies26,40 but comparable to the 2019 report of 80.7% in Sekondi-Tarkoradi also in Ghana. 24 It is, however, lower than the 95% reported among post-partum women about a year earlier at the same study site 32 and this calls for operational research into the seeming reduction in uptake of optimal IPTp-SP doses at HTH.
Age >25 years, employment and good knowledge of MiP facilitated uptake of optimal IPTp-SP doses while starting ANC later than 13 weeks was a barrier. Being employed has been reported to be associated with taking optimal doses of IPTp-SP in a review in Nigeria. 16 In contrast, other studies observed a lack of association with or a reduced odds of taking at least 3 doses of IPTp-SP with an employed status.23,40 The association between good knowledge of MiP and optimal doses of IPTp-SP in the present study compares favourably with earlier reports.13,40 Some studies have reported that pregnant women with adequate knowledge of the effects of MiP were eager to buy the SP themselves during stock-outs.13,41 This reinforces the importance of malaria-related health promotion messages delivered at ANC and through other mass communication channels in both English and local languages.
In the current study, initiating ANC visits later than 13 weeks was associated with a statistically significant reduced uptake of ⩾3 doses of IPTp-SP presumably because there may not be sufficient time to complete the recommended doses, especially if the pregnant woman started very late. This finding resonates with earlier reports of early ANC initiation being associated with receiving optimal doses of IPTp-SP42–44 but contrasts with another study that did not find any association between gestational age at booking and uptake of optimal IPTp-SP doses. 40 About 41% (26) of the women in the present study who started ANC later than 13 weeks did so between 18 and 28 weeks gestation. With the current dose protocol 4 and barring any premature delivery, it should be possible to receive three IPTp-SP doses with ANC booking visit even at 28 weeks. Probably, there may be other ‘hidden factors’ beyond initiating ANC later than 13 weeks at play in the context of the present study. These may include study participants’ non-adherence to ANC visit schedules, intermittent SP stock-outs and health provider non-adherence to IPTp-SP protocols. These factors were not investigated in the present study but have been reported previously.13,45
Women >25 years had increased odds of optimal IPTp-SP doses compared to those <25 in the present study. Similar observations were reported10,17,46,47 although age ⩾40 was not associated with uptake of at least 3 IPTp-SP doses in a trend analysis of IPTp-SP uptake in Ghana. 47 Another Ghanaian study did not find any association between age and uptake of IPTp-SP. 40 Younger-aged women may not want to attend ANC to access important interventions probably for fear of being stigmatised on account of getting pregnant outside marriage. This may explain their reduced odds of receiving at least 3 doses of IPTp-SP. However, this is not always the case as some studies have shown older age facilitates ANC utilisation48,49 while others reported age ⩽20 years at first pregnancy increased the likelihood of ANC attendance.50,51 Contrary to findings from the present study, other studies reported that marriage and at least secondary school education increased the odds of optimal IPTp-SP doses23,44,47 while parity greater than four reduced the odds of taking at least 3 IPTp-SP doses. 23
About 16.3% of respondents in the present study had less than 3 doses of IPTp-SP. This is in spite of observations that 97% of the participants attended ANC at least four times and nearly 82% initiated ANC before 13 weeks. It is possible some of these women started ANC late and also had preterm deliveries. Other factors such as stock-outs and missed opportunities 13 may have played a role. The common reasons women who had less than 3 IPTp-SP doses in what the 2019 Ghana malaria indicator survey gave were that they were only given that frequency of tablets and they didn’t know they had to take more. Qualitative approaches are needed to elicit nuanced contexts around why these particular women did not get the recommended three or more doses.
The current study reported ITN utilisation of 64.8% despite a 93.7% ownership. This prevalence of ITN use is higher than the 42.5% reported among ANC attendants in the Ho Municipality in 2016 28 and the 49% observed in the 2019 MIS. 27 The ITN utilisation falls short of the 80% target set in Ghana’s 2021–2025 national malaria strategic plan and reinforces previous observations that ITN use lags behind ownership. 52 Discomfort and the perception that there were no mosquitoes in their rooms were some reasons given by the respondents for not using ITNs in the present study and these are corroborated by other studies.18,19 Innovative behaviour change communication strategies are needed to sustainably improve ITN utilisation among pregnant women. Provision of incentives to encourage ITN use has been considered but a systematic review showed it was ineffective. 53 Besides, this strategy is hardly sustainable.
Being employed doubled the odds of ITN use in the present study. Employment was significantly associated with ITN use among pregnant women in Ethiopia 54 and may be linked to an increased economic power to purchase bed nets and to also take decisions for their health. However, economic empowerment is unlikely to be the case in the present study as about 83% of the study women received free nets during pregnancy while only about 5% reported purchasing the nets themselves. The policy and practice in Ghana is to provide all pregnant women with ITNs at the booking ANC visit. Stock-outs or lack of logistics for their distribution from central points to peripheral health facilities have been known to occur and affect ownership/utilisation. 55
Being of parity ⩾2 increased the odds of ITN use and this is similar to previous findings.22,56 It is possible that the study women perceived having previous livebirths as proof of the effectiveness of ITNs and a motivating factor to use them in subsequent pregnancies. It could also be a question of the women protecting their children from malaria and thus sleeping under the nets with them. Other studies did not find an association between parity and ITN use.54,57
Similar to previous findings, 19 age was not associated with ITN use in the present study. However, other studies have reported older58,59 or younger-aged pregnant women20,60 slept more under ITNs. Though higher levels of education are associated with ITN use in pregnant women,28,31 no such association was observed in the current study.
Optimal doses of SP had about three times the odds of having babies with normal birthweight in the multivariate analyses. This finding compares favourably with previous reports that found fewer occurrences of low birthweight with ⩾3 doses.5,26,58 Malaria-attributable low birthweight arises from preterm birth and/or small-for-gestational age babies. 61 Preterm birth is mediated by parasite-induced placental inflammatory processes that distort the balance needed to keep a pregnancy to term while fetal growth restrictions from placental insufficiency lead to small-for-gestational age babies.61,62 Though it is not completely clear how SP improves pregnancy outcomes, using IPTp-SP and ITNs mitigate the adverse processes described and increase the odds of having term babies with normal weights. 61 Using SP is also known to help treat or prevent bacterial infections including sexually transmitted and urinary tract infections that have been associated with adverse pregnancy outcomes such as preterm delivery. 61 Sulphadoxine helps regulate bacterial composition in the gut and vagina and this promotes weight gain. 61 Taking less than 3 or at least 3 doses of IPTp-SP neither influenced gestational age at delivery nor anaemia at term in the present study and this is similar to earlier findings.5,6 In spite of the variations, ⩾3 doses of IPTp-SP remain the recommendation to help reduce malaria-related maternal anaemia and low birthweight in endemic areas.
ITN use was associated with term babies and normal haemoglobin concentrations at term in the current study. Current studies directly evaluating the effect of ITNs on maternal anaemia are lacking but earlier assessments showed variable outcomes.63–65 Two studies showed a similar prevalence of maternal anaemia for ITN alone and ITN combined with IPTp-SP.66,67 Insecticide-treated net use was not associated with preterm delivery in a previous study. 64
The prevalence of anaemia increased from 36.8% at booking to 50.7% at 36–40 weeks in spite of observations that nearly 84% of the study women received IPTp-SP at least three times and about 65% reported they slept in an ITN the night before the survey. These findings contrast with those from a trend analysis of Ghana’s DHIMS 2 data that showed the prevalence of anaemia at term was persistently lower than at booking in the 10-year period from 2012 to 2021. 21 It is not immediately clear why the present study showed an increase in anaemia prevalence between booking ANC visit and 36–40 weeks but the findings provoke important questions on other contributors to maternal anaemia aside malaria infection, ITN use and uptake of IPTp-SP. The study did not take into consideration morbidities such as helminthiasis, sickle cell disease and other haemoglobinopathies, human immunodeficiency virus infection, schistosomiasis and others that could impact on maternal anaemia. Another pertinent issue is pregnant women’s poor adherence to iron and folic acid supplementation (IFAS) that is supposed to help counter the increased demand for these nutritional elements during pregnancy. A meta-analysis showed just about 4 out of 10 women adhere to IFAS in sub-Saharan Africa. 68 All participants in the present study received IFAS as part of the ANC package of interventions but adherence was not assessed. Similarly, conditions such as hypertensive diseases and diabetes in pregnancy and maternal nutritional status that can influence birthweight and prematurity were not considered in examining the association between ITN use and uptake of IPTp-SP and birthweight. These gaps may cloud the interpretation of some study findings.
Other study limitations include the fact that the study was done at a single centre and this limits its external validity as the women who accessed ANC at HTH may differ in some characteristics from those who attended ANC clinics at other health facilities in the Ho Municipality. HTH being a referral centre, it is possible that some women may have been referred there from other facilities in the municipality in which case some degree of representativeness would have been achieved. Also, responses regarding knowledge of MiP were not validated. Lastly, a comprehensive socioeconomic assessment including access to safe water and sanitation was not done for the participants but these can impact on maternal anaemia. Nevertheless, the study provides meaningful insights into the local determinants of the uptake of both ITNs and optimal doses of IPTp-SP that can inform health promotion campaigns for improving uptake of MiP interventions in the municipality.
Conclusion
Among the study participants, uptake of optimal doses of IPTp-SP exceeded the national target of 80% and protected against low birthweight. Insecticide-treated bed net use appreciably lagged behind ownership and reduced the odds of preterm births and maternal anaemia at term. Uptake of these MiP prevention interventions can further be improved with sustained malaria-related health promotion campaigns to increase pregnant women’s knowledge of MiP. Public health managers, political leadership, mass media channel operators and other stakeholders in the municipality must work together in the delivery of these messages. The campaigns are more likely to be effective if there are efforts to target young, nulliparous pregnant women less than 25 years old. Pregnant women must also be encouraged to initiate ANC visits as soon as they realise they are pregnant as this increases the odds of receiving optimal IPTp-SP doses. Future studies are needed to identify the best options for behaviour change communication strategies to improve ITN utilization in the municipality.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231199653 – Supplemental material for Interventions for malaria prevention in pregnancy; factors influencing uptake and their effect on pregnancy outcomes among post-natal women in a tertiary facility in the Volta Region of Ghana
Supplemental material, sj-docx-1-smo-10.1177_20503121231199653 for Interventions for malaria prevention in pregnancy; factors influencing uptake and their effect on pregnancy outcomes among post-natal women in a tertiary facility in the Volta Region of Ghana by Gifty Dufie Ampofo, Abraham Kwadzo Ahiakpa and Joseph Osarfo in SAGE Open Medicine
Footnotes
Acknowledgements
The authors are grateful to the study participants and midwives at the HTH PNC clinic.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from *the University of Health and Allied Sciences Research Ethics Committee (UHAS-REC A.11 [211] 21-22))*.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study and after explaining the objectives, risks and benefits of the study in English or the local Ewe language. Literate participants signed the informed consent form to indicate participation. The few illiterate participants thumb printed the informed consent form in the presence of the PNC clinic midwives as these women either came to the clinic alone or were accompanied by under-age helpers who could not be deemed as legally authorized representatives.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.