
Abstract
Objective:
The objective of this paper is to evaluate Augmented Web-based Applicant Experiences in the field of Anesthesiology. We hope to advocate for Augmented Web-based Applicant Experiences rotations and address their limitations in case in-person rotations become restricted again.
Methods:
A thorough search of articles from the years 1978 to 2023 was completed using the search phrases “Away Rotations Anesthesiology,” “Away Rotations Anesthesia,” “Audition Rotation Anesthesia” and “Audition Rotation Anesthesiology.” These search phrases were used on both the PubMed (Medline) and Excerpta medica database (EMBASE) databases, and the number of total articles that appeared was 73. These articles were then filtered to gather relevant articles for our study.
Results:
After the articles were filtered, there was one remaining article that was used for our study. To supplement this article, 29 additional sources were added using the worldwide web. However, these did not address rotations in Anesthesiology. Although these other sources did not involve Anesthesiology residencies, they still provide significant perspectives that can be applied to online rotations. A total of 30 sources were used for our manuscript.
Conclusion:
Although in-person rotations are preferred, Augmented Web-based Applicant Experiences rotations are valuable as they give residency programs an opportunity to evaluate students. Augmented Web-based Applicant Experiences rotations also provide students with learning opportunities and also help familiarize them with the residency programs. There are limitations that come with Augmented Web-based Applicant Experiences rotations. However, addressing these shortcomings can help Augmented Web-based Applicant Experiences rotations become a proper substitution for in-person rotations if they become restricted again.
Introduction
In 2020, there were a total of 1884 US anesthesia residency positions for which 2339 people applied. 1 Obtaining positions becomes significantly harder each year as the number of medical students in the United States increases faster than the number of available positions for residency. 2 Many students choose to do an “audition elective” in hopes of gaining an advantage when applying for residency programs by making themself familiar with the host program. The term “audition elective,” often used interchangeably with “away rotation,” describes a clinical elective wherein a student spends time as a medical student outside his or her home institution. Many program directors rank the audition elective highly among the tools used to choose potential residents. 3 Medical students also report feeling more competitive for residencies after completing audition electives. 4
During the severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) pandemic, medical students’ ability to seek these opportunities was negatively impacted. The American Society of Anesthesiologists (ASA) acknowledges that students who do secure an away rotation may still have their opportunities greatly limited even with the gradual recovery from the pandemic. 5 As a result, several schools have released virtual sub-internships meant to simulate an away rotation. Named the Augmented Web-based Applicant Experiences (or AWAE rotations), these programs offer personal interactions with program directors and faculty, skills workshops, virtual tours, virtual rounds, and other opportunities. These AWAE rotations exist in specialties such as plastic surgery, radiology, and otolaryngology but are scarce in the field of anesthesiology.6–8 At this time there is no academic literature available describing away rotations in Anesthesiology. The objective of this paper is to outline Anesthesiology AWAE rotations in the event that in-person rotations are restricted in the future.
Methods
To identify potentially pertinent articles for our research, we employed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) systematic review approach. 9 We conducted an extensive search on the PubMed (MEDLINE) and EMBASE databases to acquire relevant articles. In Step 1, we employed a comprehensive keyword search using the phrases “Away Rotations Anesthesiology,” “Away Rotations Anesthesia,” “Audition Rotation Anesthesia” and “Audition Rotation Anesthesiology.” The total number of articles these search phrases generated was 73. The number of articles that appeared from each search phrase is shown in Figure 1. These articles encompass a time span from 1978 to 2023. Before the articles were screened, 18 duplicates were removed. The criterion for inclusion was whether or not the article included information about online away rotations based on the title and abstract. If the article contained relevant information regarding away rotations, then the whole manuscript was analyzed to determine if it should be used. Additional relevant articles were added through the world wide web. The whole process yielded qualitative information that amounted to a total of 30 relevant articles for our topic of interest. These articles were examined in detail, wherein the results and descriptions were extracted from the manuscripts.

Study flow chart.
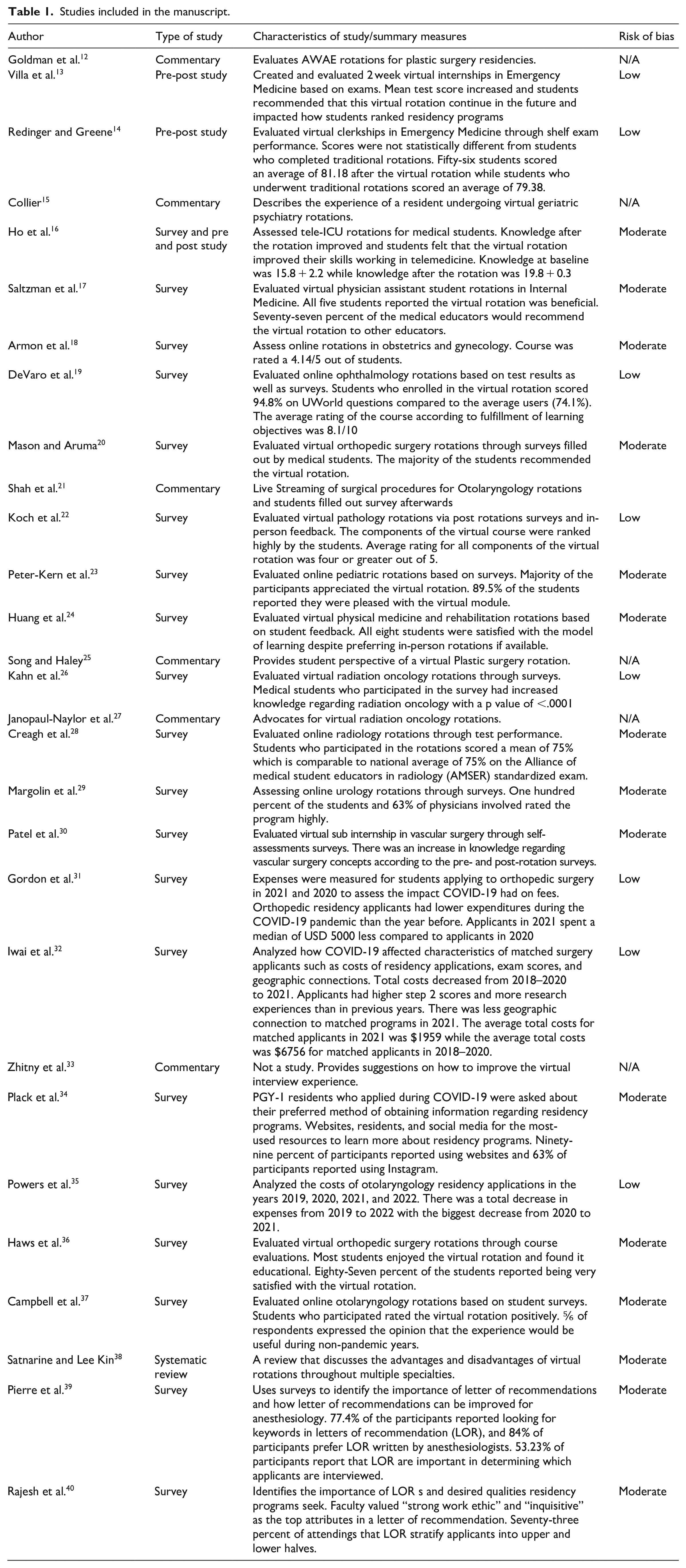
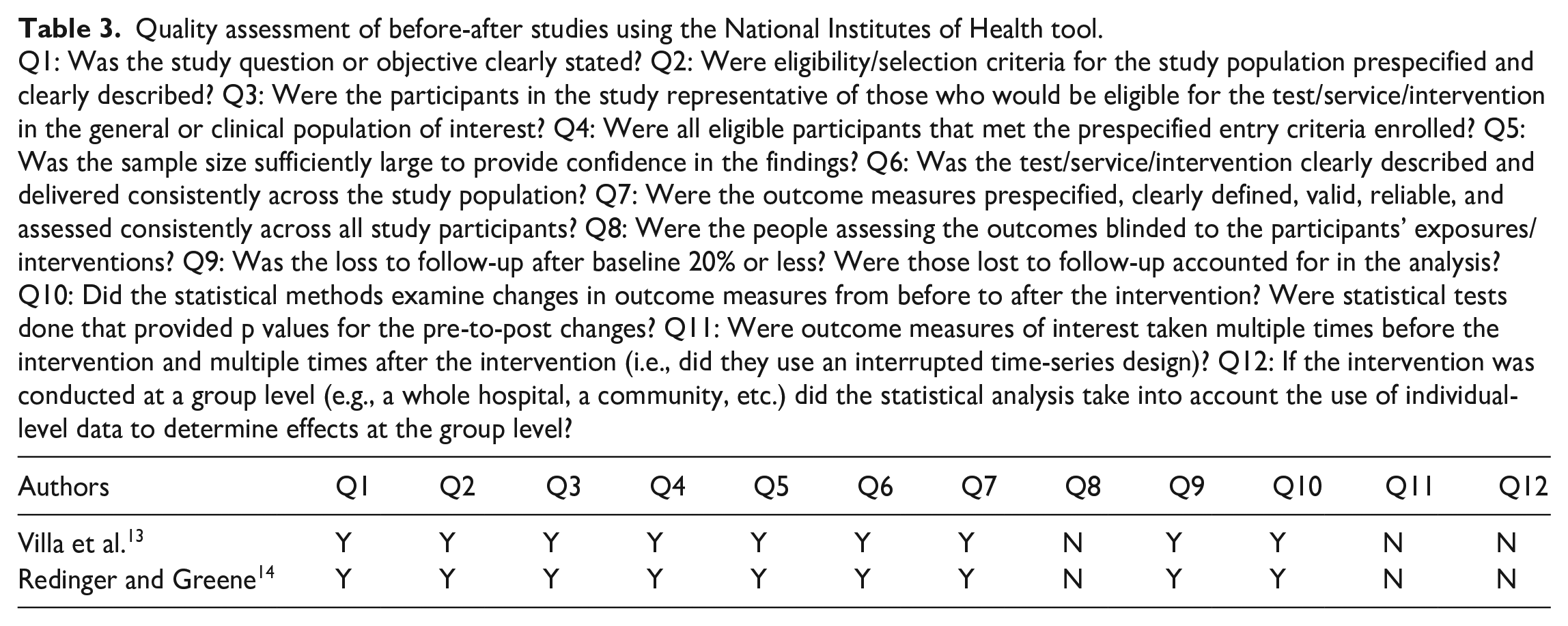
Risk of bias of the articles were determined based on the National Institute of Health study quality assessment tools and critical appraisal of a survey tool created by the Center of Evidence Based Management. Based on these tools, the articles were classified as “high,” “medium,” or “low” risk of bias (Table 1).10,11 A score between 100%–75% was considered low risk of bias, 75%–25% was considered medium risk of bias, and less than 25% was considered high risk of bias. The assessment of surveys using the risk of bias tools is shown in Table 2, while the assessment for pre-post studies are shown in Table 3. Systematic reviews were also assessed in Table 4. Three researchers carried out the procedures to obtain the final sample. The investigation team agreed on the final selection of the literature.
Studies included in the manuscript.
Quality assessment of surveys using the Center for Evidence-Based Management tool.
Q1: Did the study address a clearly focused question/issue? Q2: Is the research method (study design) appropriate for answering the research question? Q3: Is the method of selection of the subjects (employees, teams, divisions, organizations) clearly described? Q4: Could the way the sample was obtained introduce (selection) bias? Q5: Was the sample of subjects representative with regard to the population to which the findings will be referred? Q6: Was the sample size based on pre-study considerations of statistical power? Q7: Was a satisfactory response rate achieved? Q8: Are the measurements (questionnaires) likely to be valid and reliable? Q9: Was the statistical significance assessed? Q10: .Are confidence intervals given for the main results? Q11: Could there be confounding factors that haven’t been accounted for? Q12: Can the results be applied to your organization?

Quality assessment of before-after studies using the National Institutes of Health tool.
Q1: Was the study question or objective clearly stated? Q2: Were eligibility/selection criteria for the study population prespecified and clearly described? Q3: Were the participants in the study representative of those who would be eligible for the test/service/intervention in the general or clinical population of interest? Q4: Were all eligible participants that met the prespecified entry criteria enrolled? Q5: Was the sample size sufficiently large to provide confidence in the findings? Q6: Was the test/service/intervention clearly described and delivered consistently across the study population? Q7: Were the outcome measures prespecified, clearly defined, valid, reliable, and assessed consistently across all study participants? Q8: Were the people assessing the outcomes blinded to the participants’ exposures/interventions? Q9: Was the loss to follow-up after baseline 20% or less? Were those lost to follow-up accounted for in the analysis? Q10: Did the statistical methods examine changes in outcome measures from before to after the intervention? Were statistical tests done that provided p values for the pre-to-post changes? Q11: Were outcome measures of interest taken multiple times before the intervention and multiple times after the intervention (i.e., did they use an interrupted time-series design)? Q12: If the intervention was conducted at a group level (e.g., a whole hospital, a community, etc.) did the statistical analysis take into account the use of individual-level data to determine effects at the group level?
Quality assessment of systematic reviews using the National Institutes of Health Tool.
Q1: Is the review based on a focused question that is adequately formulated and described? Q2: Were eligibility criteria for included and excluded studies predefined and specified? Q3: Did the literature search strategy use a comprehensive, systematic approach? Q4: Were titles, abstracts, and full-text articles dually and independently reviewed for inclusion and exclusion to minimize bias? Q5: Was the quality of each included study rated independently by two or more reviewers using a standard method to appraise its internal validity? Q6: Were the included studies listed along with important characteristics and results of each study? Q7: Was publication bias assessed? Q8: Was heterogeneity assessed? (This question applies only to meta-analyses.).

Results
There was only one relevant article found when using the PubMed and EMBASE databases. This article discussed the use of social media and residency websites as favorable sources of information for online away rotations. Twenty-nine other articles were found through the world wide web for a total of 30 articles used. However, these articles that did not address the field of anesthesiology and only evaluated virtual rotations in other various medical fields such as otolaryngology, emergency medicine and orthopedic surgery, benefits and drawbacks of online away rotations, and significance of LOR in the context of away rotations. The risk of bias of these articles ranged from low to medium which is shown in Table 1.
Overall, the current literature of online away rotations for anesthesiology residencies is limited in academic literature with only a single article directly addressing this topic. The inclusion of related articles from different medical specialties and the exploration of virtual experiences and interviews provide valuable insights into the potential benefits and challenges of online rotations in the broader medical education landscape.
Discussion
Away rotations are an integral part of medical training in the United States. Due to the COVID-19 pandemic these mini-internships had an opportunity to be conducted virtually. 41 While previous research has analyzed the practicality of AWAE rotations in other medical specialties, a virtual away rotation specific to anesthesiology has yet to be described.12–30 Although these experiences for surgical specialties may play a vital role in educating students, it remains uncertain whether these experiences can be treated as an audition for a potential seat for an anesthesiology residency position. Considering the significant role that away rotations play in the selection of residents by program directors and the perceived benefits for students, it is crucial to objectively evaluate the advantages and disadvantages of AWAE rotations. This paper aims to contribute to the understanding that AWAE rotations have a rightful place in the field of anesthesia.
Benefits
It may seem as though an AWAE rotation would require additional supplies for medical students, but the required supplies already exist for the residents of these institutions. The same mannequins, Macintosh and Miller laryngoscopes, ultrasound machines, and central line kits that the residents utilize can be borrowed by the medical students from the medical schools. The medical schools typically re-use open single-use equipment such as laryngoscopes and central line kits, often donated by the hospitals albeit expired equipment or open-unused equipment. In other words, lack of medical equipment should not be an issue because the student can utilize the supplies of the institution which the students already attend. Furthermore, laryngoscopes and central line kits are used on a mannequin model rather than a patient. Therefore, they do not need to be sterilized and can be reused. Ideally, medical schools possess access to advanced airway devices just for their students to practice with mannequins ranging from those used to practice cardiopulmonary resuscitation to more advanced, interactive models, and robotic surgical systems.
Many of the maneuvers in anesthesiology that students will be expected to learn can be done remotely through observation by an online platform application such as Webex or Zoom. In addition, using technology that allows medical students to record themselves performing the procedure will allow attending physicians at an AWAE rotation to evaluate the students via video assessment. For example, a central venous access procedure can be ultrasound-guided on a mannequin after observation of a custom tutorial or via a remote instructor providing live feedback to the student via phone or screen-share online application. Modern Ultrasound guided applications such as Butterfly Ultrasonography can be screen-shared on a remote device such as a smartphone or a tablet device. This would allow a student to carry out similar procedures like nerve blocks given the availability of a proper mannequin. A custom-designed mannequin designed for central venous access that the medical schools possess for their trainees will have multiple access sites including internal jugular veins, subclavian veins, and carotid arteries. These vessels can be located using ultrasound to ensure cannulation of the correct vessel. Successful cannulation of either the vein or artery can be shown by the red or blue flow of fluids in the syringe meant to signify blood and the pulsatile nature of the artery flow in the mannequins. Other procedures that can be done completely remotely in a similar fashion include direct laryngoscopy, laryngeal mask airway (LMA) insertion, and fiberoptic intubation (Table 5). We propose that institutions hosting AWAE rotations should at the very least instruct their students on these procedures as they are very commonly used in anesthesiology practice.
Minimal modalities to be used to educate an AWAE rotation medical student.

In addition to the aforementioned advantages, AWAE rotations offer several other compelling benefits. One notable advantage is the significant cost reduction associated with rent and travel expenses to rotation sites. Traditional away rotations often impose a financial burden on medical students, requiring them to secure temporary housing and bear the costs of transportation. By shifting to AWAE rotations, these expenses can be mitigated, enabling students to allocate their financial resources more efficiently. This aligns with the trend observed in online residency program interviews, where the adoption of virtual platforms has the potential to alleviate financial burdens and scheduling conflicts for both applicants and programs. 31
The impact of cost reduction during AWAE rotations was exemplified in multiple studies on medical students applying to residencies. The research findings revealed a significant decrease in expenses related to away rotations and interviews, primarily attributed to the COVID-19 pandemic.31–33 This unexpected shift to remote learning and assessment allowed students to participate in rotations without incurring the typical financial burdens associated with travel, accommodation, and other related costs. This positive outcome not only relieved the financial strain on medical students but also ensured equitable access to valuable educational opportunities, irrespective of socioeconomic factors.
AWAE rotations offer increased flexibility, enabling medical students to engage in multiple rotations simultaneously. The virtual nature of these rotations eliminates geographical constraints and allows students to participate in programs across different locations without the need for physical relocation. This enhanced flexibility empowers students to broaden their exposure to various medical institutions, specialties, and educational approaches.
Drawbacks
There are downsides to the AWAE model worth mentioning. The student will not get feedback from a patient in the instances of peripheral block placement such as in regional anesthesia or epidural blocks in obstetrics anesthesia. With this procedure, the instructor can lead the student to the correct anatomical landmark, but there is no clinical correlation as a mannequin cannot provide verbal feedback. Additionally, some medical students may be at a disadvantage due to a lack of resources at their home institution. Mannequins that are required to practice procedures such as central line placement, peripheral nerve blocks, and lumbar punctures may be unavailable, and therefore the amount of funding the medical school has can impact the training of medical students in an AWAE rotation. Even with the proper equipment, certain procedures may be more difficult to evaluate remotely as they are more tactile in nature. In addition, there may be obstacles to implementation, such as staff allocation for these programs and equipment not being available even in the student’s home institution.
Besides equipment and resources, another disadvantage of AWAE rotations is the lack of patient interactions. Patient interactions give medical students the opportunity to practice their history-taking and physical examination abilities to identify any factors that may influence the anesthesia management. Although patient interactions can be substituted with role-playing activities, these activities cannot imitate the complexities of real-life patient interactions that help students develop emotional intelligence, account for rare conditions a patient may have, and encounter ethical dilemmas all of which are necessary to improve a medical student’s clinical competence.
AWAE rotations may also be limited in terms of offering the student information about the environment or underpinning of a program. Resources such as residency websites, current residents, and social media platforms may help address these shortcomings. 34 Students may therefore rely on word of mouth, prestige, or anonymous forums to determine their rank list when applying to residency programs (Table 6). Having rotations on a virtual platform rather than in person may also hinder the formation of what would have otherwise been a lasting impression between the program and the student. Although in-person rotations would be preferred by most, AWAE rotations can still provide a promising educational experience and provide medical students the opportunity to impress their programs of interest. A good portion of the knowledge needed for anesthesiology can be provided through lectures or Zoom calls online, and procedural skills can be practiced at the medical student’s home institution under the supervision of attendings at the student’s other program of interest. Despite the downsides, virtual rotations in other specialties such as emergency medicine, intensive care, internal medicine, pediatrics, ophthalmology, obstetrics and gynecology, orthopedic surgery, radiology, plastic surgery, and otolaryngology have provided a positive experience and therefore should be considered in anesthesiology when in-person rotations are not an option.35–38
Evaluation of AWAE residency programs.

Rotation model
During an AWAE rotation, a typical day might involve following a schedule that outlines the student’s responsibilities for the day. This would include attending virtual rounds, participating in virtual patient care activities, and completing virtual assignments. To simulate the experience of working with real patients, the medical student would be given access to virtual patient care activities. These may include virtual patient interviews, virtual patient exams, and virtual patient simulations. The medical student would then be expected to attend virtual rounds with their preceptor and the rest of the healthcare team. Here, they would be able to observe and participate in discussions about patient care and treatment plans. This structure ensures a comprehensive learning experience despite the absence of physical patient interactions.
Didactics
One area where AWAE rotations excel is in the delivery of didactics. Anesthesiology principles, which form a strong foundation of human physiology, are often not extensively covered in medical school core clinical rotations. AWAE rotation lectures can fill this gap by providing valuable information that students may not have access to otherwise. Topics such as different induction and paralytic agents, crucial for rapid sequence intubation in various hospital settings including the operating room, intensive care unit, trauma, and emergency room, are essential in the practice of anesthesia. Additionally, understanding ventilator settings, such as pressure control versus volume control, and the ability to assess a difficult airway have relevance beyond anesthesia practice.
Letters of recommendation
The AWAE rotation can also facilitate obtaining LOR from academic anesthesiologists, as recommended by the ASA. 47 During periods of lockdown, obtaining a LOR from a student’s non-home institution can be challenging. However, AWAE rotations offer a solution by allowing students to establish connections with faculty at the host program of interest, increasing the likelihood of securing strong LOR. A study by Pierre et al. concluded that LOR provide valuable information about applicants and that program directors and assistant program directors favor LOR coming from an anesthesiologist. 39 Furthermore, In 2018, the National Resident Matching Program Director Survey found that the LOR had an importance rating of 4.2 on a five-point Likert scale in inviting an applicant to interview, with one signifying that the LOR did not serve an important purpose and a five signifying that the LOR had a significant role. 40 Although the rotation may be conducted online, certain qualities, such as professionalism, procedural skills, and depth of knowledge, can still be evaluated virtually. These qualities are crucial in a resident, suggesting that the impact of an LOR may not be diminished compared to a letter from an in-person rotation faculty member (Table 7).
Qualities evaluated in AWAE rotations.

Limitations
The study recognizes certain limitations that should be taken into account. Firstly, there is a limited amount of research available specifically on away rotations in anesthesiology. Despite conducting an extensive search using PubMed and EMBASE, the study found only one relevant article, indicating a scarcity of literature on online away rotations in anesthesiology. It is furthermore relevant to note that it includes U.S. National Library of Medicine’s leading database, as well as articles from several other databases. This makes it the largest single database capable of capturing the most studies when conducting a literature review. 48 To address this limitation, articles from other specialties were included to provide additional insights, although these articles may not directly focus on anesthesiology.
Additionally, the potential for publication bias was acknowledged. If studies with non-significant results went unpublished, it could lead to a biased representation of the findings. This bias can impact the overall conclusions drawn from the review and potentially skew the review.
Finally, it is worth noting that our study primarily focused on the benefits and challenges of online away rotations and the use of virtual experiences and interviews. Other factors such as the impact on clinical skills development, patient interactions, and the overall educational experience may need to be explored in future research to provide a more comprehensive understanding of online away rotations in anesthesiology.
Conclusion
During the SARS-COV-2 pandemic, many specialties had to shift their in-person audition rotations to AWAE rotation models. They do offer a new method for programs to evaluate their students subjectively and objectively. In addition, the AWAE rotation is an efficient method that can be invaluable for the student to get to know a program that they would have no exposure to otherwise. Nevertheless, there exist many differences between the AWAE rotation and the traditional in-person audition rotation. Despite AWAE rotations having their limitations, students may be able to decrease the gap between in-person and online anesthesiology rotations. These advancements may help overcome the shortcomings in program exposure and student assessment and can make AWAE rotations practical substitutions for in-person audition rotations if the necessity arises.
Footnotes
Acknowledgements
We wish to thank Vladislav Pavlovich Zhitny, M.D. and Brian J. Mendelson, M.D. for their review of this report. They have provided many constructive comments and suggestions.
Author contribution
All the authors made significant contributions to the final manuscript. Eric Kawana, Benjamin Vachirakorntong, Enes Djesevic, and Michael V. DiCaro were responsible for the writing and revision of the manuscript. Vladislav Pavlovich Zhitny, MD and Brian J. Mendelson both supervised this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Not applicable.
Funding
The author(s) disclosed that this research was self-funded by the authors, and no external funding sources were involved in supporting this research.
Informed consent
Not applicable.