
Abstract
Introduction
Ureteral calculi (UC) is a common and recurrent disease that posed a high risk of complications. It can cause renal colic, hematuria, hydronephrosis and fever, among other symptoms.1,2 UC occurs when kidney stones pass into the ureter and can be classified as upper, middle, or lower stage stones based on their location. 3 Upper UC accounted for about 65% of UC cases. 4 If not eliminated through excretion, UC can continue to grow at the obstructed site, leading to hydronephrosis especially in cases of upper UC. 5 Therefore, timely treatment is critical for preserving normal kidney function.6,7 Current methods used for treating upper UC comprise Extracorporeal Shock Wave Lithotripsy, URSL (Ureteroscopic Holmium Laser Lithotripsy), percutaneous nephrolithotomy, and RLU (Retroperitoneal laparoscopic ureterolithotomy).8–10 However, the recurrence of UC following these surgeries is still a major complication. Metabolic syndrome (MS) is an increasingly common metabolic disorder worldwide. As defined by the National Cholesterol Education Program/Adult Treatment group, MS is diagnosed when an individual presents with at least three out of five specific features 11 : (1) central obesity, defined as a waist circumference of ⩾102 cm in males and ⩾88 cm in females; (2) high triglycerides (⩾150 mg/dL or 1.7 mmol/L) or intake of triglyceride-lowering medication; (3) low high-density lipoprotein (HDL) cholesterol (<40 mg/dL or 1.0 mmol/L in males and <50 mg/dL or 1.3 mmol/L in females) or use of medication for elevated HDL-C; (4) hypertension, defined as systolic blood pressure ⩾130 mmHg or diastolic blood pressure ⩾85 mmHg, or use of hypertensive treatment; and (5) high fasting blood glucose (>100 mg/dL or 5.5 mmol/L) or use of hypoglycemic therapy. Studies have shown a strong association between UC occurrence and various characteristics of MS, such as obesity, hypertension, dyslipidemia, and hyperglycemia.12,13 Recent evidence suggests that MS significantly increases the risk of UC recurrence,14,15 yet few studies have investigated the metabolic factors associated with stone recurrence, particularly in the case of upper UC, which is highly prevalent. Therefore, further investigation was warranted to identify the risk factors associated with ureteral stone recurrence, and thus achieve early detection, and effective treatment of recurring UC.
Patients and methods
The Standards for Reporting of Diagnostic Accuracy (STARD) reporting guideline was used for the reporting of this study. 16
Patient characteristics
For our retrospective study, we enrolled 243 patients who had undergone surgical treatment for unilateral single upper UC in our hospital between January 1, 2016 and December 31, 2018 (Figure 1). These patients were divided into recurrent (R) and non-recurrent (NR) groups based on their history of stone recurrence. Patient demographic information is provided in Table 1. All patients provided written informed consent before enrollment, and ethical approval was obtained from the Ethics Committee of the First Affiliated Hospital of Soochow University.

The process of patient selection. Finally, the information of 243 patients was obtained, including 91 recurrent patients and 152 NR patients.
Comparison of general data between stone recurrence group and non-recurrence group.

BMI normal value = 18.5–23.9. Triglyceride normal value = 0.45–1.69 mmol/L.
HDL normal value = 0.7–2.0 mmol/L.
Inclusion and exclusion criteria
Inclusion criteria
Patients with (1) definite diagnosis of unilateral upper UC; (2) stone diameter ⩾10 mm; (3) underwent surgical treatment with no clinical data missing; and (4) confirmed to be stone-free 1-month after the operation based on a plain film of kidney–ureter–bladder.
Exclusion criteria
Patients who (1) did not meet the inclusion criteria; (2) failed to insert a double J tube; (3) were diagnosed with circulatory system disorders or with severe insufficiency of the heart, liver, or kidney function; (4) had urinary tract tumors and other diseases; and (5) refused to participate in the study.
Treatment management
All patients underwent a thorough preoperative examination upon admission, which included blood test, urine test, electrocardiogram, chest X-ray, abdominal CT (computed tomography), coagulation test, and biochemical analysis. If a patient was diagnosed with urinary tract infection (UTI) before the surgery, they were treated with antibiotics for 1–2 weeks until urinary leukocytes were negative or <++.
URSL was performed as follows: The patient was given general intravenous anesthesia and placed in the lithotomy position. The surgical area was then disinfected. A guide wire was inserted into the ureter through the urethra, and a ureteroscope was subsequently passed over the guide wire to reach the location of the kidney stone. Once in position, the guide wire was replaced with a 200 µm holmium laser optical fiber, and the laser parameters were set at a frequency of 10–15 Hz and an energy of 0.5–1.2 J. The lower end of the stone was vaporized with the holmium laser during lithotripsy. Then, the edge of the stone was targeted, and it was smashed into pieces smaller than 3 mm, which were then removed from the ureter. Following the procedure, an F6 double J tube (Bard, USA) was placed in the location of the eliminated urinary calculus using a guide wire.
The RLU surgery was performed as follows: After general intravenous anesthesia, the patient was positioned laterally with raised hips. The retroperitoneal space was then separated and disinfected. The position of trocar placement was as follows: A 12-mm skin incision was first made at the intersection of a posterior axillary line and the angle between the 12th rib and spinous musculature to open the retroperitoneal space with the help of a balloon dilator. Second, a 5-mm trocar was set 2 cm below the 12th rib tip. Next, 2 cm above the iliac crest at the middle axillary line, the other 12 mm incision was inserted for the camera. An ultrasonic knife was used to provide exposure of the kidney and proximal ureter, followed by an exploration of the positioning of the upper urinary calculus, using curved separation forceps. The ureteral wall was lengthwise cut to an appropriate length with an electrocoagulation hook, and the urinary calculus was removed using non-invasive forceps. Finally, a ureteral stent and a drainage tube were placed at the site where the urinary calculus had been removed and then the ureteral defect was sutured. The day after the operation, the position of the ureteral stent was visualized using abdominal radiography to ensure that it remained in place. Post-operation, all patients received routine nutritional infusion, along with anti-infection and other symptomatic therapies. Two weeks after the operation, the ureteral stent was removed, based on abdominal radiography. Patients were followed up every 3 months for up to a year and every 6 months after the first year until hospital discharge. The retrospective analysis of all patient clinical data aided in determining stone recurrence patterns and related influencing factors.
Postoperative observation and follow-up
After the surgery, patients were provided with a semi-fluid diet starting from the second day, and routine anti-infective treatment was administered. The abdominal plain film was examined to ensure that the stent tube remained in place. Patients were only discharged from the hospital if the urine routine remained negative for 2–3 days after the operation. Follow-up was conducted for all patients for a period of 3–31 months, with a median follow-up time of 15 months. And a survival curve was drawn to show the relationship between MS and recurrence.
Observation index
In this study, several factors were investigated to determine their correlation with stone recurrence. These factors included age, sex, smoking and/or drinking habits, stone laterality, stone diameter, ureteral stricture, stone incarceration, UTI, operation mode, operation time, BMI, and MS. Clinical factors related to recurrence were determined through univariate and multivariate analyses with a p-value of less than 0.05.
Nomogram generation
Using the identified clinical factors related to stone recurrence that were identified through univariate and multivariate analyses, we developed a nomogram to predict the likelihood of stone recurrence in our patients.
Statistical analysis
SPSS 23.0 software (IBM Corp, Armonk, NY, United States), GraphPad Prism 8.0 software (Dotmatics, Boston, United States), and R studio (1.2.1335) (The open source data science company, Boston, United States) were employed for data analyses. Measurement data are presented as (χ ± s). Group differences were analyzed with the Mann–Whitney U test and χ2 test. 17 Multivariate logistic regression analysis was employed to establish discrete risk factors for postoperative UC recurrence. Log-rank analysis was used to analyze differences in the postoperative UC recurrence–time curve between MS and non-MS patients. p < 0.05 was the significance threshold. “STARD” reporting guideline has been used. 16
Results
Univariate analysis of factors related to postoperative stone recurrence
A total of 243 participants (128 men and 115 women) were separated into R and NR cohorts. Patient demographics are described in Table 1. The median follow-up time for all participants was 15 months (range 3–31 months). Based on our analysis, we revealed marked differences in stone diameter, ureteral stricture, stone incarceration, mode of operation, operation time, MS, BMI, triglycerides, diabetes, and HBP between the R and NR cohorts (p < 0.05). Three-point sites (10 mm, 12 mm) were selected via the SPSS 23.0 software and all the patients were separated into three cohorts, depending on the stone diameter: Cohort A: D = 10 mm; Cohort B: 10 mm <D ⩽ 12 mm; and Cohort C: D > 12 mm. As summarized in Table 1, the stone diameter was strongly associated with the recurrence rate. Meanwhile, three-point sites (50 min, 75 min) were selected, using the SPSS 23.0 software, and all the patients were again separated into three cohorts: Cohort I: T ⩽ 50 min, Cohort II: 50 min <T ⩽ 75 min, and Cohort III: and T>75 min. As depicted in Table 1, the length of operation time was closely related to stone recurrence.
Relationship between MS and recurrence
Univariate analysis demonstrated a close relationship between MS and stone recurrence (Table 1). We further employed the χ2 test to analyze the relationship between components of MS and stone recurrence. We revealed that the overall rate of recurrence was higher in the MS patients, relative to non-MS patients (Figure 2, p < 0.0001).
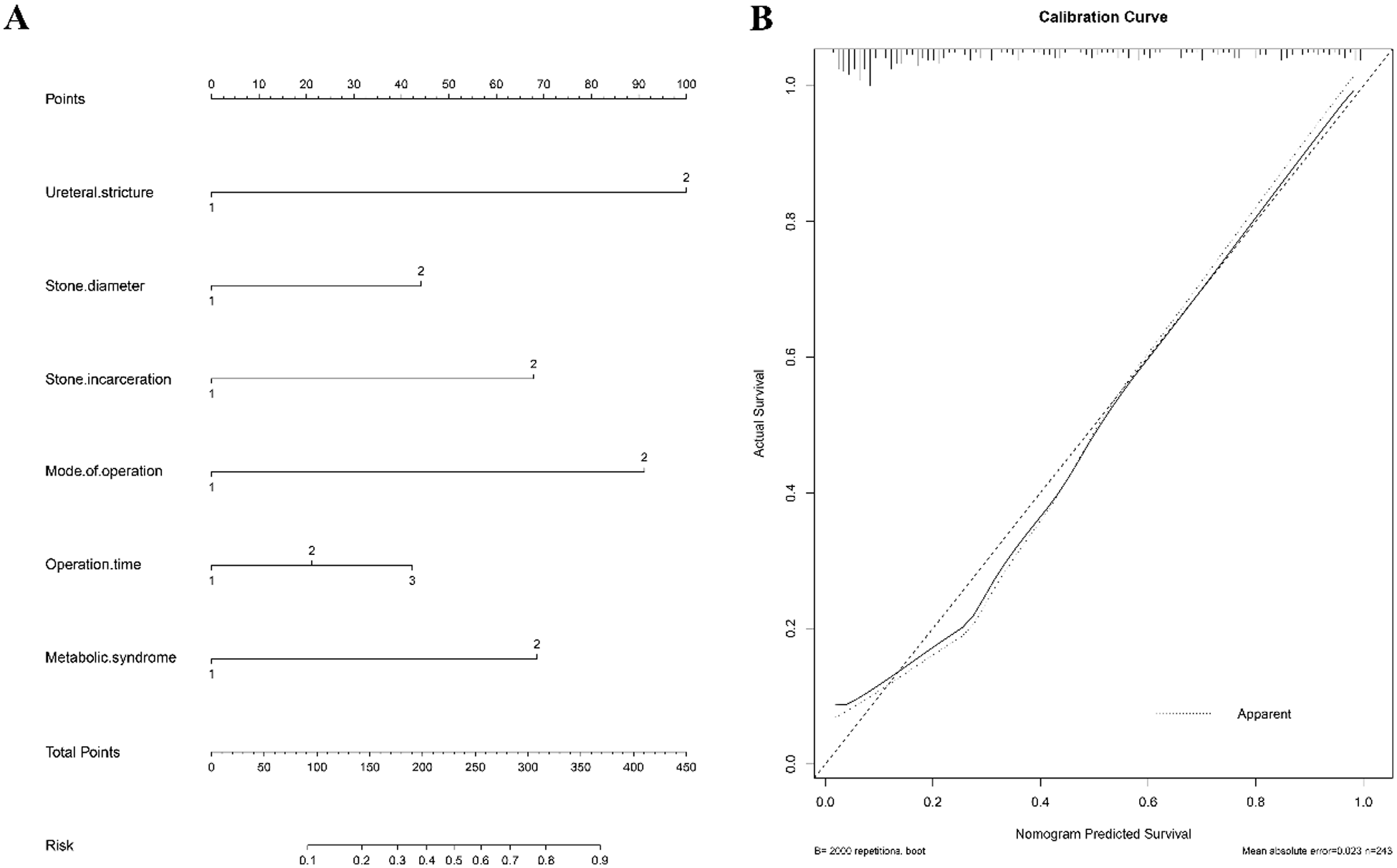
Nomogram predicts recurrence of upper UC. Each variable associated with stone recurrence is located on its axis (A). Draw each vertical line up to the Point axis to determine the number of points for each variable. Add the points of each variable and position it on the total points axis. Draw a vertical line down to find out the probability of clinical stone recurrence. The calibration curve of the nomogram (B). The apparent curve represents the relationship between the predicted probability and the actual probability of clinically significant stone recurrence based on our entire study population. The deviation-corrected curve is drawn by bootstrapping using 1000 resamples. The ideal curve is the 45-inch line, which means a perfect prediction.
Multivariate analysis of ureteral stone recurrence
In further multivariate analysis of influencing factors with statistical differences in univariate analysis, we found that the ureteral stricture, stone diameter, surgical management, and MS were risk factors for stone recurrence (Table 2).
Multivariate analysis of influencing factors of stone recurrence.

Nomogram generation and clinical application
Using data from the stone diameter, ureteral stricture, stone incarceration, surgical intervention (URSL, RLU), operation time, and MS, we constructed a predictive nomogram (Figure 2A). Table 3 lists related feature assignments to help understand the nomogram. The calibration curve revealed the goodness of fit of the nomogram. The 45° dashed line denotes ideal prediction, and the black line denotes the prediction performance of the nomogram (Figure 2B). Generally, the closer the black line is to the ideal prediction line, the better the predictive power of the model. Moreover, the ROC (receiver operating characteristic) curve of the nomogram showed an area under the curve value (AUC) of 0.929 (Figure 3), suggesting high accuracy and effectiveness in the prediction of stone recurrence.
Assignment of related clinical factors.

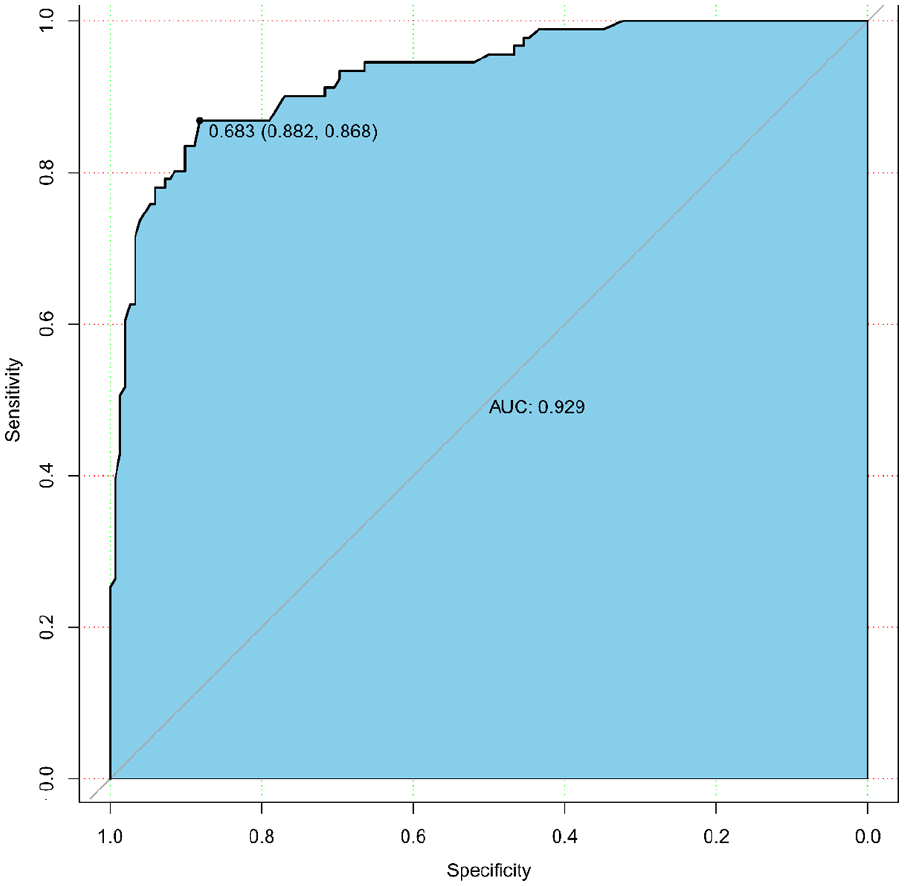
The ROC curve of the nomogram. The AOC is 0.929. It means that the nomogram is more accurate and effective in predicting stone recurrence.
Follow-up observations and the relationship between MS and recurrence
Patients underwent follow-up for 3–31 months, with a median follow-up time of 15 months. No urinary complications except ureteral stricture were observed after the surgery and during follow-ups. Postoperative UC recurrence was identified in 91 cases (37.4%) cases, using either B-ultrasound examination or CT. Since univariate and multivariate analyses demonstrated a close relationship between MS and stone recurrence, a survival curve was drawn and showed that the stone recurrence rate was markedly elevated in MS patients, relative to non-MS patients (p < 0.0001) (Figure 4).

Time curve of postoperative stone recurrence in patients with MS and non-MS. In the MS group, the probability of recurrence-free survival was significantly lower than that in the non-MS group, and there was a significant difference between the two groups (p < 0.0001). With the progress of time, it was found that the probability of recurrence-free survival of the MS group decreased significantly, which was higher than that of the Non-MS group, and the time of recurrence was earlier.
Discussion
Large calculi can get stuck in the ureteral stricture, causing serious obstruction, and resulting in renal dysfunction or hydronephrosis, and, in extreme cases, renal failure. 18 Stone diameter ⩾10 mm is generally treated with URSL, due to the generally small trauma and definite therapeutic outcome. 19 However, the efficacy of URSL for upper UC is only 35%–87%. 20 Advances in urological endoscopic technology have made RLU a viable option for treating UC. Moreover, RLU is also recommended for UC diameter >2 cm, as well as when there is a severe ureteral stricture or when UC co-occurs with pyeloureteral lesions that require simultaneous operation. 21 RLU offers less surgical trauma and faster postoperative recovery. 22 Although URSL and RLU have a significant positive outcome in treating upper UC, postoperative recurrence of upper UC remains a severe challenge facing urologists. Moreover, postoperative recurrence requires reoperation, which brings both surgical pain and economic burden to the patients. Multiple studies have reported postoperative recurrence factors for UC.23,24 But few have reported on the simultaneous comprehensive study of multiple factors, especially the correlation between MS and stone recurrence. Hence, to establish effective measures of recurrent stone prevention, it is essential to explore the risk factors related to stone recurrence.
This study analyzed the correction between recurring stones and a myriad of clinical factors. We revealed that the discrete risk factors for postoperative upper UC recurrence include ureteral stricture, stone diameter, surgical intervention, and MS. From our study, we concluded that patients with preoperative ureteral stricture were remarkably more likely to experience postoperative US recurrence than those without ureteral stricture. This may be due to the fact that the postoperative stone discharge cannot easily be removed from the ureter, and may cause incarceration and calculi adhesion during the removal process, thereby increasing the likelihood of UC formation. Meanwhile, the larger the stone, the more pressure on the ureter, the more likely to form polyps and stenosis. Likewise, we demonstrated that various surgical interventions can affect UC recurrence. RLU, for instance, showed a higher UC recurrence rate than URSL. A possible explanation for this could be that the wound scar is created by RLU, which can cause secondary ureteral stricture, thus increasing the risk of UC formation. Similar to ureteral stricture and surgical intervention, prior studies have demonstrated that the formation and development of UC is closely related to hypertension, hyperlipidemia, hyperglycemia, obesity, and other related metabolic diseases. Moreover, these metabolic disorders can be risk factors for UC.25,26 In addition, there are reports that MS patients are strongly susceptible to forming uric acid stones, compared to non-MS patients. 27
It is important to note that although our study established discrete risk factors for postoperative upper segment UC recurrence, we have not delved into the individual mechanisms behind these relationships. Hence, future studies examining the underlying mechanisms involved in these relationships are highly recommended. The goal of the current study was to analyze the risk factors for upper UC recurrence, and construct a nomogram to effectively predict recurring UC. An accurate prediction of UC recurrence can lead to early detection and early treatment. Our generated nomogram had an AUC value of 0.929, suggesting excellent predictability, and the potential of being used as a reference for UC diagnosis and treatment by clinical urologists.
However, our study has its limitations. First, it is a single-center study. Second, the sample size is not large enough, and this study also lacks research on pediatric data. 28 Third, the follow-up was not long enough. Fourth, power analysis was not done which made our study less convincing. In the future, we will further carry out multi-center, large sample, long-term follow-up performances to verify our findings.
Conclusion
In summary, ureteral stricture, stone diameter, laparoscopic ureterolithotomy, and MS were found to be discrete risk factors for postoperative recurrence of unilateral single US. Among them, MS was the most important risk factor. Given this evidence, the diagnosis and treatment of MS are keys to the prevention of UC recurrence. Detailed assessment and necessary interventions must be undertaken before surgery to aid in the reduction of UC recurrence. Moreover, using a nomogram, we can directly and effectively predict the probability of UC recurrence, which can be widely used in clinical practices.
Footnotes
Acknowledgements
None.
Authors contributions
(I) Conception and design: Zhiyu Zhang; (II) Administrative support: Jun Ouyang, Zhiyu Zhang; (III) Provision of study materials or patients: Qi Zhou; (IV) Collection and assembly of data: Qi Zhou, Zhiyu Zhang; (V) Data analysis and interpretation: Qi Zhou, Zhiyu Zhang; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Suzhou Science and Technology Project (SLJ201906 and SYS2019053).
Ethics approval
The author is responsible for all aspects of the work to ensure that issues related to the accuracy or completeness of any part of the work are properly investigated and resolved. The study is based on the Helsinki Declaration (revised in 2013). The study was approved by the Ethics Committee of the first affiliated Hospital of Soochow University and written informed consent was obtained from all participants. Trial registration: the Ethics Committee of the first affiliated Hospital of Soochow University, No. 119 (2020). Registered 21 October 2020—Retrospectively registered, ![]()
Consent to participate
All authors agree to participate in the submission of the article.
Consent for publication
All authors agree to publish without any conflict of interest.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.